Advances in Computed Tomography, 2012, 1, 21-22
http://dx.doi.org/10.4236/act.2012.13005 Published Online December 2012 (http://www.SciRP.org/journal/act)
Re-Sheathing the Scimitar Syndrome
Michael Michail, Kaleab N. Asrress, Abhishek Joshi, John A. Giles,
Muhammed Z. Khawaja, Eric T. McWilliams
Department of Cardiology, Conquest Hospital, Hastings, UK
Email: eric.mcwilliams@gmail.com
Received November 10, 2012; revised December 12, 2012; accep te d Decemb er 20, 2012
ABSTRACT
Scimitar Syndrome is a congenital condition resulting in anomalous pulmonary venous drainage from the lung into the
inferior vena cava. It is often associated with cardiac and pu lmonary abnormalities, both which are determinan ts in the
severity and timing of presentation . True incidence of this condition is un known and likely to be significantly underes-
timated as many patients remain asymptomatic through adult life. The increase in availability and use of medical imag-
ing suggests that more asymptomatic and subacute cases will be detected. The management in those with the delayed
presentation of this co ndition is debated, however the mainstay of therapy remains medical.
Keywords: Adult-Onset Scimitar Syndrome; Multidetector Computed Tomography
1. Case Report
A fifty-year-old lady presented with progressive exer-
tional dyspnoea in absence of significant past medical
history. Clinical examination was normal. Twelve lead
electrocardiograms showed non-specific changes. Bio-
markers including full blood count, cardiac troponin-T,
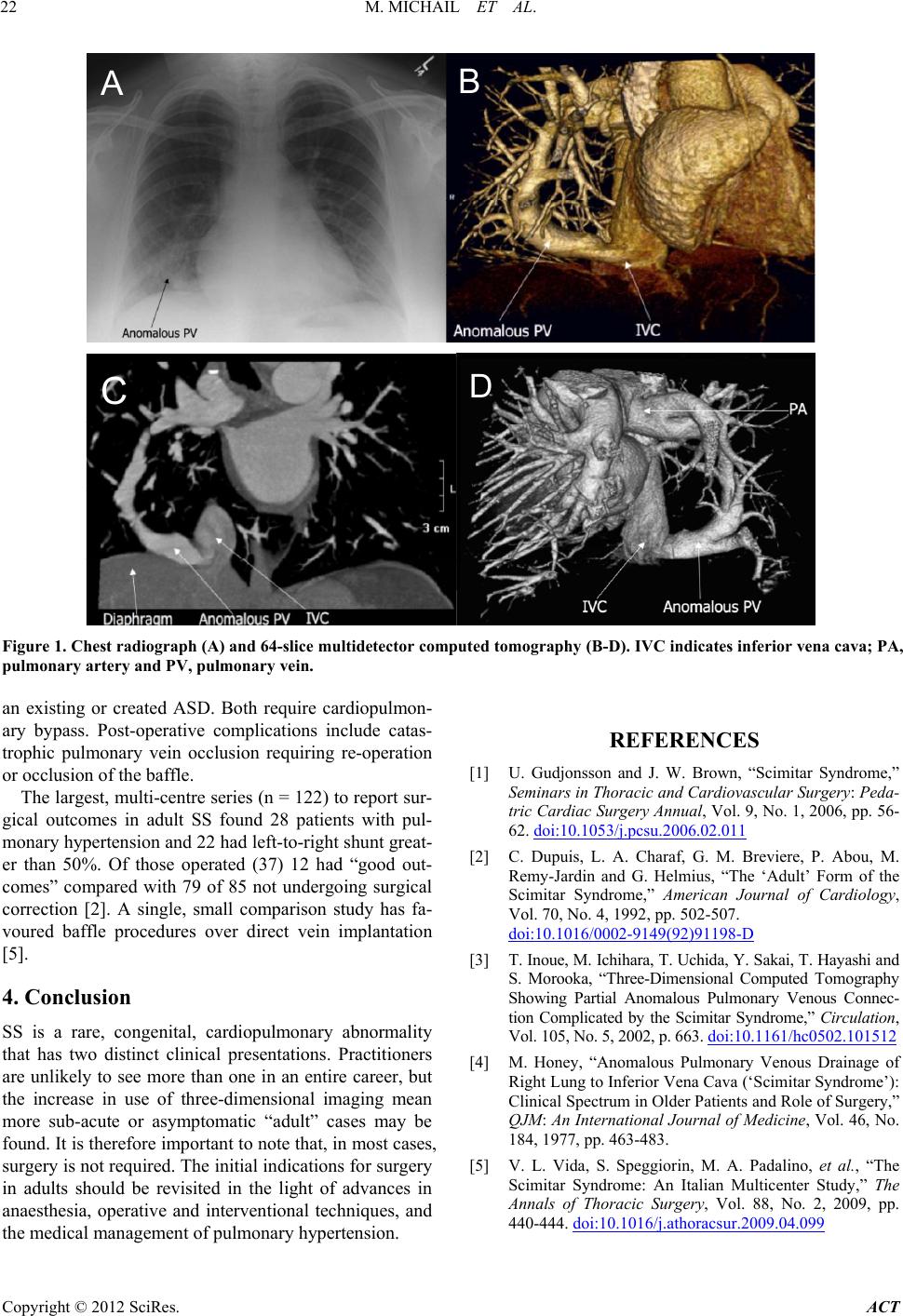
and D-dimers were normal. Plain chest radiograph
showed abnormal vascular markings in the right lower
zone suspicious of a scimitar vein (SV) (Figure 1(A)).
64-slice multidetector computed tomography showed
partial anomalous pulmonary venous drainage of the en-
tire right lung to the inferior vena cava (IVC) below the
right atrial-IVC junction (Figures 1(B)-(D)), confirming
scimitar syndrome (SS). Cardiac catheterisation con-
firmed the presence of the SV, and found a left-to-right
shunt with Qp:Qs of 2.1:1.
2. Scimitar Syndrome
SS is a rare congenital abnormality, characterised by ano-
malous pulmonary venous drainage of the right, or less
frequently, the left lung, into the inferior vena cava. The
true incidence is unknown. The syndrome is named after
the Turkish sword “scimitar” describing the radiogra-
phic appearance of the anomalous vein.
SS has two distinct presentations. The “infant” form is
associated with other congenital abnormalities and great-
er mortality. Clinical features may include failure to
thrive, tachypnoea, cardiac failure, recurrent chest infec-
tions and cyanosis [1]. Medical therapy is used to allevi-
ate symptoms in infants, however the presence of pul-
monary hypertension warrants prompt surgical correc-
tion.
The second form presents in children and adults. Car-
diac and pulmonary abnormalities are associated, the
former more accountable for the severity of symptoms.
Cardiac abnormalities include dextrocardia, atrial and
ventricular septal defects, patent ductus arteriosus and
pulmonary vein stenosis. Pulmonary abnormalities vary
but commonly include right lung hypoplasia and pulmo-
nary sequestration. In two thirds of patients, the SV pro-
vides drainage for the entire right lung.
Delayed presentation in the adult group is the result of
fewer cardiopulmonary anomalies. Patients present with
exertional dyspnoea and recurrent chest infections, more
commonly involving the right lung. Electrocardiogram
may find atrial fibrillation, right ventricular hypertrophy
or right bundle branch block. Pulmonary function tests
demonstrate mild deficits in vital capacity [2]. Co mputed
tomography is increasingly used to provide 3D images to
guide further treatment [3].
3. Treatment
The conventional indications for corrective surgery in
adults with SS are a shunt of greater than 50% (a ratio of
2:1), or pulmonary sequestration with recurrent pulmo-
nary infection. These indications arose from a small, sin-
gle centre study (n = 6) [4].
Corrective surgery attempts to reduce left-to-right
shunt by diverting the flow of SV into systemic circula-
tion. Two main approaches have been used: First, re-im-
pla n t a t io n of th e S V into the le ft atrium or, second, to use
a baffle to redirect flow across the right atrium through
C
opyright © 2012 SciRes. ACT