Paper Menu >>
Journal Menu >>
 Vol.2, No.9, 997-1001 (2010) Health doi:10.4236/health.2010.29147 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ Effects of cola intake on fertility: a review Atsushi Imai1*, Satoshi Ichigo2, Hiroshi Takagi2, Kazutoshi Matsunami2, Noriko Suzuki3, Akio Yamamoto3 1Institute of Endocrine-Related Cancer, Matsunami General Hospital, Gifu, Japan; *Corresponding Author: aimai@matsunami-hsp.or.jp 2Department of Obstetrics and Gynecology, Matsunami General Hospital, Gifu, Japan 3Department of Obstetrics and Gynecology, Gifu University School of Medicine, Gifu, Japan Received 22 June 2010; revised 12 July 2010; accepted 14 July 2010. ABSTRACT The consumption of soft drinks has increased considerably during the last decades. Among them, the cola-based preparations are possibly the refreshments with the largest sales world- wide. During the previous years, important concerns have been raised about the effects of colas on human health. In this review, we in- troduce the cola effects on reproduction in- cluding pregnancy miscarriages, ovulatory and menstrual disorders, and reduced semen quality. Although caffeine intoxication may be thought to play the most important role, a component of cola other than caffeine, or in combination with caffeine, may be associated with increased risk of reproductive hazards in heavy cola (> 1 L per day)-consumers. Cola discontinuation usually leads to an uneventful recovery in the most cases suggesting justification of limitations in the maximum recommended daily dose of these soft drinks. Cola is not an essential beverage, and abstaining from drinking more than 1 L per day is a minor intrusion in one’s personal life. Despite these uncertainties, this growing know- ledge may alarm the fertility risk of chronic cola intake in peoples of childbearing age. Keywords: Cola; Soft Drink; Caffeine; Semen; Miscarriage; Ovulation 1. INTRODUCTION The consumption of soft drinks has increased consider- able during the last decades. Among them, the cola- based preparations are possibly the refreshments with the largest sale worldwide. During the previous years, important concerns have been raised about the effects of colas on human health. In addition to the possible detri- mental effects of chronic cola consumption (enamel sof- tening [1,2], bone demineralization [3,4], hypokalemic myopathy [5-7], development of metabolic syndrome and diabetes mellitus [8-10], and chronic kidney dis- eases [11,12]), several lines of evidence suggest that the chronic consumption of large amounts of cola-based soft drinks may increase the risk of reproductive problems such as decreased fetal growth, preterm delivery, and spontaneous abortion [13-16]. However, results from these epidemiological studies suggesting the association between cola consumption and such outcomes have been conflicting and the available information is incomplete and remains controversial. The observations may have important public health implications as, recently, trends of increasing the portion size of these preparations have been noticed. With the aim of evaluating the available epidemiological evidence of the effect of cola consump- tion on reproductive quality (see Table 1), a systematic qualitative review was conductive. 2. PHARMACOLOGICAL EFFECTS OF INGREDIENTS IN COLA Cola contains many different chemical compounds and no certainty exists as to which ones may be associated with disease risk. Cola soft drinks may contain large amounts of glucose (up to 11 g of sugar/dL) and high-fructose corn syrup. Highly caloric carbonated soft drinks are often sweet- ened with high fructose corn syrup, which makes soda inexpensive to produce. While sugary soda may be sold cheaply as a food item and yield a profit, they provide little satiety. Thus, the excessive consumption of theses preparations may lead to glycemic load, resulting in os- motic diuresis and hyperinsulinemia. Fructose itself may cause kidney damage, perhaps mediated by uric acid [17]. Cola contains sufficient amounts of caffeine ranging 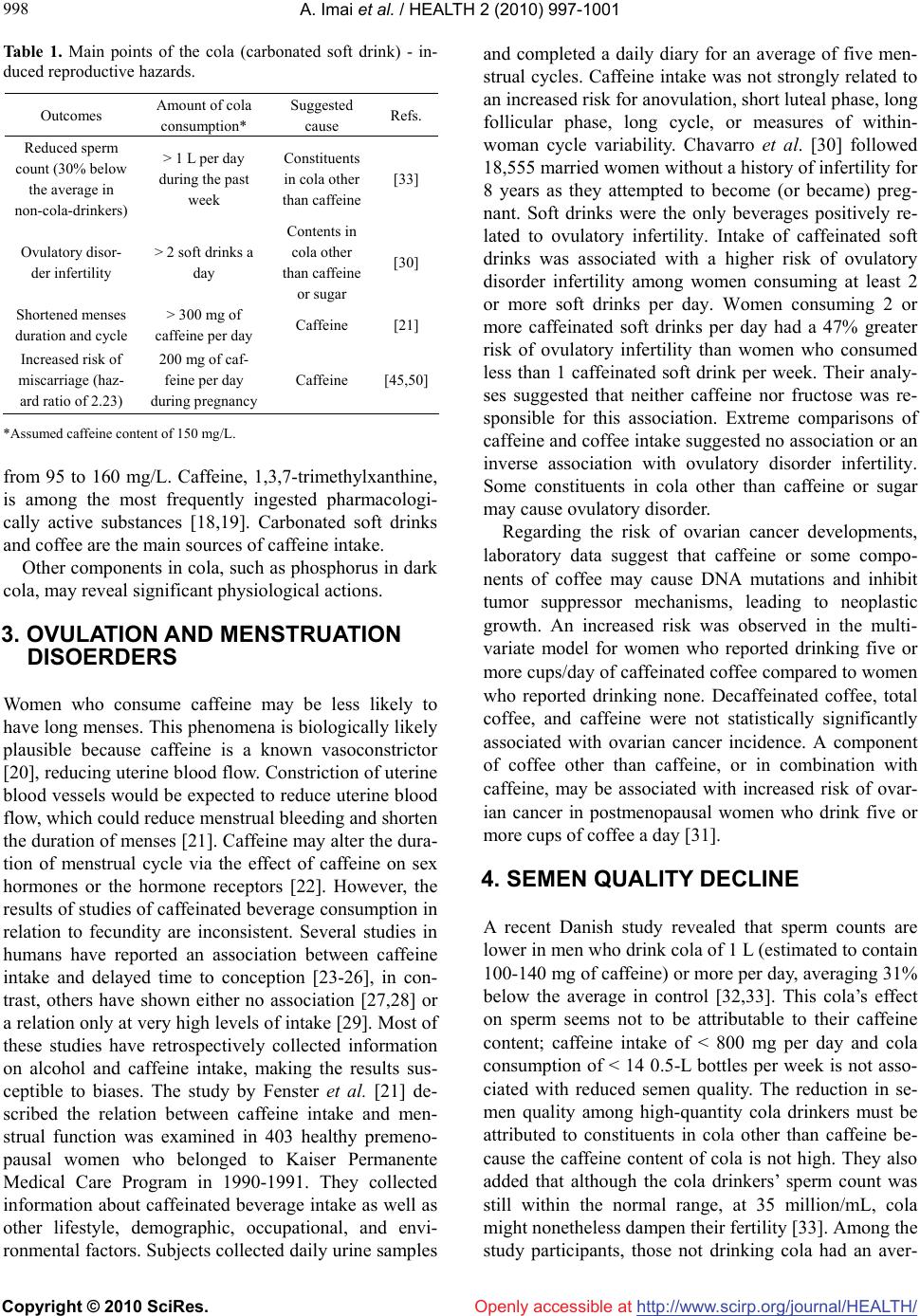 A. Imai et al. / HEALTH 2 (2010) 997-1001 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 998 Table 1. Main points of the cola (carbonated soft drink) - in- duced reproductive hazards. Outcomes Amount of cola consumption* Suggested cause Refs. Reduced sperm count (30% below the average in non-cola-drinkers) > 1 L per day during the past week Constituents in cola other than caffeine [33] Ovulatory disor- der infertility > 2 soft drinks a day Contents in cola other than caffeine or sugar [30] Shortened menses duration and cycle > 300 mg of caffeine per day Caffeine [21] Increased risk of miscarriage (haz- ard ratio of 2.23) 200 mg of caf- feine per day during pregnancy Caffeine [45,50] *Assumed caffeine content of 150 mg/L. from 95 to 160 mg/L. Caffeine, 1,3,7-trimethylxanthine, is among the most frequently ingested pharmacologi- cally active substances [18,19]. Carbonated soft drinks and coffee are the main sources of caffeine intake. Other components in cola, such as phosphorus in dark cola, may reveal significant physiological actions. 3. OVULATION AND MENSTRUATION DISOERDERS Women who consume caffeine may be less likely to have long menses. This phenomena is biologically likely plausible because caffeine is a known vasoconstrictor [20], reducing uterine blood flow. Constriction of uterine blood vessels would be expected to reduce uterine blood flow, which could reduce menstrual bleeding and shorten the duration of menses [21]. Caffeine may alter the dura- tion of menstrual cycle via the effect of caffeine on sex hormones or the hormone receptors [22]. However, the results of studies of caffeinated beverage consumption in relation to fecundity are inconsistent. Several studies in humans have reported an association between caffeine intake and delayed time to conception [23-26], in con- trast, others have shown either no association [27,28] or a relation only at very high levels of intake [29]. Most of these studies have retrospectively collected information on alcohol and caffeine intake, making the results sus- ceptible to biases. The study by Fenster et al. [21] de- scribed the relation between caffeine intake and men- strual function was examined in 403 healthy premeno- pausal women who belonged to Kaiser Permanente Medical Care Program in 1990-1991. They collected information about caffeinated beverage intake as well as other lifestyle, demographic, occupational, and envi- ronmental factors. Subjects collected daily urine samples and completed a daily diary for an average of five men- strual cycles. Caffeine intake was not strongly related to an increased risk for anovulation, short luteal phase, long follicular phase, long cycle, or measures of within- woman cycle variability. Chavarro et al. [30] followed 18,555 married women without a history of infertility for 8 years as they attempted to become (or became) preg- nant. Soft drinks were the only beverages positively re- lated to ovulatory infertility. Intake of caffeinated soft drinks was associated with a higher risk of ovulatory disorder infertility among women consuming at least 2 or more soft drinks per day. Women consuming 2 or more caffeinated soft drinks per day had a 47% greater risk of ovulatory infertility than women who consumed less than 1 caffeinated soft drink per week. Their analy- ses suggested that neither caffeine nor fructose was re- sponsible for this association. Extreme comparisons of caffeine and coffee intake suggested no association or an inverse association with ovulatory disorder infertility. Some constituents in cola other than caffeine or sugar may cause ovulatory disorder. Regarding the risk of ovarian cancer developments, laboratory data suggest that caffeine or some compo- nents of coffee may cause DNA mutations and inhibit tumor suppressor mechanisms, leading to neoplastic growth. An increased risk was observed in the multi- variate model for women who reported drinking five or more cups/day of caffeinated coffee compared to women who reported drinking none. Decaffeinated coffee, total coffee, and caffeine were not statistically significantly associated with ovarian cancer incidence. A component of coffee other than caffeine, or in combination with caffeine, may be associated with increased risk of ovar- ian cancer in postmenopausal women who drink five or more cups of coffee a day [31]. 4. SEMEN QUALITY DECLINE A recent Danish study revealed that sperm counts are lower in men who drink cola of 1 L (estimated to contain 100-140 mg of caffeine) or more per day, averaging 31% below the average in control [32,33]. This cola’s effect on sperm seems not to be attributable to their caffeine content; caffeine intake of < 800 mg per day and cola consumption of < 14 0.5-L bottles per week is not asso- ciated with reduced semen quality. The reduction in se- men quality among high-quantity cola drinkers must be attributed to constituents in cola other than caffeine be- cause the caffeine content of cola is not high. They also added that although the cola drinkers’ sperm count was still within the normal range, at 35 million/mL, cola might nonetheless dampen their fertility [33]. Among the study participants, those not drinking cola had an aver-  A. Imai et al. / HEALTH 2 (2010) 997-1001 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 999 age count of 50 million/mL. In fact, previous studies on caffeine intake and sperm quality have been contradictory [34-36]. Alternatively, these associations may be attributed to the less healthy lifestyle and diet of high-quantity consumers. Heavy quantity consumers of cola or caffeine had an unhealth- ier lifestyle, which has previously been associated with poorer semen quality [37-40]. To the extent possible, many researchers considered these factors in the analy- ses, and they did not appear to explain the caffeine and cola associations. High-quantity caffeine and cola con- sumers also had a less healthy diet, and previous studies have found reduced semen quality among men who consumed few fruits and vegetables and had a low intake of antioxidant and trace minerals [33]. Cola contains sufficient amounts of many minerals including phosph- orus. High cola and caffeine consumption may be related to in utero exposure to caffeine. Ramlau-Hansen et al. [41] studied the association between prenatal coffee and cur- rent caffeine exposure and semen quality. There is a tendency toward decreasing crude median semen volume and adjusted mean testosterone and inhibin concentra- tions with increasing maternal coffee consumption dur- ing pregnancy. Sons of mothers drinking 4-7 cups/day had lower testosterone levels than sons of mothers drinking 0-3 cups/day. However caffeine intake had no impact on semen quality. 5. MISCARRIAGES Caffeine can readily cross the placental barrier to the fetus [42]; its clearance is prolonged in pregnant women, and its metabolism rate is low in the fetus because of low levels of enzymes [43,44]. It may also influence cell development through increasing cellular cyclic adeno- sine monophosphate (cAMP) concentrations and de- crease intervillous placental blood flow via increasing circulating catecholamines [18,19,45]. Caffeine intake during pregnancy has been suggested as a risk factor for adverse reproductive outcomes. Therefore, caffeine could have an adverse effect on fetal development. Indeed, caffeine intake has been reported to increase the risk of miscarriage [15,16,46-48]. Although numerous studies on maternal caffeine consumption and the risk of mis- carriage have been published since the 1980s, the effect of caffeine intake on the risk of miscarriage remains controversial because of methodological limitations in past studies. Many studies have relied on retrospective information, which is subject to recall bias [15,16,46-48]. Some had only a small number of participants, which limited their power to detect an effect. Some did not take into account potential confounding factors such as smok- ing, alcohol consumption, and most importantly, preg- nancy-related symptoms including nausea and vomiting. Some recruited women who sought prenatal care at their 13th to 28th weeks of gestation, therefore too late in pregnancy to study miscarriage. Such controversy has led to the uncertainty about the health effects of caffeine consumption during pregnancy among both clinicians and pregnant women alike. Weng et al. [45] demonstrated, in their prospective cohort study, an elevated risk of miscarriage associated with caffeine consumption during pregnancy and a dose- response relationship with most of the risk associated with caffeine consumption at 200 mg (which approxi- mately 1.5 L cola contains) or greater per day. This ob- served effect was independent of many potential con- founders including pregnancy related symptoms such as nausea, vomiting, and aversion to caffeine consumption. Even among women who never changed caffeine con- sumption pattern during pregnancy, there was an almost 80% increased risk of miscarriage associated with caf- feine consumption of 200 mg/day or greater, although it was not statistically significant because of reduced sam- ple size by stratification. The increased risk of miscar- riage appeared to be due to caffeine itself rather than other possible chemicals in coffee because caffeine in- take from noncoffee sources showed the similarly in- creased risk of miscarriage. On the other hand, a similar cohort study, published same month, by Svavitz et al. [49] demonstrated that this can result in recall bias gen- erating a positive results, whereas when caffeine expo- sure is ascertained before miscarriage, the findings indi- cate no effect of caffeine. To data, the literature is still inconclusive regarding the influence of caffeine on mis- carriage and the available information is incomplete and remains controversial [47,50]. 6. CONCLUSIONS Although much epidemiological work has been con- ducted, results from studies investigating the association between cola consumption and outcomes such as repro- ductive hazards have been conflicting and the available information was incomplete and remained controversial. As summarized in Table 1, our reviewing recent reports suggest the association between cola consumption and increased risk of reproductive hazards. In addition to caffeine, cola contains a number of other chemical com- pounds, and one or more of these could be physiologi- cally active. Further studies might attempt to disentangle a caffeine effect from a noncaffeine effect by comparing different types of beverage drinkers. Cola is not an es- sential beverage, and abstaining from drinking more than 1 L per day is a minor intrusion in one’s personal life.  A. Imai et al. / HEALTH 2 (2010) 997-1001 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1000 The growing knowledge may alarm the fertility risk of chronic cola intake in peoples of childbearing age. Authors contributions: All authors discussed and wrote the draft of the manuscript, and A.I. coordinated the project and wrote the final version. Conflict of interest statement: The authors report no conflicts of interest. REFERENCES [1] Jensdottir, T., Arnadottir, I., Thorsdottir, I. and Holbrook, W.P. (2004) Relationship between dental erosion, soft drink consumption, and gastroesophageal reflux among Icelanders. Clinical Oral Investigation, 8(2), 91-96. [2] Jensdottir, T., Holbrook, P., Nauntofte, B., Buchwald, C. and Bardow, A. (2006) Immediate erosive potential of cola drinks and orange juices. Journal of Dental Research, 85(3), 226-230. [3] Tucker, K. (2009) Osteoporosis prevention and nutrition. Current of Osteoporosis Reports, 7(4), 111-117. [4] Ogur, R., Uysal, B., Ogur, T., Yaman, H., Oztas, E., Oz- demir, A. and Hasde, M. (2007) Evaluation of the effect of cola drinks on bone mineral density and associated factors. Basic and Clinical Pharmacology and Toxicology, 100(5), 334-338. [5] Matsunami, K. and Imai, A. (1994) Hypokalemia in a pregnant woman with long-term heavy cola consumption. International Journal of Gynaecology and Obstetrics, 44(3), 283-284. [6] Tsimihodimos, V., Kakaidi, V. and Elisaf, M. (2009) Cola-induced hypokalaemia: Pathophysiological mecha- nisms and clinical implications. International Journal of Clinical Practice, 63(6), 900-902. [7] Packer, C. (2009) Cola-induced hypokalaemia: A super- sized problem. International Journal of Clinical Practice, 63(6), 833-835. [8] Shoham, D., Durazo-Arvizu, R., Kramer, H., Luke, A., Vupputuri, S., Kshirsagar, A. and Cooper, R.S. (2008) Sugary soda consumption and albuminuria: Results from the National Health and Nutrition Examination Survey, 1999-2004. PLoS One, 3(10), e3431. [9] Assy, N., Nasser, G., Kamayse, I., Nseir, W., Beniashvili, Z., Djibre, A. and Grosovski, M. (2008) Soft drink con- sumption linked with fatty liver in the absence of tradi- tional risk factors. Canadian Journal of Gastroenterology, 22(10), 811-813. [10] Acheson, K. (2005) Caffeine and insulin sensitivity. Metabolic Syndrome & Related Disorders, 3(1), 19-25. [11] Paganini-Hill, A., Kawas, C. and Corrada, M. (2007) Non-alcoholic beverage and caffeine consumption and mortality: The Leisure World Cohort Study. Preventive Medicine, 44(4), 305-310. [12] Saldana, T., Basso, O., Darden, R. and Sandler, D. (2007) Carbonated beverages and chronic kidney disease. Epi- demiology, 18(4), 501-506. [13] Bech, B., Nohr, E., Vaeth, M., Henriksen, T. and Olsen, J. (2005) Coffee and fetal death: A cohort study with pro- spective data. American Journal of Epidemiology, 162(10), 983-990. [14] Parazzini, F., Chatenoud, L., Di Cintio, E., Mezzopane, R., Surace, M., Zanconato, G., Fedele, L. and Benzi, G. (1998) Coffee consumption and risk of hospitalized mis- carriage before 12 weeks of gestation. Human Reproduc- tion, 13(8), 2286-2291. [15] Matijasevich, A., Santos, I. and Barros, F. (2005) Does caffeine consumption during pregnancy increase the risk of fetal mortality? A literature review. Cadernos de Saúde Pública, 21(6), 1676-1684. [16] Signorello, L. and McLaughlin, J. (2004) Maternal caf- feine consumption and spontaneous abortion: A review of the epidemiologic evidence. Epidemiology, 15(2), 229- 239. [17] Johnson, R., Segal, M., Sautin, Y., Nakagawa, T., Feig, D.I., Kang, D.H., Gersch, M.S., Benner, S. and Sánchez-Lozada, L.G. (2007) Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. American Journal of Clinical Nu- trition, 86(4), 899-906. [18] Arnaud, M. (1987) The pharmacology of caffeine. Pro- gress in Drug Research, 31, 273-313. [19] Benowitz, N. (1990) Clinical pharmacology of caffeine. Annual Reviews of Medicine, 41, 277-288. [20] Chou, T. and Benowitz, N. (1994) Caffeine and coffee: Effects on health and cardiovascular disease. Compara- tive Biochemistry & Physiology. Part C, Pharmacology, Toxicology & Endocrinology, 109(2), 173-189. [21] Fenster, L., Quale, C., Waller, K., Windham, G.C., Elkin, E.P., Benowitz, N. and Swan, S.H. (1999) Caffeine con- sumption and menstrual function. American Journal of Epidemiology, 149(6), 550-557. [22] Kitts, D. (1987) Studies on the estrogenic activity of a coffee extract. Journal of Toxicology & Environmental Health, 20(1-2), 37-49. [23] Christianson, R., Oechsli, F. and van den Berg, B. (1989) Caffeinated beverages and decreased fertility. Lancet, 1(8634), 378-379. [24] Grodstein, F., Goldman, M., Ryan, L. and Cramer, D. (1993) Relation of female infertility to consumption of caffeinated beverages. American Journal of Epidemiol- ogy, 137(12), 1353-1360. [25] Stanton, C. and Gray, R. (1995) Effects of caffeine con- sumption on delayed conception. American Journal of Epidemiology, 142(12), 1322-1329. [26] Bolúmar, F., Olsen, J., Rebagliato, M. and Bisanti, L. (1997) Caffeine intake and delayed conception: A Euro- pean multicenter study on infertility and subfecundity. European study group on infertility subfecundity. American Journal of Epidemiology, 145(4), 324-334. [27] Alderete, E., Eskenazi, B. and Sholtz, R. (1995) Effect of cigarette smoking and coffee drinking on time to concep- tion. Epidemiology, 6(4), 403-408. [28] Joesoef, M., Beral, V., Rolfs, R., Aral, S. and Cramer, D. (1990) Are caffeinated beverages risk factors for delayed conception? Lancet, 335(8682), 136-137. [29] Jensen, T., Henriksen, T., Hjollund, N., Scheike, T., Kol- stad, H., Giwercman, A., Ernst, E., Bonde, J.P., Skakke- baek, N.E. and Olsen, J. (1998) Caffeine intake and fe- cundability: A follow-up study among 430 Danish cou- ples planning their first pregnancy. Reproductive Toxi- cology, 12(3), 289-295. [30] Chavarro, J., Rich-Edwards, J., Rosner, B. and Willett, W.  A. Imai et al. / HEALTH 2 (2010) 997-1001 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 1001 (2009) Caffeinated and alcoholic beverage intake in rela- tion to ovulatory disorder infertility. Epidemiology, 20(3), 374-381. [31] Lueth, N., Anderson, K., Harnack, L., Fulkerson, J. and Robien, K. (2008) Coffee and caffeine intake and the risk of ovarian cancer: The Iowa Women’s Health Study. Cancer Causes & Control, 19(10), 1365-1372. [32] Endocrine Society (2010) Sperm and cola don’t mix wee. EndocrineNews, May 2010, 27. [33] Jensen, T., Swan, S., Skakkebaek, N., Rasmussen, S. and Jørgensen, N. (2010) Caffeine intake and semen quality in a population of 2,554 young Danish men. American Journal of Epidemiology, 171(8), 883-891. [34] Vine, M., Setzer, R.J., Everson, R. and Wyrobek, A. (1997) Human sperm morphometry and smoking, caf- feine, and alcohol consumption. Reproductive Toxicology, 11(2-3), 179-184. [35] Marshburn, P., Sloan, C. and Hammond, M. (1989) Se- men quality and association with coffee drinking, ciga- rette smoking, and ethanol consumption. Fertility and Sterility, 52(1), 162-165. [36] (1997) Reproductive toxicology. Caffeine. Environmental Health Perspectives, 105(Suppl. 1), 1279-1280. [37] Jensen, T., Jacobsen, R., Christensen, K., Nielsen, N. and Bostofte, E. (2009) Good semen quality and life expec- tancy: A cohort study of 43,277 men. American Journal of Epidemiology, 170(5), 559-565. [38] Jensen, T., Jørgensen, N., Asklund, C., Carlsen, E., Kris- tensen, T.S., Holm, M. and Skakkebaek, N.E. (2007) Self-rated health and semen quality among 3,457 young Danish men. Fertility and Sterility, 88(5), 1366-1373. [39] Ramlau-Hansen, C., Nohr, E., Thulstrup, A., Bonde, J., Storgaard, L. and Olsen, J. (2007) Is maternal obesity re- lated to semen quality in the male offspring? A pilot study. Human Reproduction, 22(10), 2758-2762. [40] Ramlau-Hansen, C., Thulstrup, A., Storgaard, L., Toft, G., Olsen, J. and Bonde, J. (2007) Is prenatal exposure to tobacco smoking a cause of poor semen quality? A fol- low-up study. American Journal of Epidemiology, 165 (12), 1372-1379. [41] Ramlau-Hansen, C., Thulstrup, A., Bonde, J., Olsen, J. and Bech, B. (2008) Semen quality according to prenatal coffee and present caffeine exposure: Two decades of follow-up of a pregnancy cohort. Human Reproduction, 23(12), 2799-2805. [42] Goldstein, A. and Warren, R. (1962) Passage of caffeine into human gonadal and fetal tissue. Biochemical Phar- macology, 11(2), 166-168. [43] Aldridge, A., Aranda, J. and Neims, A. (1979) Caffeine metabolism in the newborn. Clinical Pharmacology and Therapeutics, 25(4), 447-453. [44] Aldridge, A., Bailey, J. and Neims, A. (1981) The dispo- sition of caffeine during and after pregnancy. Seminars in Perinatology, 5(4), 310-314. [45] Weng, X., Odouli, R. and Li, D. (2008) Maternal caffeine consumption during pregnancy and the risk of miscar- riage: A prospective cohort study. American Journal of Obstetrics and Gynecology, 198(3), e271-e278. [46] Fernandes, O., Sabharwal, M., Smiley, T., Pastuszak, A., Koren, G. and Einarson, T. (1998) Moderate to heavy caffeine consumption during pregnancy and relationship to spontaneous abortion and abnormal fetal growth: A meta-analysis. Reproductive Toxicology, 12(4), 435-444. [47] Signorello, L. and McLaughlin, J. (2008) Caffeine and miscarriage: Case closed? American Journal of Obstet- rics and Gynecology, 199(5), e14-e15. [48] Leviton, A. and Cowan, L. (2002) A review of the litera- ture relating caffeine consumption by women to their risk of reproductive hazards. Food and Chemical Toxicology, 40(9), 1271-1310. [49] Savitz, D., Chan, R., Herring, A., Howards, P. and Hart- mann, K. (2008) Caffeine and miscarriage risk. Epidemi- ology, 19(1), 55-62. [50] Graham, N., Hammond, C.J. and Gold, M. (2008) Caf- feine in miscarriages: It’s not just in the coffee. American Journal of Obstetrics and Gynecology, 199(5), e15. |