M. W. Kuria, Y. Olando / Open Journal of Psychiatry 2 (2012) 301-304
302
of reasons. Firstly, the manufacture of the traditional
brews is usually unhygienic and at times the brews have
been laced with methanol resulting to deaths blindness
and disabilities [8]. Secondly, most of the brews are
manufactured illegally without control on the ethanol
content. Thirdly, the cost of the brews is relatively lower
than that of the legal brews and therefore the majority of
the alcohol users can afford it. Kenya has currently
passed a law to legalize traditional and illicit brews so as
to regulate production, sale and consumption of alcoholic
drinks [1].
Kenyans have a hazardous drinking pattern of alcohol
which can cause social and medical harm [7,9] with an
increasingly use by underage and young persons [10].
These coupled with a repo rted increase in lifetime drink-
ing among young, black African; and use of drugs by
females as a way to cope with current or past life stress-
ors [11,12] demands that quality control of alcoholic
brews be instituted and enforced.
Anecdotal reports indicate that consuming killer sub-
stances bottled in filthy backyards and cleverly labeled
as fortified wine, gin, opaque beer, vodka, brandy or rum
are currently sold in the Kenyan market. According to
anecdotal reports the suspect drinks, said to control 80
per cent of the wines and spirits market, contravene all
the mandatory requirements for manufacture as well as
trade in alcoholic beverag es—tax obligation, quality cer-
tification, wholesomeness and packaging. Cheap alcohol
package in small quantities (250 milliliter) which have in
the past being available in the Kenyan market has cur-
rently being prohibited by the new Alcoholic Drinks
Control Act, 2010.
In Kenya, alcohol consumption is highest in poor
communities where potent home brewed alcoho l is cheap
and readily available. Quality control is weak; meaning
ethanol content can at times be dangerously high. Ex am-
ples of such home made brews include, “muratina”,
“mnazi”, “changaa”, “mbangari”, “busaa”, and “kumi-
kumi”. These are the illicit brews that the newly passed
law (Alcohol Drinks Control Act) intends to make licit
and industrialize the production in attempt to protect the
alcohol users from harmful effects of contaminated il-
licit brews (Kenya Gazette supplement, 2010). Since
cost and availability of alcohol are factors that influ-
ence alcohol use an increase in available licit types of
alcohol in market may result to more people drinking
alcohol.
Illicit drug use has spread from urban and advantaged
groups to rural and disadvantaged (poor) communities
where youth associate alcohol use with enjoyment, fun
and survival [13]. This is true for Kenya where use of
illicit alcohol has become common among rural and in-
formal settlement communities where dealing with the
alcohol dependence problem is further complicated by
the scarce resources in such communities.
In spite of the high health and social economic costs
associated with alcohol use disorders most African go-
vernments depend heavily on alcohol industries for reve-
nue received through taxation. These coupled with em-
ployment opportunities for people gives the alcohol in-
dustries a bargaining power when it comes to introduce-
tion, implementation and enforcement of alcohol po licies
in Africa.
2. METHOD
Ethical approval for the study was obtained from the
Kenyatta National Hospital/University of Nairobi ethi-
cal review board. Permission to collect the illicit alco-
hol brew samples was obtained from the Ministry of
Public Health and all ethical considerations were ad-
hered to. One hundred and eighty eight participants of a
community based detoxification and rehabilitation pro-
gramme were asked to indicate the types of alcohol
beverages they were using in order of prevalence irre-
spective of whether the brews were licit or illicit. Four-
teen most commonly used brews were randomly pur-
chased fro m the twelv e vi llage s lo cat ed wi thin the s tud y
area.
The purchased alcohol beverages were given a serial
number and taken to the Government Chemist for che-
mical, analysis principal investigator and a public health
officer.
The chemical composition of the alcohol samples was
determined through gas chromatography.
3. RESULTS
A total of 188 participants underwent community-based
detoxification but only 156 were followed up for the six
months. Majority (91.5%) was male and 8.5% were fe-
male. Majority (60.5%) of the participants had begun
drinking alcohol before the age of 18 years, with the
mean AUDIT score being 28.6 for males and 26.6 for
females. The mean age of the group was 31.9 years, with
majority (84%) of the participants aged below 40 years.
The majority (53.3%) of the participants earned an in-
come of less than 143 United States dollars per month.
The majority (51.1%) were married, while 38.9% were
single. The remaining participants were either separated
or divorced.
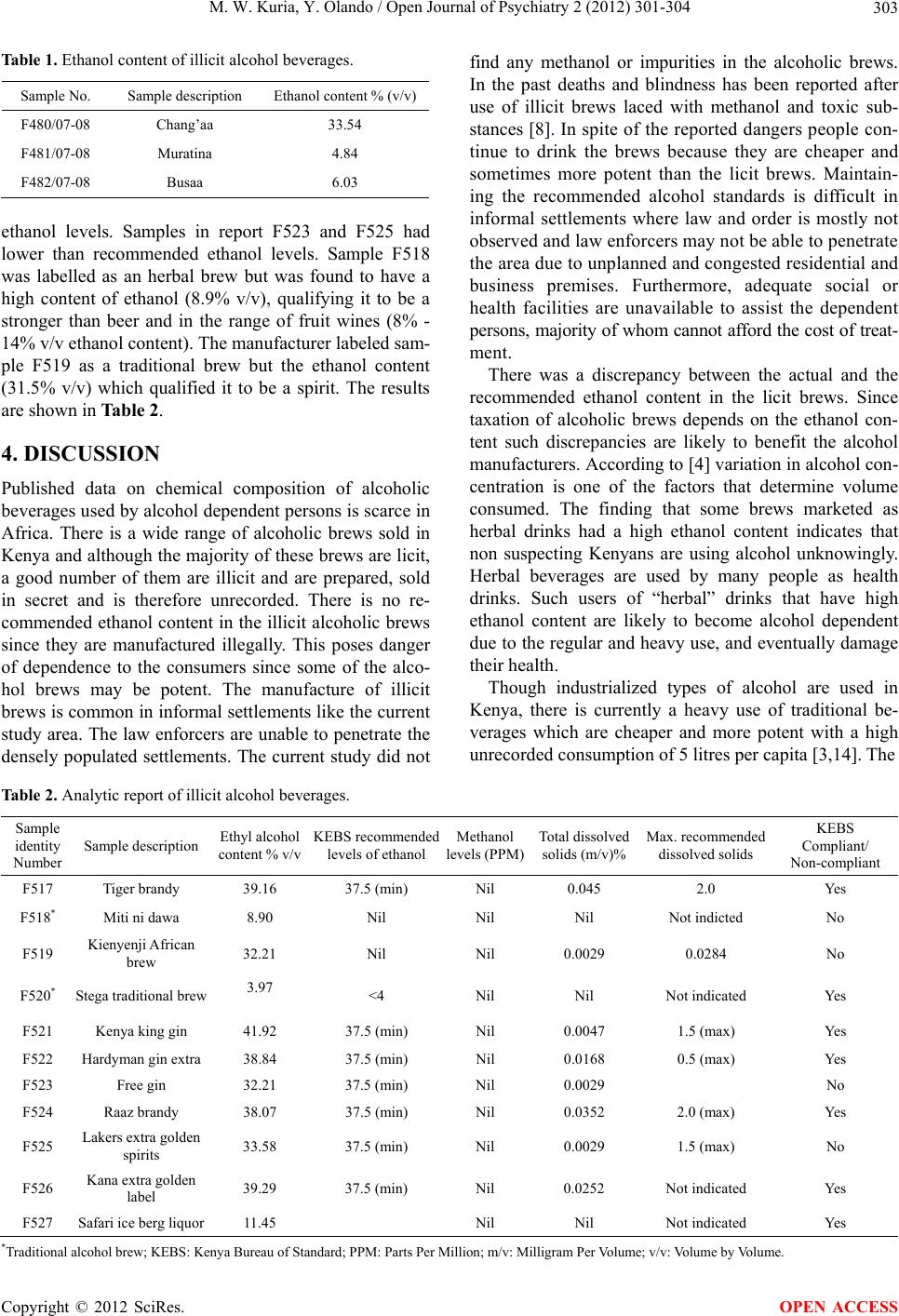
Fourteen samples of alcoholic b everage were collected
from the study area and labeled F517 - F527 for the licit
brews and F480 - F482 for the illicit brews. Two of the
illicit brews were within the beer range of alcoholic
brews while the third one was within the spirit range.
The results are shown in Table 1.
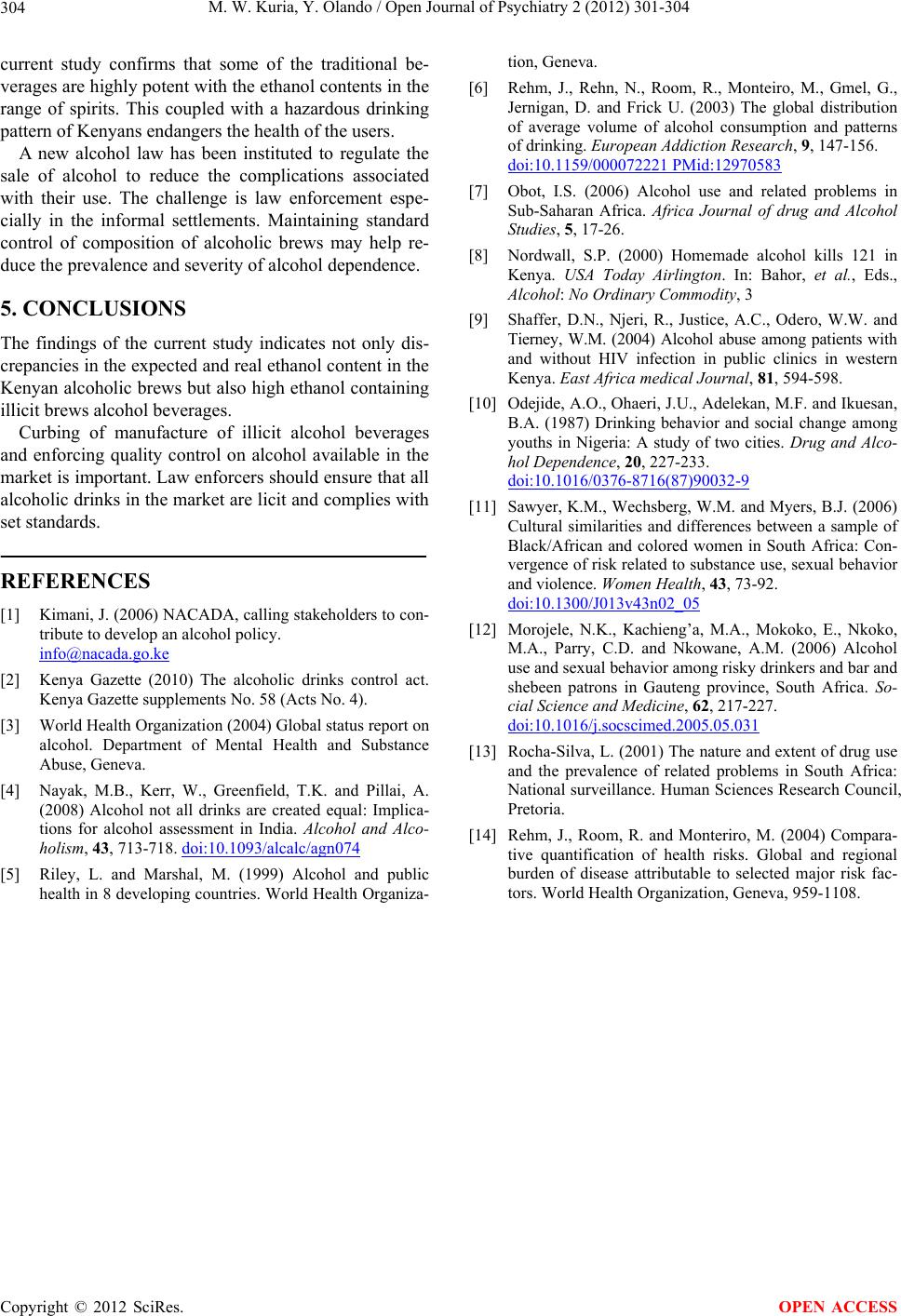
Four out of the eleven licit brews had not complied
with the recommended Kenya Bureau of Standards
Copyright © 2012 SciRes. OPEN ACCESS