U. A. RAHOMA, P. K. CHUNDI 29
system, it can be concluded that the use of CR system is
cost beneficial when compared to film based system.
5. Conclusion
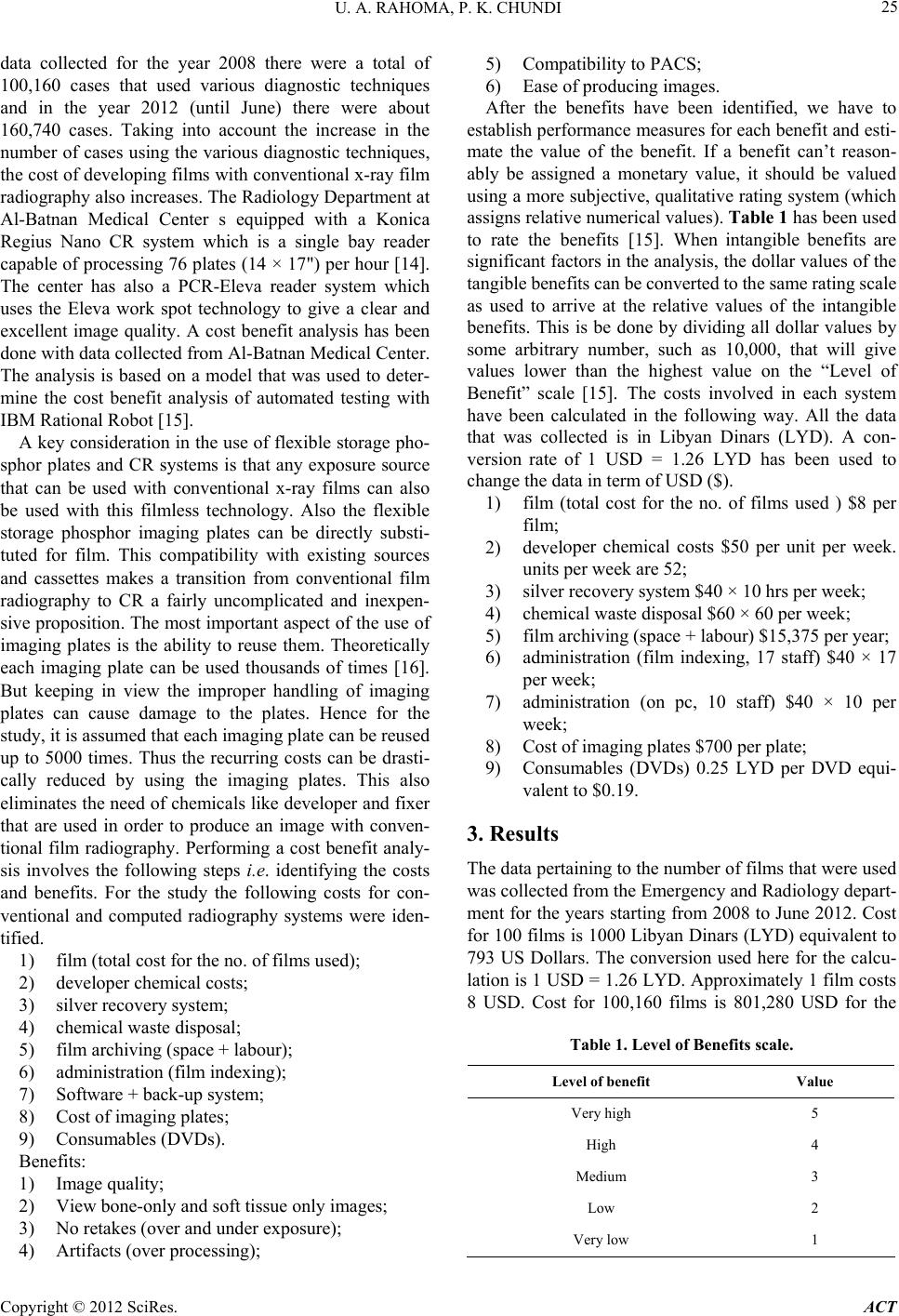
For the years starting from 2008 to 2012, the average
value of the net difference between the costs and benefits
for the conventional film based system is −83.38 where
as for the CR System it is 22.06. Based on the principles
of Cost Benefit Analysis it can be concluded that the
system with a net positive difference is more cost benefi-
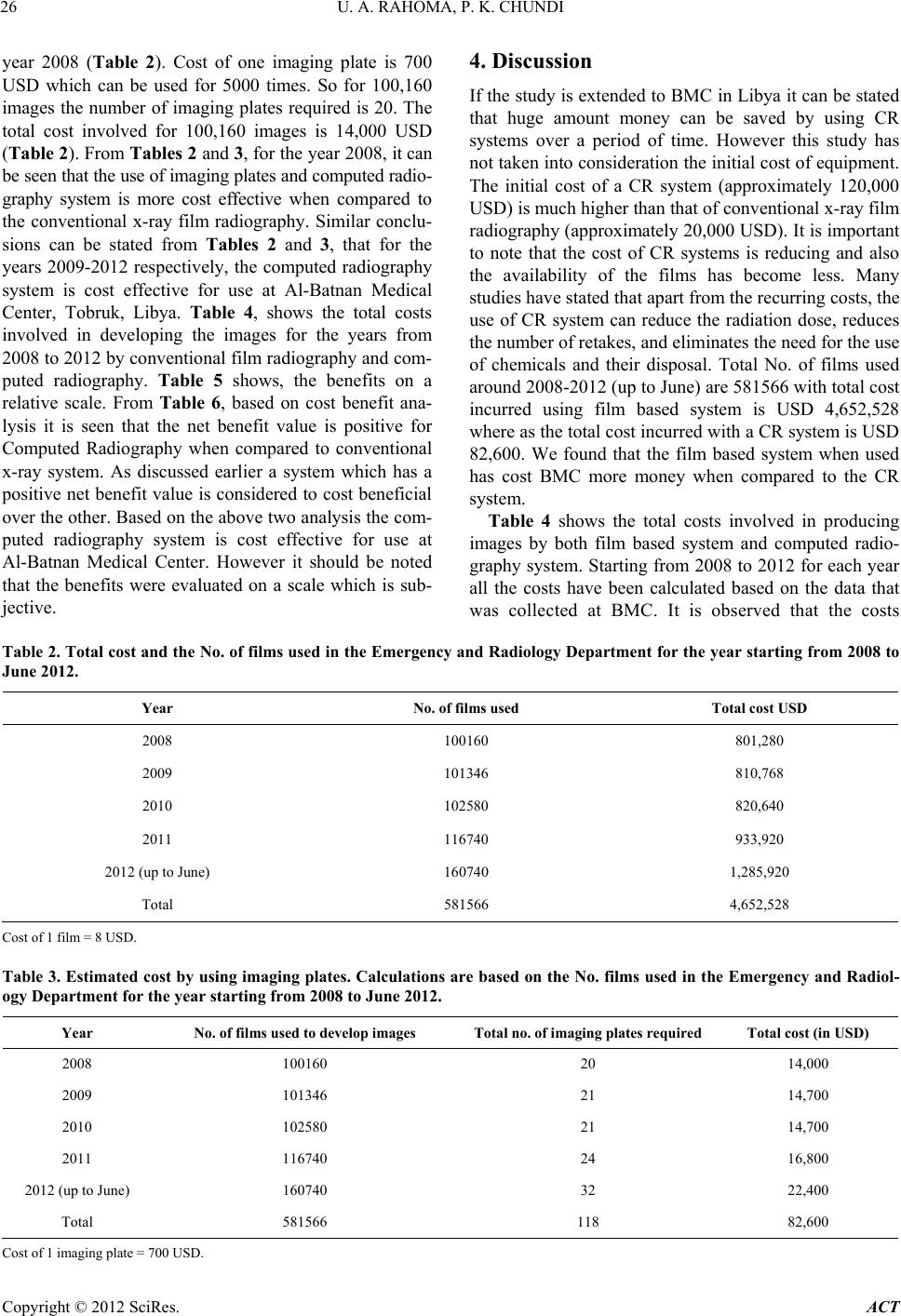
cial than the other. Apart from the initial cost of the CR
System, based on the data collected from the center a
total of 581566 images were produced with the total cost
incurred using film based system being USD 4,652,528.
If the same number of images were produced using a CR
system the total cost incurred would have been USD
82,600. Taking into consideration the cost of a new CR
system to be USD 120,000, the overall cost for producing
the images is USD 202,600. It is observed that an amount
of USD 4,449,928 could have been saved over the period
of 5 years starting from 2008 to 2012 (up to June) by
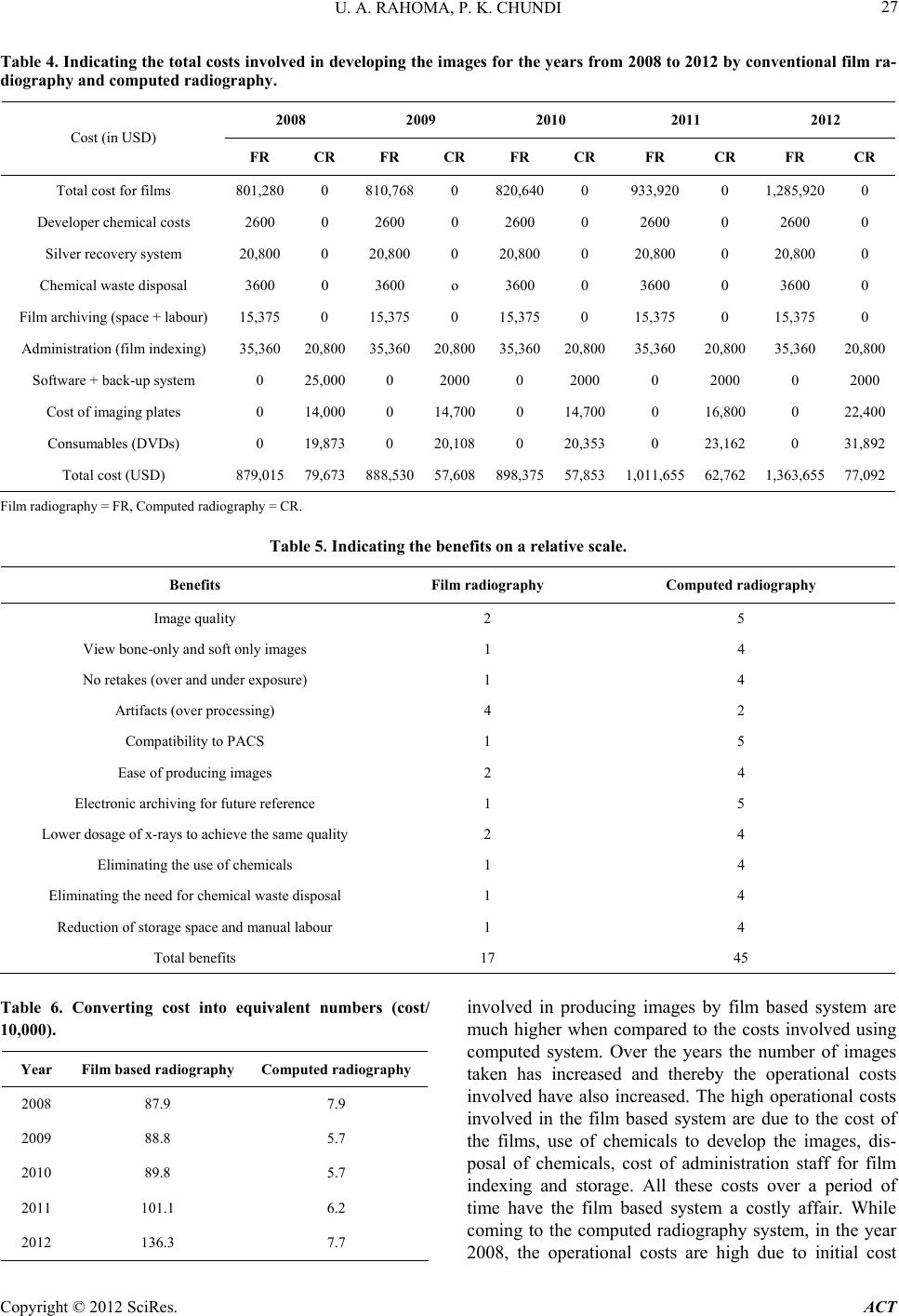
using the CR system at BMC. With the help of the above
two analysis it can be concluded that the use of computed
radiography is definitely more cost effective for use at
BMC, when compared to the conventional x-ray radio-
graphy. Considering the fact that center’s staff is well
trained in using the CR system, it is economical to use
this system with respect to the operational and recurring
costs when compared to the conventional x-ray film ra-
diography.
REFERENCES
[1] G. Roberts and J. Graham, “Computed Radiography,” In:
S. Kraft and G. Roberts, Eds., Modern Diagnostic Imag-
ing, Veterinary Clinics of North America: Equine Prac-
tice, Saunders, Philadelphia, 2001, pp. 47-62.
[2] R. G. Swee, J. E. Gray and J. W. Beabout, “Screen-Film
versus Computed Radiography Imaging of the Hand: A
Direct Comparison,” American Journal of Roentgenology,
Vol. 168, No. 2, 1997, pp. 539-542.
[3] S. Don, C. F. Hildebolt and T. L. Sharp, “Computed Ra-
diography versus Screen Film Radiography: Detection of
Pulmonary Edema in a Rabbit Model that Stimulates
Neonatal Pulmonary Infiltrates,” Radiology, Vol. 213,
1999, pp. 455-460.
[4] R. E. Greene and J. Oestmann, “Computed Digital Radi-
ography in Clinical Practice,” Thieme Medical Publishers,
New York, 1992, pp. 2-46.
[5] J. R. Patel, “Digital Applications of Radiography,” 3rd
Middle East Nondestructive Testing Conference & Exhi-
bition, Manama, 27-30 November 2005, pp. 27-30.
[6] B. Reiner, E. Siegel, T. Mc Laurin, et al., “Evaluation of
Soft-Tissue Foreign Bodies: Comparing Conventional
Plain Film Radiography, Computed Radiography Printed
on Film, and Computed Radiography Displayed on A
Computer Workstation,” American Journal of Roentge-
nology, Vol. 167, No. 1, 1996, pp. 141-144.
[7] S. A. Wegryn, D. W. Piraino, B. J. Richmond, et al.,
“Comparison of Digital and Conventional Musculoske-
letal Radiography: An Observer Performance Study,” Ra-
diology, Vol. 175, No. 1, 1990, pp. 1225-1228.
[8] G. Roberts, “Computed radiography: How It works and
Its Advantages,” The AAEP 2000 Resort Symposium Lec-
ture Workbook, 4-6 February 2000.
[9] P. J. Lund, E. A. Krupinski, S. Pereles and B. Mockbee,
“Comparison of Conventional and Computed Radiogra-
phy: Assessment of Image Quality and Reader Perform-
ance in Skeletal Extremity Trauma,” Academic Radiology,
Vol. 4, No. 8, 1997, pp. 1570-576.
doi:10.1016/S1076-6332(97)80207-3
[10] M. Ogoda, “DICOM 101: Understanding the Basics of
DICOM. Insights & Images,” The User’s Publication of
Computed Radiography, Fujifilm Medical Systems, Stam-
ford, 2001, pp. 2-4.
[11] J. L. Bootman, C. Rowland and A. I. Wertheimer, “Cost-
Benefit Analysis: A Research Tool for Evaluating Inno-
vative Health Programs,” Evaluation & the Health Pro-
fessions, Vol. 2, No. 2, 1979, pp. 129-154.
doi:10.1177/016327877900200202
[12] Z. F. Lu, E. L. Nickoloff, J. C. So and A. K. Dutta, “Com-
parison of Computed Radiography and Film Screen Com-
bination Using a Contrast-Detail Phantom,” Journal of
Applied Clinical Medical Physics, Vol. 4, No. 1, 2003, pp.
91-98. doi:10.1120/1.1524950
[13] Fujifilm, “Advanced Processing Capabilities of FCR,”
2003.
[14] Konica Minolta, “Nano CR Clinic Brochure,” 2007.
[15] K. Micheal, “Using Cost-Benefit Analysis to Compare
Different Test Structures for Rational Robot,” 19 No-
vember 2003.
[16] Siemens Medical, “Computed Radiography System. An
Easy Step from Analog to Digital,” 2006.
Copyright © 2012 SciRes. ACT