 Open Journal of Ophthalmology, 2012, 2, 131-139 http://dx.doi.org/10.4236/ojoph.2012.24029 Published Online November 2012 (http://www.SciRP.org/journal/ojoph) 131 Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children Mehul A. Shah, Shreya M. Shah, Khushboo A. Shikhangi, Pramod R. Upadhyay, Geetopam B. Bardoloi Drashti Netralaya, Dahod, India. Email: omtrust@rdiffmail.com Received August 8th, 2012; revised September 14th, 2012; accepted October 30th, 2012 ABSTRACT Purpose: To assess treatment results in pediatric patients with cataracts, to evaluate the efficacy of various surgical interventions, and to determine the factors that affect visual outcomes. Methods: This is aProspective cohort study. We studied a consecutive series of pediatric patients with congenital, developing, or traumatic cataracts who underwent surgery between January, 1999 and April, 2012 at Drashti Netralaya, Dahod. Patient demographics, cataract type, presenting symptoms, surgical intervention, postoperative visual acuity, and follow-up refractive changes were recorded. Results: In total, 1305 eyes of 1047 children were included: unilateral cataracts were present in 786 (60.2%) eyes. There were 610 (46.7%) traumatic and 695 (53.3%) non-traumatic cases. Ages at surgery ranged from 1 to 215 months. Eyes were grouped by the surgical intervention performed: Group 1, pars plana approach including 366 (28%) eyes that underwent lensectomies, and Group 2, anterior approach, including 939 (71.9%) eyes that underwent phacoemulsifi- cation ± IOL placement or small incision cataract surgery ±IOL placement. The mean follow-up time was 117 days. Ultimately, 113 (30.9%) Group 1 and 503 (53.6%) Group 2 patients achieved a visual acuity better than 20/60 (P < 0.001). Age at intervention, laterality, sensory nystagmus, pre-treatment vision, IOL insertion, and etiology were all significantly related (all P < 0.001) to visual outcome. Conclusions: Surgical treatment with intraocular lens implanta- tion for children with congenital, developmental, or traumatic cataracts is an effective treatment for visual rehabilitation. Visual outcome was significantly better in cases of traumatic cataracts versus non-traumatic cataracts. Keywords: Pediatric Cataract; Visual Outcome; Traumatic Cataract; Developmental Cataract; Congenital Cataract 1. Introduction Childhood cataracts are responsible for 5% - 20% of blindness in children worldwide and for an even higher percentage of childhood visual impairment in developing countries [1-5]. The overall incidence of clinically sig- nificant cataracts (unilateral or bilateral) in childhood is unknown, but has been estimated to be as high as 0.4% [6,7]. The prevalence of childhood cataract varies from 1.2 to 6.0 cases per 10,000 infants. Pediatric cataracts are responsible for more than one million cases of childhood blindness in Asia. In developing countries, such as India, 7.4% - 15.3% of childhood blindness is due to cataracts [8,9]. Internationally, the incidence is unknown. Although the World Health Organization and other health organi- zations have made outstanding progress in vaccination and disease prevention, the rate of congenital cataracts re- mains much higher in underdeveloped countries. The visual results of cataract surgery in children have generally [10-12] been poorer than in adults [1-3, 6,12,13]. This difference is due, in part, to the various types of amblyopia that develop in children with cata- racts, the association of nystagmus with early onset cata- racts, and the presence of other ocular abnormalities that adversely affect vision in eyes with developmental lens opacities. Since the introduction of the aspiration tech- nique for cataract removal by Scheie in 1960 [14], surgi- cal procedures for the removal of the lens in childhood have improved [15,16], and earlier surgery for congenital cataracts has been encouraged [17-19]. Any opacification of the lens and its capsule in chil- dren is defined as a pediatric cataract. Pediatric cataracts can be unilateral or bilateral. They can be subdivided based on morphology, as well as etiology. Morphologi- cally, the most common type of pediatric cataract is the zonular cataract, characterized by opacification of a dis- crete region of the lens. This type includes nuclear, la- mellar, sutural, and capsular cataracts [6,10]. Polar cataracts are opacities of the subcapsular cortex in the polar regions of the lens. Almost all (90%) anterior polar cataracts are unilateral; bilateral anterior polar cata- racts are commonly asymmetric and typically do not progress over time. Posterior polar cataracts are often Copyright © 2012 SciRes. OJOph  Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children 132 small, but even a small posterior polar cataract can im- pair vision. A distinctive type of posterior polar cataract is the posterior lentiglobus or lenticonus, in which a pro- trusion of the posterior capsule is present. Membranous cataracts form when the lens, cortex, and nucleus are par- tially or completely reabsorbed, leaving a small amount of opacified lens material between the anterior and the posterior lens capsules (Duke-Elder, 1972). Congenital cataracts are one of the most common causes of treatable blindness in children, particularly in developing countries [1]. A recent report indicated that infants with bilateral congenital cataract who underwent early surgery (within 1 month of birth) and received ap- propriate optical rehabilitation could obtain visual acuity of better than 0.4 and could even achieve stereopsis [2]. However, because of typically relatively late detection and diagnosis, the nonavailability of facilities for infant anesthesia, and poor compliance with long-term follow- up, the visual prognosis for infants with congenital cata- ract in developing countries differs markedly from that in industrialized countries. Visual loss is primarily attribu- table to amblyopia, most importantly, to “stimulus-form deprivation amblyopia,” with the additional factor of ocu- lar rivalry in unilateral disease. Thus, improved under- standing of the critical periods of visual development has resulted in to surgical intervention for dense cataracts being deemed necessary within the first 3 months of life, possibly as early as the first 6 weeks in unilateral disease. Clinical factors believed to be important to visual out- come in children include age at diagnosis and surgery, type of refractive correction, type of cataract surgery, compliance with occlusion regimen, etiology of the cata- ract, presence of non-ophthalmic disorders, development of capsular opacity or secondary membrane, and serious ocular postoperative complications. Primary posterior capsulotomy and anterior vitrectomy are considered “routine surgical steps,” especially in younger children. Previously, preparation for secondary intraocular lens (IOL) implantation at a later date was not considered. However, widespread acceptance of IOL im- plantation in children has caused this to be revised. Thus, management of the posterior capsule should eliminate or delay the formation of visual axis opacity and yet leave sufficient capsular support to achieve the desired “in- the-bag” (or ciliary sulcus) fixation of an IOL. Even when IOL implantation is not performed with the pri- mary procedure, it is important to treat and prepare the eye in such a way that secondary implantation can be achieved subsequently. 2. Materials and Methods The study was approved by the hospital ethics committee. This was a prospective hospital-based study at a tertiary care eye hospital in western India over 20 years, from January, 1992 to April, 2012. All pediatric patients (0 to 18) with cataracts presenting to our department during this period were enrolled in the study. Patient primary details and history were documented using a pre-tested online format. Ocular trauma details were documented with an online world eye injury regis- try form. Vision was checked according to the American Aca- demy of Pediatrics vision check protocol. Both eyes were assessed. Anterior segment examinations were conduc- ted using a slit lamp bio-microscope. The pupils were dilated. Ocular pressure was measured using a Perkin’s hand- held tonometer. If this was not possible, the pressure was measured under general anesthesia. This procedure was omitted for eyes with open globe injuries. The posterior segment of the eye was evaluated with the help of an indirect ophthalmoscope and a +20 D lens and an ultra- sound “B” scan if the media was not clear. The surgical technique was decided based on etiology, cataract morphology, and the position of the lens. Sur- gery was done by the anterior or pars plana route. Ante- rior route surgeries were performed using a phacoemulsi- fier or manual suction. Membranectomies and lensecto- mies were performed using a pneumatic cutter leaving capsular support for secondary implant. Intraocular lenses were not implanted in patients younger than 1.5 years. Children below this age underwent lensectomies/mem- branectomies; secondary implant placement was conduc- ted later. Patients were rehabilitated using glasses or con- tact lenses in-between. For IOL power calculations, we followed published guidelines [20,21]. In cases of globe rupture, open globe injury wound repair was done as a first stage and the cataract was ope- rated on at a second sitting. All steps of the surgical techniques were documented using a pretested online format. All traumatic cataract patients without infection were treated with systemic corticosteroids. In all patients with inflammation and membranous cataracts, a primary pos- terior capsulotomy and anterior vitrectomy were per- formed. Postoperative follow-up was performed according to a pretested online format, including vision, anterior and posterior segment findings and intra ocular pressure, over an appropriate follow-up schedule. Glasses were pre- scribed when the media were clear and the final prescrip- tion was at 6 weeks post-operation. Patients underwent orthoptic evaluations and amblyopic patients were treated with appropriate patching. Aphakic patients were reha- bilitated using glasses or contact lenses. Patients were evaluated for stereopsis and contrast sensitivity using a Titmus vision tester or a Titmus fly test. Copyright © 2012 SciRes. OJOph  Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children 133 Patients developing later cataracts underwent mem- branectomies and vitrectomies as required. For children operated on below the age of 1.5 years, secondary lens implantation was performed after they reached 1.5 years of age. Data were analyzed using the SPSS software (ver. 19.0; SPSS Inc., Chicago, IL, USA). Univariate parametrical analyses were used. A P-value of <0.05 was considered to indicate statistical significance. 3. Results The enrolled patient group consisted of 1305 eyes in 805 pediatric patients with cataracts. There were 858 (65.7%) males and 447 (34.3%) females (Table 1). The mean patient age was 9.5 ± 4.7 years (range, 0 - 18). Of the cataracts, 610 (46.7%) were traumatic and 695 (53.3%) were congenital or developmental. Of the eyes, 1117 (85.6%; Table 2) had diminished vision and 188 (14.4%) presented with leukocoria. The follow-up period was 1 - 3084 days (mean, 117.4 days). In the non-traumatic group, eyes were further subdi- vided into congenital (293, 22.5%), developmental (373, 28.6%), and secondary cataracts (29, 2.2%; Tables 2 and 3). According to the statistical analysis, the demographic factors analyzed, including socioeconomic status (74.5% were of lower socioeconomic status) and residence (92% were from rural areas), had no significant relationship with the final visual acuity. Regarding patient entry, 9.2% of the patients had re- ceived primary treatment prior to reaching our center; this was not associated with a significant difference in the final visual outcome (P = 0.2). Of the total patients enrolled, 26.4% entered via an outreach department, and 71% were self-referred. Among the injuries, 30% were reported within the first 24 h, 30% were reported within 3 days, and 33.9% were reported within 1 month. A wooden stick was the most common object causing eye injury (51.4%). Neither the injury-causing object (P = 0.3) nor the activity at the time of injury (P = 0.3) was significantly associated with the final visual acuity. A comparison of pre- and post-operative visual acui- ties showed that treatment significantly improved visual acuity (Tabl e 4; P < 0.001, Pearson’s χ2 test; P = 0.001, ANOVA). An intraocular lens was implanted in 1205 cases (92.3%) and was significantly associated with im- proved visual acuity (P < 0.001). When we compared visual outcome between the trau- matic and non-traumatic groups, the traumatic group did significantly better (Table 5; P < 0.001). Final visual acuity following cataract surgery was > 6/60 in 399 eyes (56.8%) and ≥6/12 in 105 eyes (15.1%) in the non-trau- matic group. In the traumatic group, the visual acuity Table 1. Age and sex distribution. Sex Age (Years) Female Male 0 to 2 37 56 3 to 5 67 119 6 to 10 156 293 11 to 18 187 390 Total 447 858 Table 2. Aetiology of cataract. Type of Cataract Frequency Percent Complicated 29 2.2 Congenital 293 22.5 Developmental 373 28.6 Traumatic 610 46.7 Total 1305 100.0 was >6/60 in 333 eyes (54.6%) and ≥6/12 in 193 eyes (31.6%). The difference between the groups was signifi- cant (P < 0.001). In total, 296 (22.6%) eyes had a final visual acuity ≥6/12 and 728 (57.8%) eyes had a final visual acuity >6/60 (Table 5). Sensory nystagmus was present in 221 (17%) eyes. This caused a significant difference in final visual out- come (Table 6; P < 0.001). We examined unilateral versus bilateral cataracts (Ta- ble 7; P < 0.001) and found better results in unilateral cases. In the non-traumatic group, bilateral cases had better results (Table 7; P < 0.001). We compared visual outcome according to age of in- tervention. Significantly better results were achieved in the age range between 6 and 18, likely because of the traumatic cases in this age group (Table 8; P < 0.001). We compared final visual outcome between the anterior and pars plana routes. An anterior approach resulted in a better outcome (Table 9; P < 0.001). We also studied visual outcome when a primary poste- rior capsulotomy and vitrectomy were performed. Pri- mary posterior capsulotomy and vitrectomy were per- formed in 460 (34.5%) cases and a significant difference was found (Table 1 0; P < 0.001). Better overall results were achieved if a primary posterior capsulotomy and vitrectomy were not performed, while vision was im- proved in cases of traumatic cataracts (Table 10; P = 0.008). Insertion of an IOL resulted in a significant improve- ent in visual outcome. (Table 11; P < 0.001). m Copyright © 2012 SciRes. OJOph  Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children Copyright © 2012 SciRes. OJOph 134 Table 3. Comparision of visual outcome according to aetiology. Type of Cataract Visual Acuity Complicated Congenital Developmental Traumatic Uncooperative 0 9 6 5 <1/60 20 66 66 201 1/60 to 3/60 3 61 65 69 6/60 to 6/36 2 17 50 46 6/24 to 6/18 3 128 92 94 6/12 to 6/9 0 5 30 53 6/6 to 6/5 1 5 62 140 Total 29 291 371 608 P = 0.0001299. Table 4. Comparision of visual outcome according to pre operative visual acuity. Visual Acuity (Preoperative) Visual Acuity (Post OP) Uncooperative <1/60 1/60 to 3/60 6/60 to 6/36 6/24 to 6/18 6/12 to 6/6 6/9 to 6/6 Uncooperative 7 13 0 0 0 0 0 <1/60 7 321 11 11 3 1 0 1/60 to 3/60 1 128 54 11 5 0 0 6/60 to 6/36 0 74 28 10 3 0 0 6/24 to 6/18 7 132 37 99 41 0 2 6/12 to 6/9 1 62 15 3 7 1 0 6/6 to 6/5 5 140 24 23 12 3 3 Total 28 870 169 157 71 5 5 P = 0.000. Table 5. Comparision of visual outcome amongst traumatic and non traumatic group. Cataract Visual Acuity Non Traumatic Traumatic Uncooperative 15 5 <1/60 153 201 1/60 to 3/60 130 69 6/60 to 6/36 70 46 6/24 to 6/18 224 94 6/12 to 6/9 36 53 6/6 to 6/5 69 140 Total 697 608 P = 0.000. Table 6. Comparision of visual outcome according to pre- sence of sensory nystegmus. Sensory_Nystagmus Visual Acuity No Yes Uncooperative 13 7 <1/60 302 52 1/60 to 3/60 150 49 6/60 to 6/36 96 20 6/24 to 6/18 230 88 6/12 to 6/9 88 1 6/6 to 6/5 204 5 Total 1083 222 P = 0.000.  Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children 135 Table 7. Comparision of visual outcome according to lateri- lity. Laterality Visual Acuity Bilateral Unilateral Uncooperative 8 12 <1/60 75 278 1/60 to 3/60 98 100 6/60 to 6/36 58 57 6/24 to 6/18 187 130 6/12 to 6/9 28 60 6/6 to 6/5 59 149 Total 513 786 P = 0.000. Table 8. Comparision of visual outcome according to age of intervention. Cataract Age (yrs) Visual Acuity 0 to 2 3 to 5 6 to 10 11 to 18 Uncooperative 1 6 12 1 <1/60 5 58 130 160 1/60 to 3/60 3 26 67 102 6/60 to 6/36 0 11 50 54 6/24 to 6/18 81 75 88 73 6/12 to 6/9 0 3 39 46 6/6 to 6/5 2 5 62 139 Total 92 184 448 575 P = 0.000. Table 9. Comparision of visual outcome according to surgi- cal approach. Surgical Approach Visual Acuity A P Uncooperative 10 10 <1/60 194 160 1/60 to 3/60 140 59 6/60 to 6/36 92 24 6/24 to 6/18 230 88 6/12 to 6/9 80 9 6/6 to 6/5 193 16 Total 939 366 P = 0.000. Table 10. Comparision of visual outcome according to PPC. PPC Visual Acuity No Yes Uncooperative 12 8 <1/60 259 95 1/60 to 3/60 108 91 6/60 to 6/36 73 43 6/24 to 6/18 193 125 6/12 to 6/9 63 26 6/6 to 6/5 151 58 Total 859 446 P = 0.000; PPC = Primary Posterior Capsulotomy. Table 11. Comparision of visual outcome according to in- sertion of IOL. IOL Visual Acuity No Yes Uncooperative 1 19 <1/60 31 323 1/60 to 3/60 17 182 6/60 to 6/36 3 113 6/24 to 6/18 48 270 6/12 to 6/9 2 87 6/6 to 6/5 3 206 Total 105 1200 P = 0.000. We examined age of intervention and found signifi- cantly better outcomes if the intervention was performed at >5 years (Table 12; P < 0.001). Vision was better at >5 years in both groups. We compared results by morphology of the cataract in non-traumatic group. Good results were achieved with lamellar cataracts (Table 13; P < 0.001). We examined cases with amblyopia and unilateral as well as bilateral cataracts. A significant difference was found in bilateral cases (Table 14; P < 0.001). In the non- traumatic group, 184 eyes had a unilateral cataract with deprivational amblyopia; vision improvement was not significant (Table 14; P = 0.510). For the traumatic group, we also gathered data regard- ing activities at the time of the injury and the object causing the injury (Tables 15 and 16). 4. Discussion The enrolled patient group consisted of 1305 eyes of 805 Copyright © 2012 SciRes. OJOph 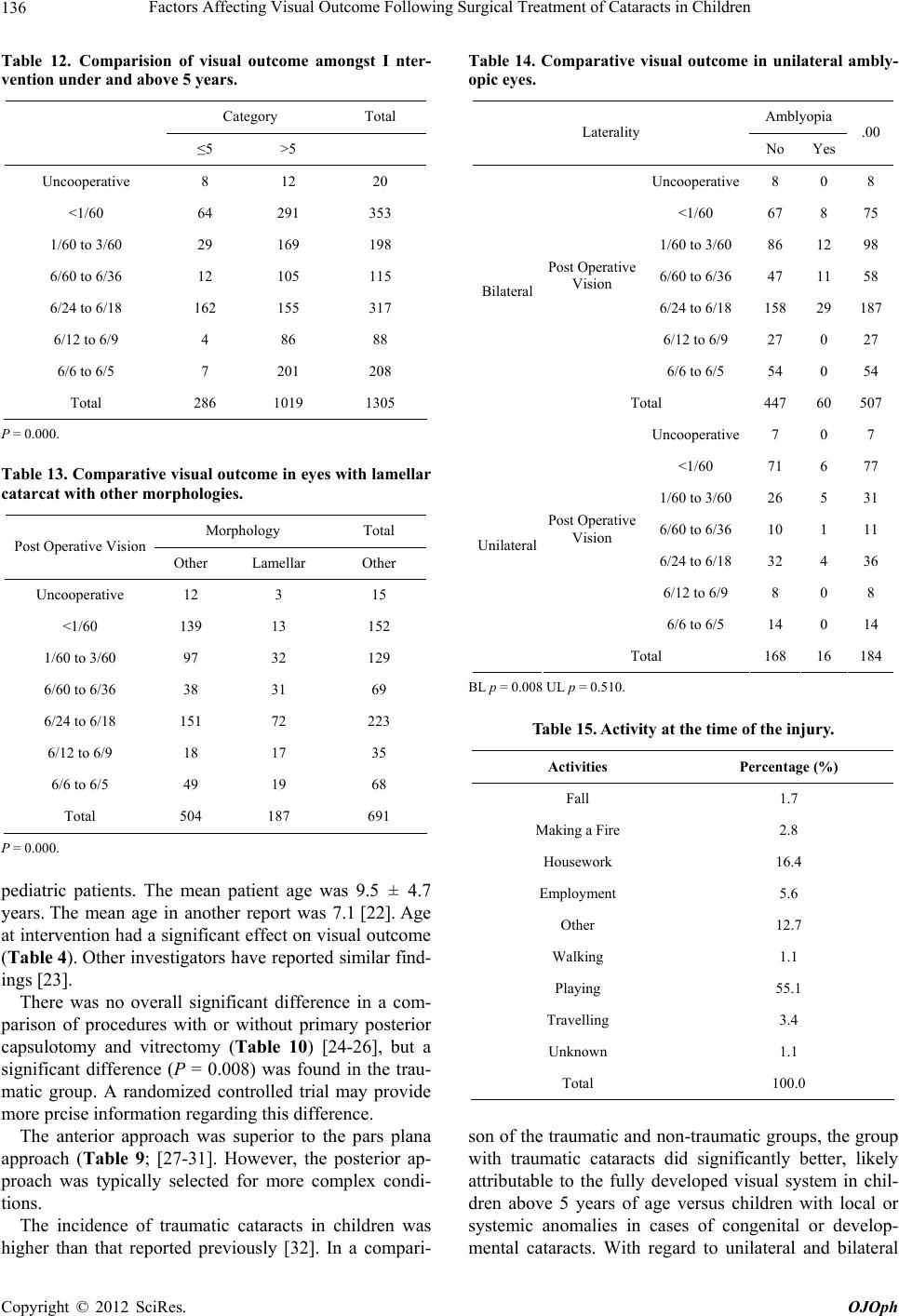 Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children 136 Table 12. Comparision of visual outcome amongst I nter- vention under and above 5 years. Category Total ≤5 >5 Uncooperative 8 12 20 <1/60 64 291 353 1/60 to 3/60 29 169 198 6/60 to 6/36 12 105 115 6/24 to 6/18 162 155 317 6/12 to 6/9 4 86 88 6/6 to 6/5 7 201 208 Total 286 1019 1305 P = 0.000. Table 13. Comparative visual outcome in eyes with lamellar catarcat with other morphologies. Morphology Total Post Operative Vision Other Lamellar Other Uncooperative 12 3 15 <1/60 139 13 152 1/60 to 3/60 97 32 129 6/60 to 6/36 38 31 69 6/24 to 6/18 151 72 223 6/12 to 6/9 18 17 35 6/6 to 6/5 49 19 68 Total 504 187 691 P = 0.000. pediatric patients. The mean patient age was 9.5 ± 4.7 years. The mean age in another report was 7.1 [22]. Age at intervention had a significant effect on visual outcome (Table 4). Other investigators have reported similar find- ings [23]. There was no overall significant difference in a com- parison of procedures with or without primary posterior capsulotomy and vitrectomy (Table 10) [24-26], but a significant difference (P = 0.008) was found in the trau- matic group. A randomized controlled trial may provide more prcise information regarding this difference. The anterior approach was superior to the pars plana approach (Table 9; [27-31]. However, the posterior ap- proach was typically selected for more complex condi- tions. The incidence of traumatic cataracts in children was higher than that reported previously [32]. In a compari- Table 14. Comparative visual outcome in unilateral ambly- opic eyes. Amblyopia Laterality No Yes .00 Uncooperative 8 0 8 <1/60 67 8 75 1/60 to 3/60 86 12 98 6/60 to 6/36 47 11 58 6/24 to 6/18 158 29 187 6/12 to 6/9 27 0 27 Post Operative Vision 6/6 to 6/5 54 0 54 Bilateral Total 447 60 507 Uncooperative 7 0 7 <1/60 71 6 77 1/60 to 3/60 26 5 31 6/60 to 6/36 10 1 11 6/24 to 6/18 32 4 36 6/12 to 6/9 8 0 8 Post Operative Vision 6/6 to 6/5 14 0 14 Unilateral Total 168 16 184 BL p = 0.008 UL p = 0.510. Table 15. Activity at the time of the injury. Activities Percentage (%) Fall 1.7 Making a Fire 2.8 Housework 16.4 Employment 5.6 Other 12.7 Walking 1.1 Playing 55.1 Travelling 3.4 Unknown 1.1 Total 100.0 son of the traumatic and non-traumatic groups, the group with traumatic cataracts did significantly better, likely attributable to the fully developed visual system in chil- dren above 5 years of age versus children with local or systemic anomalies in cases of congenital or develop- mental cataracts. With regard to unilateral and bilateral Copyright © 2012 SciRes. OJOph 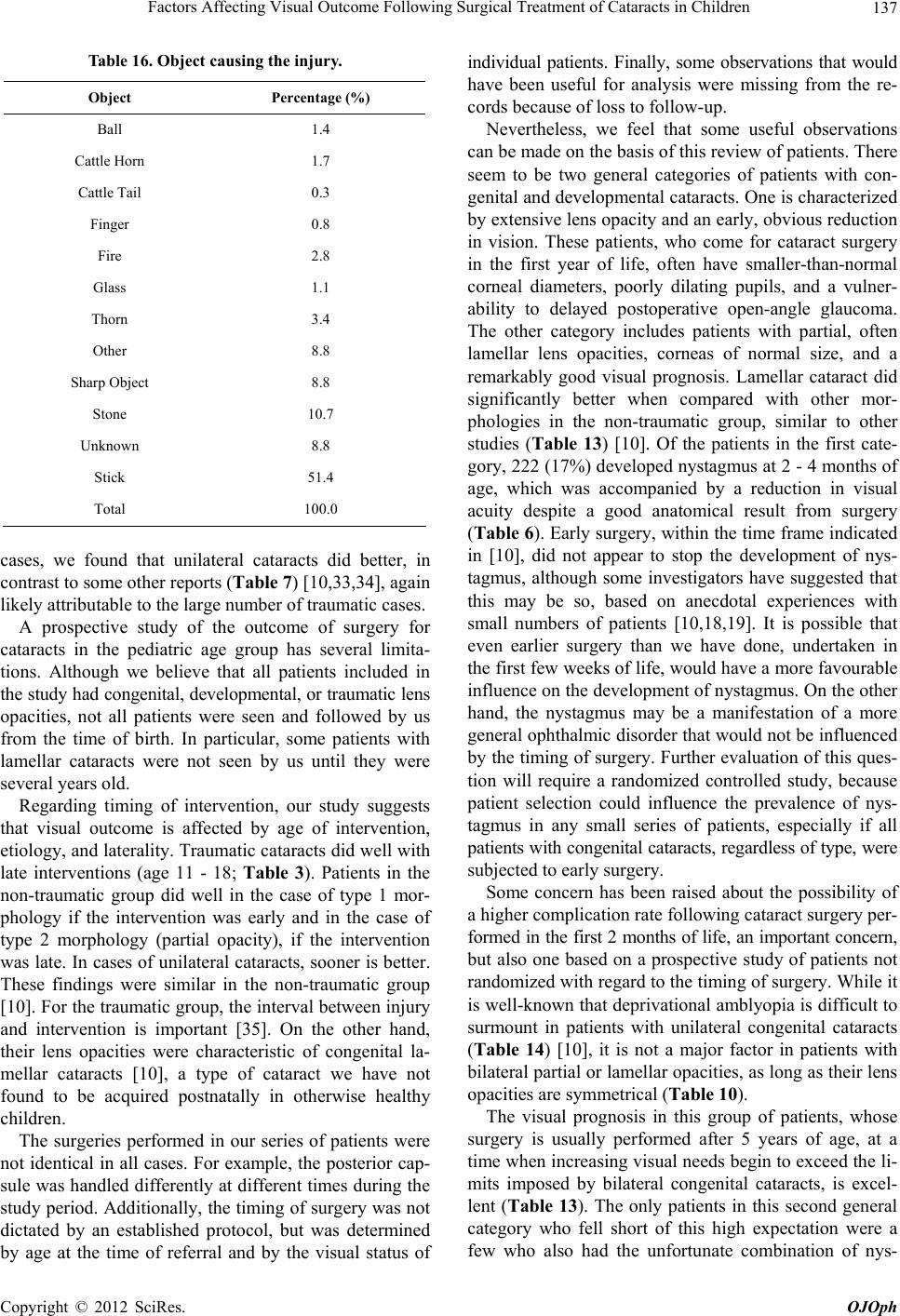 Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children 137 Table 16. Object causing the injury. Object Percentage (%) Ball 1.4 Cattle Horn 1.7 Cattle Tail 0.3 Finger 0.8 Fire 2.8 Glass 1.1 Thorn 3.4 Other 8.8 Sharp Object 8.8 Stone 10.7 Unknown 8.8 Stick 51.4 Total 100.0 cases, we found that unilateral cataracts did better, in contrast to some other reports (Table 7) [10,33,34], again likely attributable to the large number of traumatic cases. A prospective study of the outcome of surgery for cataracts in the pediatric age group has several limita- tions. Although we believe that all patients included in the study had congenital, developmental, or traumatic lens opacities, not all patients were seen and followed by us from the time of birth. In particular, some patients with lamellar cataracts were not seen by us until they were several years old. Regarding timing of intervention, our study suggests that visual outcome is affected by age of intervention, etiology, and laterality. Traumatic cataracts did well with late interventions (age 11 - 18; Table 3). Patients in the non-traumatic group did well in the case of type 1 mor- phology if the intervention was early and in the case of type 2 morphology (partial opacity), if the intervention was late. In cases of unilateral cataracts, sooner is better. These findings were similar in the non-traumatic group [10]. For the traumatic group, the interval between injury and intervention is important [35]. On the other hand, their lens opacities were characteristic of congenital la- mellar cataracts [10], a type of cataract we have not found to be acquired postnatally in otherwise healthy children. The surgeries performed in our series of patients were not identical in all cases. For example, the posterior cap- sule was handled differently at different times during the study period. Additionally, the timing of surgery was not dictated by an established protocol, but was determined by age at the time of referral and by the visual status of individual patients. Finally, some observations that would have been useful for analysis were missing from the re- cords because of loss to follow-up. Nevertheless, we feel that some useful observations can be made on the basis of this review of patients. There seem to be two general categories of patients with con- genital and developmental cataracts. One is characterized by extensive lens opacity and an early, obvious reduction in vision. These patients, who come for cataract surgery in the first year of life, often have smaller-than-normal corneal diameters, poorly dilating pupils, and a vulner- ability to delayed postoperative open-angle glaucoma. The other category includes patients with partial, often lamellar lens opacities, corneas of normal size, and a remarkably good visual prognosis. Lamellar cataract did significantly better when compared with other mor- phologies in the non-traumatic group, similar to other studies (Table 13) [10]. Of the patients in the first cate- gory, 222 (17%) developed nystagmus at 2 - 4 months of age, which was accompanied by a reduction in visual acuity despite a good anatomical result from surgery (Table 6). Early surgery, within the time frame indicated in [10], did not appear to stop the development of nys- tagmus, although some investigators have suggested that this may be so, based on anecdotal experiences with small numbers of patients [10,18,19]. It is possible that even earlier surgery than we have done, undertaken in the first few weeks of life, would have a more favourable influence on the development of nystagmus. On the other hand, the nystagmus may be a manifestation of a more general ophthalmic disorder that would not be influenced by the timing of surgery. Further evaluation of this ques- tion will require a randomized controlled study, because patient selection could influence the prevalence of nys- tagmus in any small series of patients, especially if all patients with congenital cataracts, regardless of type, were subjected to early surgery. Some concern has been raised about the possibility of a higher complication rate following cataract surgery per- formed in the first 2 months of life, an important concern, but also one based on a prospective study of patients not randomized with regard to the timing of surgery. While it is well-known that deprivational amblyopia is difficult to surmount in patients with unilateral congenital cataracts (Table 14) [10], it is not a major factor in patients with bilateral partial or lamellar opacities, as long as their lens opacities are symmetrical (Table 10). The visual prognosis in this group of patients, whose surgery is usually performed after 5 years of age, at a time when increasing visual needs begin to exceed the li- mits imposed by bilateral congenital cataracts, is excel- lent (Table 13). The only patients in this second general category who fell short of this high expectation were a few who also had the unfortunate combination of nys- Copyright © 2012 SciRes. OJOph 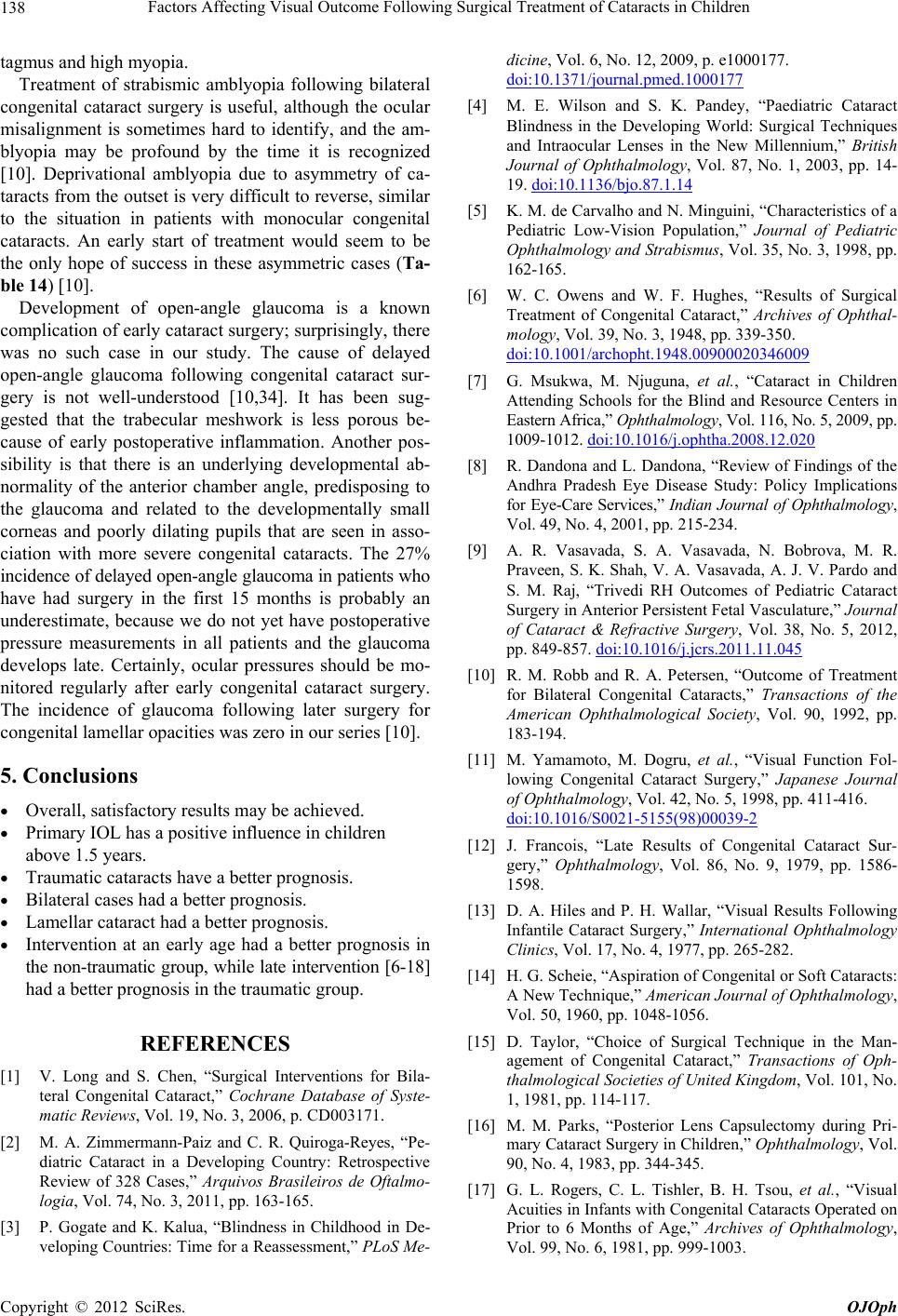 Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children 138 tagmus and high myopia. Treatment of strabismic amblyopia following bilateral congenital cataract surgery is useful, although the ocular misalignment is sometimes hard to identify, and the am- blyopia may be profound by the time it is recognized [10]. Deprivational amblyopia due to asymmetry of ca- taracts from the outset is very difficult to reverse, similar to the situation in patients with monocular congenital cataracts. An early start of treatment would seem to be the only hope of success in these asymmetric cases (Ta- ble 14) [10]. Development of open-angle glaucoma is a known complication of early cataract surgery; surprisingly, there was no such case in our study. The cause of delayed open-angle glaucoma following congenital cataract sur- gery is not well-understood [10,34]. It has been sug- gested that the trabecular meshwork is less porous be- cause of early postoperative inflammation. Another pos- sibility is that there is an underlying developmental ab- normality of the anterior chamber angle, predisposing to the glaucoma and related to the developmentally small corneas and poorly dilating pupils that are seen in asso- ciation with more severe congenital cataracts. The 27% incidence of delayed open-angle glaucoma in patients who have had surgery in the first 15 months is probably an underestimate, because we do not yet have postoperative pressure measurements in all patients and the glaucoma develops late. Certainly, ocular pressures should be mo- nitored regularly after early congenital cataract surgery. The incidence of glaucoma following later surgery for congenital lamellar opacities was zero in our series [10]. 5. Conclusions Overall, satisfactory results may be achieved. Primary IOL has a positive influence in children above 1.5 years. Traumatic cataracts have a better prognosis. Bilateral cases had a better prognosis. Lamellar cataract had a better prognosis. Intervention at an early age had a better prognosis in the non-traumatic group, while late intervention [6-18] had a better prognosis in the traumatic group. REFERENCES [1] V. Long and S. Chen, “Surgical Interventions for Bila- teral Congenital Cataract,” Cochrane Database of Syste- matic Reviews, Vol. 19, No. 3, 2006, p. CD003171. [2] M. A. Zimmermann-Paiz and C. R. Quiroga-Reyes, “Pe- diatric Cataract in a Developing Country: Retrospective Review of 328 Cases,” Arquivos Brasileiros de Oftalmo- logia, Vol. 74, No. 3, 2011, pp. 163-165. [3] P. Gogate and K. Kalua, “Blindness in Childhood in De- veloping Countries: Time for a Reassessment,” PLoS Me- dicine, Vol. 6, No. 12, 2009, p. e1000177. doi:10.1371/journal.pmed.1000177 [4] M. E. Wilson and S. K. Pandey, “Paediatric Cataract Blindness in the Developing World: Surgical Techniques and Intraocular Lenses in the New Millennium,” British Journal of Ophthalmology, Vol. 87, No. 1, 2003, pp. 14- 19. doi:10.1136/bjo.87.1.14 [5] K. M. de Carvalho and N. Minguini, “Characteristics of a Pediatric Low-Vision Population,” Journal of Pediatric Ophthalmology and Strabismus, Vol. 35, No. 3, 1998, pp. 162-165. [6] W. C. Owens and W. F. Hughes, “Results of Surgical Treatment of Congenital Cataract,” Archives of Ophthal- mology, Vol. 39, No. 3, 1948, pp. 339-350. doi:10.1001/archopht.1948.00900020346009 [7] G. Msukwa, M. Njuguna, et al., “Cataract in Children Attending Schools for the Blind and Resource Centers in Eastern Africa,” Ophthalmology, Vol. 116, No. 5, 2009, pp. 1009-1012. doi:10.1016/j.ophtha.2008.12.020 [8] R. Dandona and L. Dandona, “Review of Findings of the Andhra Pradesh Eye Disease Study: Policy Implications for Eye-Care Services,” Indian Journal of Ophthalmology, Vol. 49, No. 4, 2001, pp. 215-234. [9] A. R. Vasavada, S. A. Vasavada, N. Bobrova, M. R. Praveen, S. K. Shah, V. A. Vasavada, A. J. V. Pardo and S. M. Raj, “Trivedi RH Outcomes of Pediatric Cataract Surgery in Anterior Persistent Fetal Vasculature,” Journal of Cataract & Refractive Surgery, Vol. 38, No. 5, 2012, pp. 849-857. doi:10.1016/j.jcrs.2011.11.045 [10] R. M. Robb and R. A. Petersen, “Outcome of Treatment for Bilateral Congenital Cataracts,” Transactions of the American Ophthalmological Society, Vol. 90, 1992, pp. 183-194. [11] M. Yamamoto, M. Dogru, et al., “Visual Function Fol- lowing Congenital Cataract Surgery,” Japanese Journal of Ophthalmology, Vol. 42, No. 5, 1998, pp. 411-416. doi:10.1016/S0021-5155(98)00039-2 [12] J. Francois, “Late Results of Congenital Cataract Sur- gery,” Ophthalmology, Vol. 86, No. 9, 1979, pp. 1586- 1598. [13] D. A. Hiles and P. H. Wallar, “Visual Results Following Infantile Cataract Surgery,” International Ophthalmology Clinics, Vol. 17, No. 4, 1977, pp. 265-282. [14] H. G. Scheie, “Aspiration of Congenital or Soft Cataracts: A New Technique,” American Journal of Ophthalmology, Vol. 50, 1960, pp. 1048-1056. [15] D. Taylor, “Choice of Surgical Technique in the Man- agement of Congenital Cataract,” Transactions of Oph- thalmological Societies of United Kingdom, Vol. 101, No. 1, 1981, pp. 114-117. [16] M. M. Parks, “Posterior Lens Capsulectomy during Pri- mary Cataract Surgery in Children,” Ophthalmology, Vol. 90, No. 4, 1983, pp. 344-345. [17] G. L. Rogers, C. L. Tishler, B. H. Tsou, et al., “Visual Acuities in Infants with Congenital Cataracts Operated on Prior to 6 Months of Age,” Archives of Ophthalmology, Vol. 99, No. 6, 1981, pp. 999-1003. Copyright © 2012 SciRes. OJOph 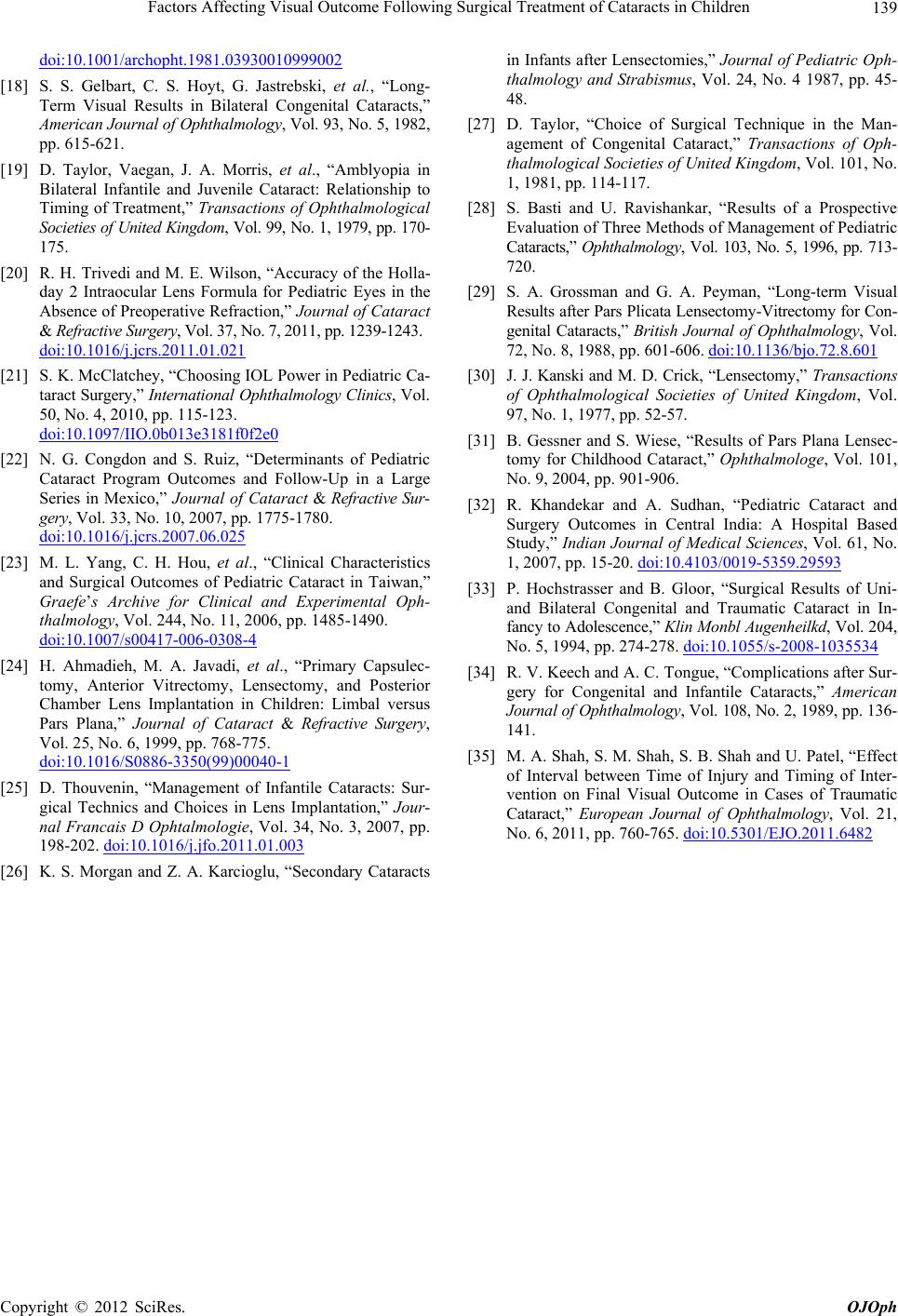 Factors Affecting Visual Outcome Following Surgical Treatment of Cataracts in Children Copyright © 2012 SciRes. OJOph 139 doi:10.1001/archopht.1981.03930010999002 [18] S. S. Gelbart, C. S. Hoyt, G. Jastrebski, et al., “Long- Term Visual Results in Bilateral Congenital Cataracts,” American Journal of Ophthalmology, Vol. 93, No. 5, 1982, pp. 615-621. [19] D. Taylor, Vaegan, J. A. Morris, et al., “Amblyopia in Bilateral Infantile and Juvenile Cataract: Relationship to Timing of Treatment,” Transactions of Ophthalmological Societies of United Kingdom, Vol. 99, No. 1, 1979, pp. 170- 175. [20] R. H. Trivedi and M. E. Wilson, “Accuracy of the Holla- day 2 Intraocular Lens Formula for Pediatric Eyes in the Absence of Preoperative Refraction,” Journal of Cataract & Refractive Surgery, Vol. 37, No. 7, 2011, pp. 1239-1243. doi:10.1016/j.jcrs.2011.01.021 [21] S. K. McClatchey, “Choosing IOL Power in Pediatric Ca- taract Surgery,” International Ophthalmology Clinics, Vol. 50, No. 4, 2010, pp. 115-123. doi:10.1097/IIO.0b013e3181f0f2e0 [22] N. G. Congdon and S. Ruiz, “Determinants of Pediatric Cataract Program Outcomes and Follow-Up in a Large Series in Mexico,” Journal of Cataract & Refractive Sur- gery, Vol. 33, No. 10, 2007, pp. 1775-1780. doi:10.1016/j.jcrs.2007.06.025 [23] M. L. Yang, C. H. Hou, et al., “Clinical Characteristics and Surgical Outcomes of Pediatric Cataract in Taiwan,” Graefe’s Archive for Clinical and Experimental Oph- thalmology, Vol. 244, No. 11, 2006, pp. 1485-1490. doi:10.1007/s00417-006-0308-4 [24] H. Ahmadieh, M. A. Javadi, et al., “Primary Capsulec- tomy, Anterior Vitrectomy, Lensectomy, and Posterior Chamber Lens Implantation in Children: Limbal versus Pars Plana,” Journal of Cataract & Refractive Surgery, Vol. 25, No. 6, 1999, pp. 768-775. doi:10.1016/S0886-3350(99)00040-1 [25] D. Thouvenin, “Management of Infantile Cataracts: Sur- gical Technics and Choices in Lens Implantation,” Jour- nal Francais D Ophtalmologie, Vol. 34, No. 3, 2007, pp. 198-202. doi:10.1016/j.jfo.2011.01.003 [26] K. S. Morgan and Z. A. Karcioglu, “Secondary Cataracts in Infants after Lensectomies,” Journal of Pediatric Oph- thalmology and Strabismus, Vol. 24, No. 4 1987, pp. 45- 48. [27] D. Taylor, “Choice of Surgical Technique in the Man- agement of Congenital Cataract,” Transactions of Oph- thalmological Societies of United Kingdom, Vol. 101, No. 1, 1981, pp. 114-117. [28] S. Basti and U. Ravishankar, “Results of a Prospective Evaluation of Three Methods of Management of Pediatric Cataracts,” Ophtha lmolo gy, Vol. 103, No. 5, 1996, pp. 713- 720. [29] S. A. Grossman and G. A. Peyman, “Long-term Visual Results after Pars Plicata Lensectomy-Vitrectomy for Con- genital Cataracts,” British Journal of Ophthalmology, Vol. 72, No. 8, 1988, pp. 601-606. doi:10.1136/bjo.72.8.601 [30] J. J. Kanski and M. D. Crick, “Lensectomy,” Transactions of Ophthalmological Societies of United Kingdom, Vol. 97, No. 1, 1977, pp. 52-57. [31] B. Gessner and S. Wiese, “Results of Pars Plana Lensec- tomy for Childhood Cataract,” Ophthalmologe, Vol. 101, No. 9, 2004, pp. 901-906. [32] R. Khandekar and A. Sudhan, “Pediatric Cataract and Surgery Outcomes in Central India: A Hospital Based Study,” Indian Journal of Medical Sciences, Vol. 61, No. 1, 2007, pp. 15-20. doi:10.4103/0019-5359.29593 [33] P. Hochstrasser and B. Gloor, “Surgical Results of Uni- and Bilateral Congenital and Traumatic Cataract in In- fancy to Adolescence,” Klin Monbl Augenheilkd, Vol. 204, No. 5, 1994, pp. 274-278. doi:10.1055/s-2008-1035534 [34] R. V. Keech and A. C. Tongue, “Complications after Sur- gery for Congenital and Infantile Cataracts,” American Journal of Ophthalmology, Vol. 108, No. 2, 1989, pp. 136- 141. [35] M. A. Shah, S. M. Shah, S. B. Shah and U. Patel, “Effect of Interval between Time of Injury and Timing of Inter- vention on Final Visual Outcome in Cases of Traumatic Cataract,” European Journal of Ophthalmology, Vol. 21, No. 6, 2011, pp. 760-765. doi:10.5301/EJO.2011.6482
|