H. SUGIURA, S. DEMURA
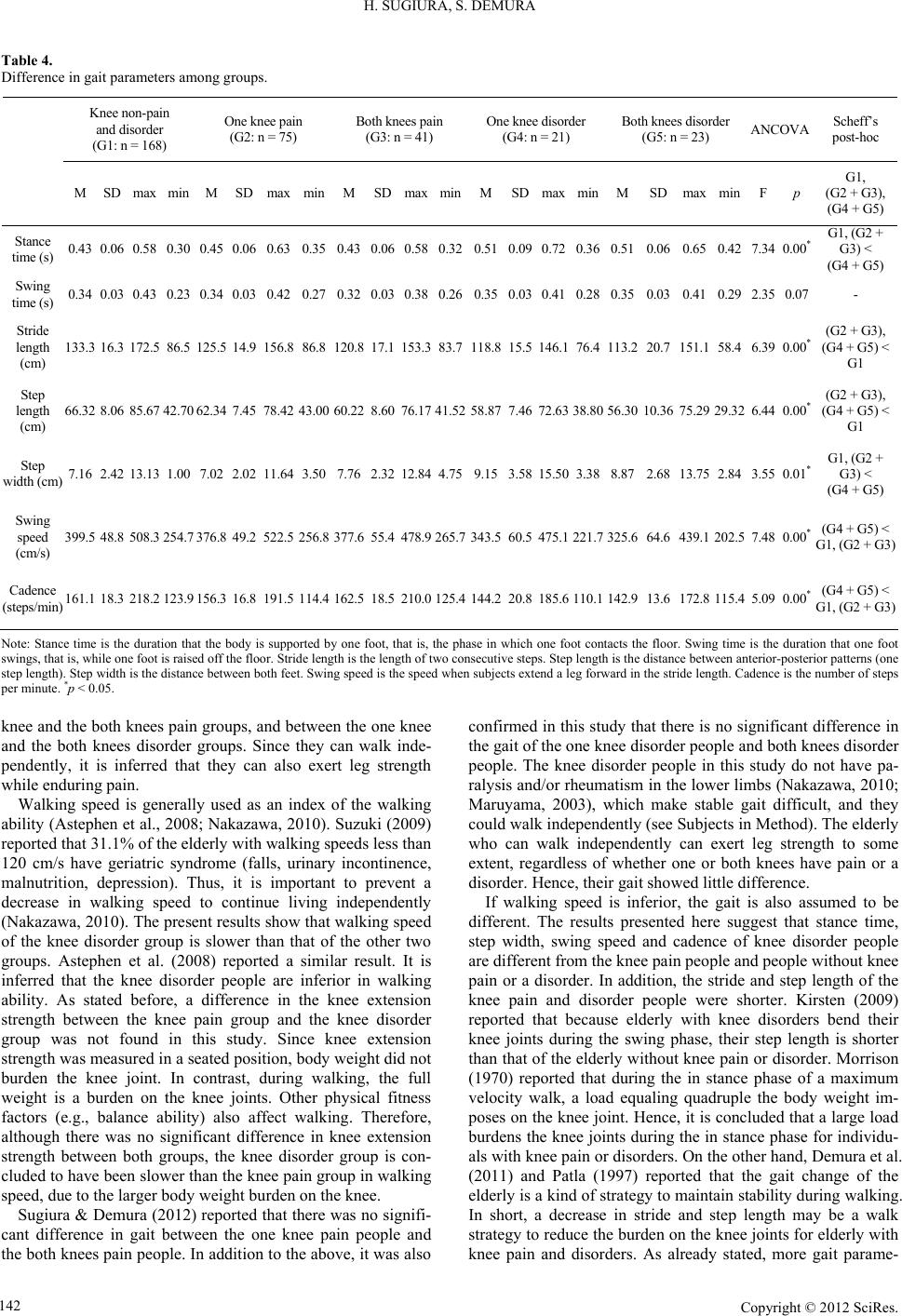
ters (stance time, step width, swing speed and cadence) showed
significant differences between the knee disorder group and the
knee pain group. It is inferred that the knee disorder individuals
establish a strategy to maintain walking stability, rather than
trying to walk quickly.
It is necessary to further examine ability to achieve activities
of daily living other than walking in the female elderly with
knee pain and disorder.
Conclusion
In conclusion, the female elderly with knee pain and/or dis-
orders are inferior in knee extension strength and walk ability to
the elderly without knee pain or disorder. In addition, the fe-
male elderly with knee disorders are inferior in walking ability
to the elderly with knee pain.
REFERENCES
Alindon, T. E., Snow, S., Cooper, C., & Dieppe, P. A. (1992). Patterns
of osteoarthritis of the knee joint in the community: The importance
of the patellofemoral joint. Annals of the Rheumatic Diseases, 51,
844-849. doi:10.1136/ard.51.7.844
Al-Zaharni, K. S., & Bakheit, A. M. (2002). A study of the gait charac-
teristics of patients with chronic osteoarthritis of the knee. Disability
and Rehabilitation , 24, 275-280. doi:10.1080/09638280110087098
Andriacchi, T., Galante, J., & Fermier, R. (1982). The influence of total
knee replacement design on walking and stair-climbing. Journal of
Bone and Joint Surgery -Mericana Volume, 64, 1328-1335.
Astephen, J. L., Deluzio, K. J., Caldwell, G. E., & Dunbar, M. J. (2008).
Biomechanical changes at the hip, knee, and ankle joints during gait
are associated with knee osteoarthritis severity. Journal of Ortho-
paedic Research, 26, 332-341. doi:10.1002/jor.20496
Bellamy, N., Buchanan, W. W., Goldsmith, C. H., Campbell, J., & Stitt,
L. W. (1988). Validation study of WOMAC: A health status instru-
ment for measuring clinically important patient relevant outcomes to
antirheumatic drug therapy in patients with osteoarthritis of the hip
or knee. Journal of Rheu ma t o lo g y , 15, 1833-1840.
Berman, A. T., Zarro, V. J., Bosacco, S. J., & Israelite, C. (1987).
Quantitative gait analysis after unilateral or bilateral knee replace-
ment. Journal of Bone and Joint Surgery-Mericana Volume, 69,
1340-1345.
Demura, S., Yamaji, S., & Sato, S. (2011). Gait and fall characteristics
of the elderly. Journal of Joint Surgery, 30, 100-107.
Frontera, W. R., Hughes, V. A., Lutz, K. J., & Evans, W. J. (1991). A
cross-sectional study of muscle strength and mass in 45- to
78-year-old men and women. Journal of Applied Physiology, 71,
644-650.
Hashimoto, H., Hanyu, T., Clement, S., & Elizabeth, L. (2003). The
development of Japanese edition knee function scale—A comparison
with WOMAC (Western Ontario and McMaster Universities) os-
teoarthritis index. Journal of Orthopaedic Science, 77, 22-23.
Hurley, M. V., Rees, J., & Newham, D. J. (1998). Quadriceps function,
proprioceptive acuity and functional performance in healthy young,
middle-aged and eld erly subjects. Age and Ageing, 27, 55-62.
doi:10.1093/ageing/27.1.55
Jochanan, S., Robert, H. R., Aaron, C., Eliana, E. M., & Jeremy, M. J.
(2009). Physical acti vity, function, and longevity among the very old.
Archives of Internal Medicine, 169, 1476-1483.
doi:10.1001/archinternmed.2009.248
Kirsten, G. N. (2009). Gait analysis by observation. Tokyo: Igaku-
Shoin.
Kurokawa, Y., Takahashi, M., & Turumi T. (2001). Physiotherapy of
leg joint disorders. Tokyo: Mitsuwa Shoten.
Maruyama, H. (2003). The gait. Tokyo: The Society of Physical The-
rapy Science.
Mary, E., & Tinetti, M. D. (2003). Preventing falls in elderly persons.
New England Journal of Medci ne , 348, 42-49.
doi:10.1056/NEJMcp020719
Morrison, J. B. (1970). The mechanics of the knee joint in relation to
normal walking. Journal of Biomechan i c al Engineering, 3, 51-61.
doi:10.1016/0021-9290(70)90050-3
Nakazawa, K. (2010). Neurorehabilitation of walking. Tokyo: Kyo-
rin-Shoin.
Oida, Y., & Nakamura, N. (2008). Exercise learning support manual for
the knee joint ache prevention and reduction. Tokyo: Sunlife Plan.
Oliveria, S. A., Fels o n , D. T., Ciril lo , P. A., Re ed , J. I. , & Walker, A. M.
(1999). Body weight, body mass index, and incident symptomatic
osteoarthritis of the hand, hip and knee. Epidemiology, 10, 161-166.
doi:10.1097/00001648-199903000-00013
Patla, A. E. (1997). Understanding the roles of vision in the control of
human locomotion. Gait Posture, 5, 54-69.
doi:10.1016/S0966-6362(96)01109-5
Peat, G., McCarney, R., & Croft, P. (2001). Knee pain and osteoarthri-
tis in older adults: A review of community burden and current use of
primary health care. Annals of the Rheumatic Diseases, 60, 91-97.
doi:10.1136/ard.60.2.91
Pratt, D. J. (1994). Some aspects of modern orthotics. Physiological
Measurement, 15, 1-27. doi:10.1088/0967-3334/15/1/001
Sato, D., Kaneda, K., Wakabayashi, H., & Nomura, T. (2007). The
water exercise improves health-related quality of life of frail elderly
people at day service facility. Quality of Life Research, 16, 1577-
1585. doi:10.1007/s11136-007-9269-2
Sugiura, H., & Demura, S. (2012). Effect of subjective knee joint pain
on knee extension strength, gait and ADL score in the female elderly.
Gazzetta Medica Italiana, 171, 533-540.
Suzuki, M., Ohyama, N., Yamada, K., & Kanamori, M. (2002) The
relationship between fear of falling, activities of daily living and
quality of life among elderly individuals. Nursing and Health Sci-
ences, 4, 155-161. doi:10.1046/j.1442-2018.2002.00123.x
Suzuki, T. (2009). The physical characteristic of the elderly. Health
Care, 51, 148-153.
Tennant, A., Fear, J., Pickering, A., Hillman, M., Cutts, A., & Cham-
berlain, M. A. (1995). Prevalence of knee problems in the population
aged 55 years and over: Identifying the need for arthroplasty. British
Medical Journal, 310, 1291-1293. doi:10.1136/bmj.310.6990.1291
Urwin, M., Symmons, D., Allison, T., Brammah, T., Busby, H., &
Roxby, M. (1998). Estimating the burden of musculoskeletal disor-
ders in the community: The comparative prevalence of symptoms at
different anatomical sites, and the relation to social deprivation. An-
nals of Rheumatology, 5 7 , 649-655. doi:10.1136/ard.57.11.649
Yoshimura, N., Nishioka, S., Kinoshita, H., Hori, N., Nishioka, T.,
Ryujin, M., Mantani, Y., Miyake, M., David, C., & Cyrus, C. (2004).
Risk factors for knee osteoarthritis in Japanese women: Heavy
weight, previous joint injuries, and occupational activities. Journal of
Rheumatology, 31, 157-162.
Zeni Jr., J. A., & Higginson, J. S. (2009). Differences in gait parameters
between healthy subjects and persons with moderate and severe knee
osteoarthritis: A result of altered walking speed? Clinical Biome-
chanics, 24, 372-3 78. doi:10.1016/j.clinbiomech.2009.02.001
Zoltan, B., Robert, P., Arpad, I., & Rita, M. K. (2006). The influence of
walking speed on gait parameters in healthy people and in patients
with osteoarthritis. Knee Surgery, Sports Traumatology, Arthroscopy,
14, 612-662. doi:10.1007/s00167-005-0005-6
Copyright © 2012 SciRe s . 143