B. ATANASOVA ET AL.
Conclusion
The present study has added knowledge concerning the ol-
factory hedonic perception in MDD. Using implicit instantane-
ous HR measures, findings revealed that depressed individuals
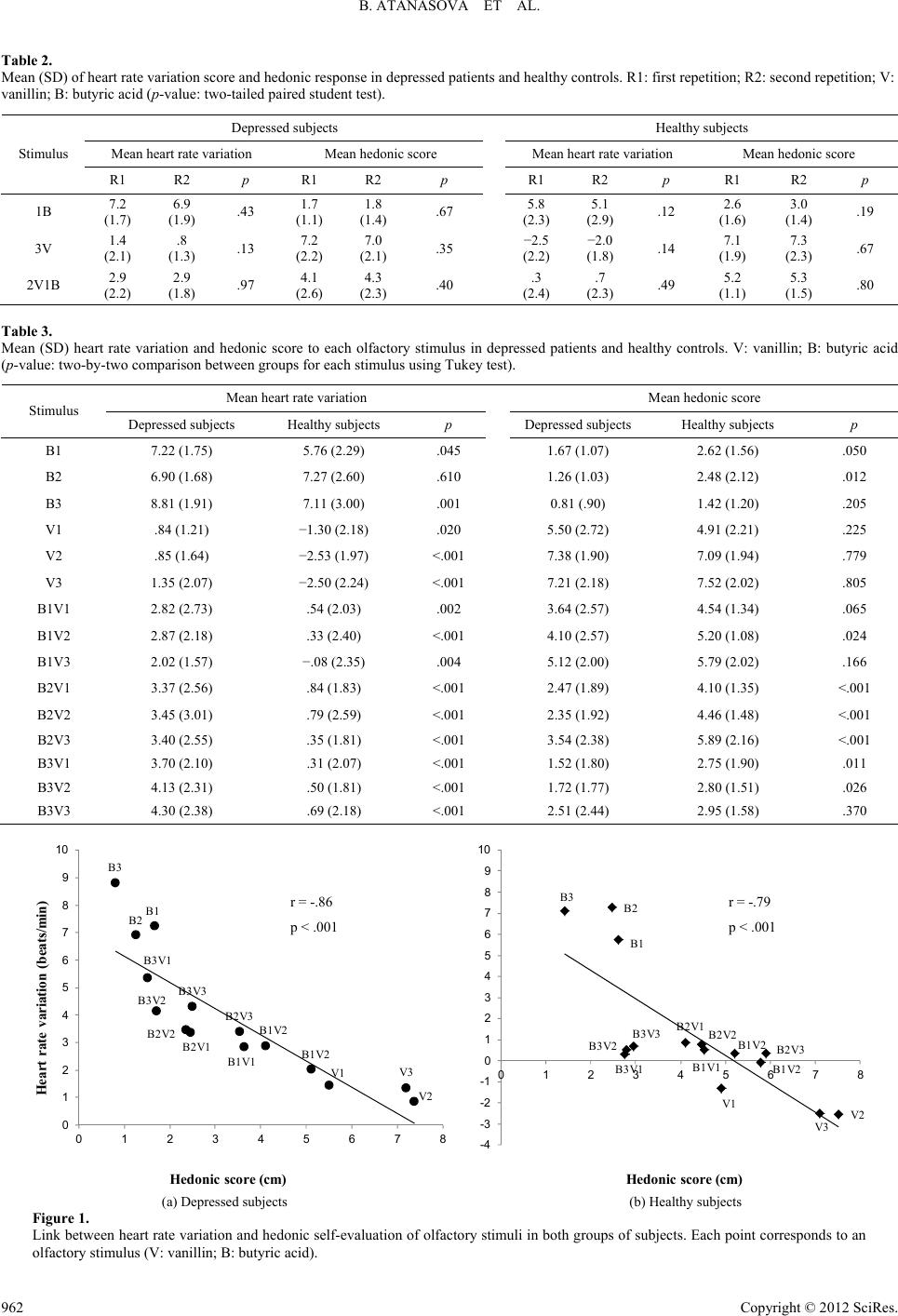
were characterized by increased negative perception of olfac-
tory stimuli whatever their hedonic valence. The results also
suggest that there is a positive attenuation effect specific to
pleasant olfactory stimuli. The results raise the question of
whether the negative bias seen in depressed patients is a direct
result of the clinical condition, or reflects permanent trait ab-
normality. To answer this question, two complementary mea-
surements are required: one before psychiatric treatment, and
one during a follow-up investigation a few months after remis-
sion. A close relationship between the explicit subjective he-
donic response and the implicit instantaneous HR measure was
also observed for both groups, suggesting that these two meth-
ods could be used for olfactory hedonic evaluation.
REFERENCES
Alaoui-Ismaïli, O., Robin, O., Rada, H., Dittmar, A., & Vernet-Maury,
E. (1997a). Basic emotions evoked by odorants: comparison between
autonomic responses and self-evaluation. Physiology & Behavior, 62,
713-720. doi:10.1016/S0031-9384(97)90016-0
Alaoui-Ismaïli, O., Vernet-Maury, E., Dittmar, A., Delhomme, G., &
Chanel, J. (1997b). Odor hedonics: Connection with emotional re-
sponse estimated by autonomic parameters. Chemical Senses, 22,
237-248. doi:10.1093/chemse/22.3.237
American Psychiatric Association (1994). Diagnostic and statistical
manual of mental disorder (4th ed.). Washington DC: American
Psychiatric Association.
Anderson, A. K., Christoff, K., Stappen, I., Panitz, D., Ghahremani, D.
G., Glover, G., Gabrieli, J. D. E., & Sobel, N. (2003). Dissociated
neural representations of intensity and valence in human olfaction.
Nature Neuroscience, 6, 196-202. doi:10.1038/nn1001
Atanasova, B., El-Hage, W., Chabanet, C., Gaillard, P., Belzung, C., &
Camus, V. (2010). Olfactory anhedonia and negative olfactory alli-
esthesia in depressed patients. Psychiatry Research, 176, 190-196.
doi:10.1016/j.psychres.2008.11.016
Bensafi, M., Rouby, C., Farget, V., Bertrand, B., Vigouroux, M., &
Holley, A. (2002a). Influence of affective and cognitive judgments
on autonomic parameters during inhalation of pleasant and un-
pleasant odors in humans. Neuroscience Letters, 319, 162-166.
doi:10.1016/S0304-3940(01)02572-1
Bensafi, M., Rouby, C., Farget, V., Bertrand, B., Vigouroux, M., &
Holley, A. (2002b). Autonomic nervous system responses to odours:
The role of pleasantness and arousal. Chemical Senses, 27, 703-709.
doi:10.1093/chemse/27.8.703
Bensafi, M., Rouby, C., Farget, V., Vigouroux, M., & Holley, A.
(2002). Asymmetry of pleasant vs unpleasant odor processing during
affective judgment in humans. Neuroscience Letters, 328, 309-313.
doi:10.1016/S0304-3940(02)00548-7
Berenbaum, H., & Oltmanns, T. F. (1992). Emotional experience and
expression in schizophrenia and depression. Journal of Abnormal
Psychology, 101, 37-44. doi:10.1037/0021-843X.101.1.37
Bylsma, L. M., Morris, B. H., & Rottenberg, J. (2008). A meta-analysis
of emotional reactivity in major depressive disorder. Clinical Psy-
chology Review, 28, 676-691. doi:10.1016/j.cpr.2007.10.001
Chapman, L. J., Chapman, J. P., & Raulin, M. L. (1976). Scales for
physical and social anhedonia. Journal of Abnormal Psychology, 85,
374-382. doi:10.1037/0021-843X.85.4.374
Clepce, M., Gossler, A., Reich, K., Kornhuber, J., & Thuerauf, N.
(2010). The relation between depression, anhedonia and olfactory
hedonic estimates—A pilot study in major depression. Neuroscience
Letters, 471, 139-143. doi:10.1016/j.neulet.2010.01.027
Cumming, A. G., Matthews, N. L., & Park, S. (2011). Olfactory identi-
fication and preference in bipolar disorder and schizophrenia. Euro-
pean Archives of Psychiatry and Clinical Neuroscience, 261, 251-
259. doi:10.1007/s00406-010-0145-7
Drevets, W. C., Videen, T. O., Price, J. L., Preskorn, S. H., Carmichael,
S. T., & Raichle, M. E. (1992). A functional anatomical study of
unipolar depression. The Journal of Neuroscience: The Official
Journal of the Society f o r N e u r o s c i e nc e , 12, 3628-3641.
Duburcq, A., Blin, P., Charpak, Y., Blachier, C., Allicar, M. P., Bou-
hassira, M., Hergueta, T., & Lecrubier, Y. (1999). Use of a structured
diagnostic interview to identify depressive episodes in an epidemic-
ologic study: A posteriori internal validation. Revue d’épidémiologie
et de santé publique, 47, 455-463.
Ehrlichman, H., & Bastone, L. (1992). Olfaction and emotion. In M.
Serby, & K. L. Chobor (Eds.), Science of olfaction (pp. 410-438).
Springer-Verlag, New York. doi:10.1007/978-1-4612-2836-3_15
Fawcett, J., Clark, D. C., Scheftner, W. A., & Gibbons R. D. (1983).
Assessing anhedonia in psychiatric patients. Archives of General
Psychiatry, 40, 79-84. doi:10.1001/archpsyc.1983.01790010081010
Frye, R. E., Schwartz, B. S., & Doty, R. L. (1990). Dose-related effects
of cigarette smoking on olfactory function. The Journal of the
American Medical Association, 263, 1233-1236.
doi:10.1001/jama.263.9.1233
Gorwood, P. (2008). Neurobiological mechanisms of anhedonia. Dia-
logues in Clinical Neurosc ie n c e , 10, 291-299.
Kaviani, H., Gray, J., Checkley, S., Raven, P., Wilson, G., & Kumari,
V. (2004). Affective modulation of the startle response in depression:
influence of the severity of depression, anhedonia, and anxiety.
Journal of Affective Disor d ers, 83, 21-31.
doi:10.1016/j.jad.2004.04.007
Keedwell, P. A., Andrew, C., Williams, S. C. R., Brammer, M. J., &
Phillips, M. L. (2005). The neural correlates of anhedonia in major
depressive disorder. Biological Psychiatry, 58, 843-853.
doi:10.1016/j.biopsych.2005.05.019
Lehofer, M., Moser, M., Hoehn-Saric, R., McLeod, D., Liebmann, P.,
Drnovsek, B., Egner, S., Hildebrandt, G., & Zapotoczky H. G. (1997).
Major depression and cardiac autonomic control. Biological Psy-
chiatry, 42, 914-919. doi:10.1016/S0006-3223(96)00494-5
Lesser, I. M., Mena, I., Boone, K. B., Miller, B. L., Mehringer, C. M.,
& Wohl, M. (1994). Reduction of cerebral blood flow in older de-
pressed patients. Archives of General Psychiatry, 51, 677-686.
doi:10.1001/archpsyc.1994.03950090009002
Lombion-Pouthier, S., Vandel, P., Nezelof, S., Haffen, E., & Millot, J.
L. (2006). Odor perception in patients with mood disorders. Journal
of Affective Disorders, 90, 187-191. doi:10.1016/j.jad.2005.11.012
Martzke, J. S., Kopala, L. C., & Good, K. P. (1997). Olfactory dysfunc-
tion in neuropsychiatric disorders: Review and methodological con-
siderations. Biological Psychiatry, 42, 721-732.
doi:10.1016/S0006-3223(96)00442-8
Montgomery, S. A., & Asberg, M. (1979). A new depression scale
designed to be sensitive to change. The British Journal of Psychiatry:
The Journal of Mental Science, 1 3 4 , 382-389.
doi:10.1192/bjp.134.4.382
Moskowitz, H. R., Dravnieks, A., & Klarman, L. A. (1976). Odor in-
tensity and pleasantness for a diverse set of odorants. Perception &
Psychophysics, 19, 122-128. doi:10.3758/BF03204173
Pause, B. M., Raack, N., Sojka, B., Göder, R., Aldenhoff, J. B., &
Ferstl, R. (2003). Convergent and divergent effects of odors and
emotions in depression. Psychophysiology, 40, 209-225.
doi:10.1111/1469-8986.00023
Pause, B. M., Miranda, A., Göder, R., Aldenhoff, J. B., & Ferstl, R.
(2001). Reduced olfactory performance in patients with major de-
pression. Journal o f Psychiatric Research, 35, 271-277.
doi:10.1016/S0022-3956(01)00029-2
Siegle, G., Granholm, E., Ingram, R. E., & Matt, G. E. (2001). Pupil-
lary and reaction time measures of sustained processing of negative
information in depression. Biological Psychiatry, 49, 624-636.
doi:10.1016/S0006-3223(00)01024-6
Sloan, D. M., Strauss, M. E., Quirk, S. W., & Sajatovic, M. (1997).
Subjective and expressive emotional responses in depression. Jour-
nal of Affective Disorders, 46, 135-141.
doi:10.1016/S0165-0327(97)00097-9
Sloan, D. M., & Sandt, A. R. (2010). Depressed mood and emotional
Copyright © 2012 SciRes.
964