S. Shimodera et al. / Open Journal of Psychiatry 2 (2012) 258-261
260
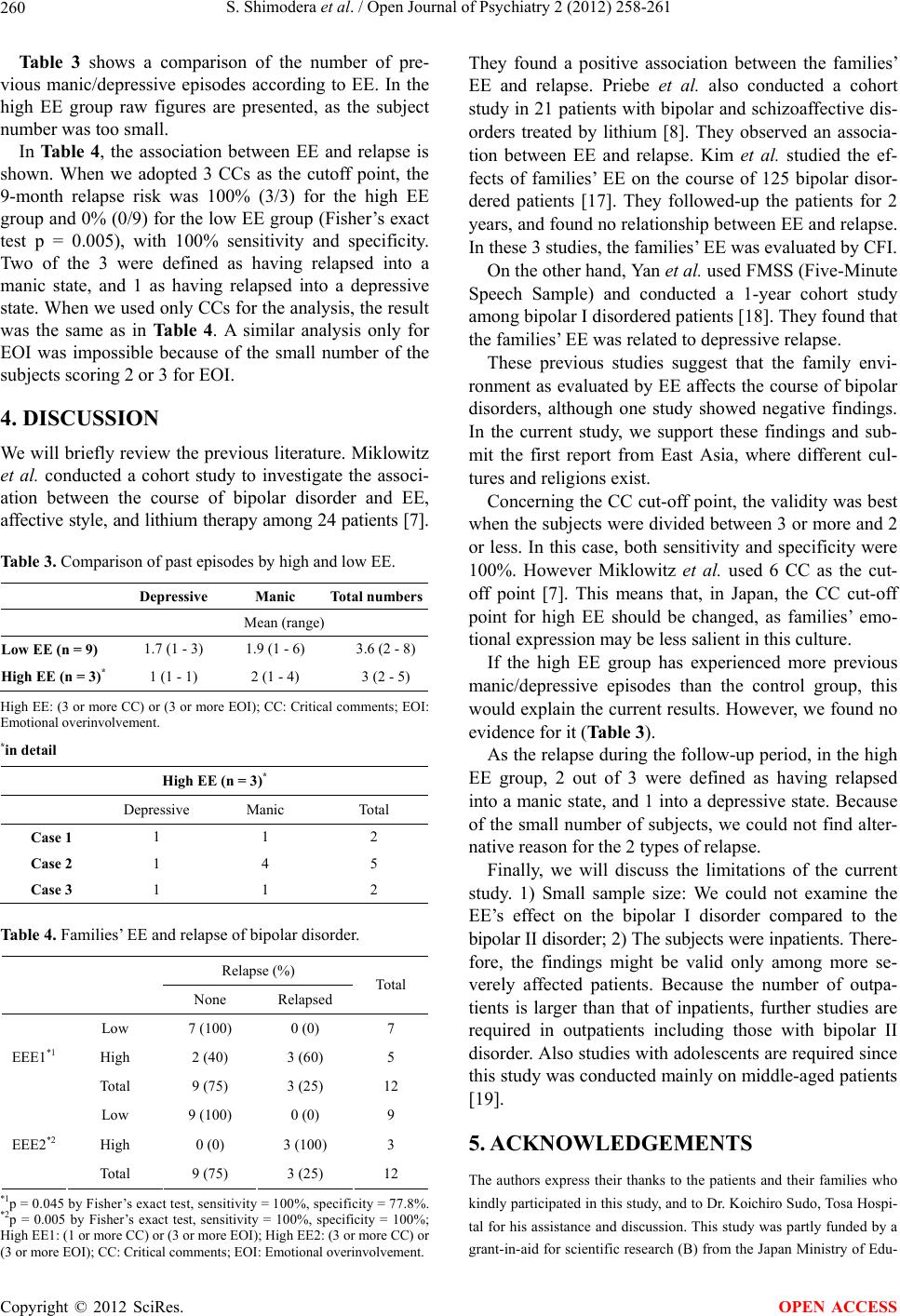
Table 3 shows a comparison of the number of pre-
vious manic/depressive episodes according to EE. In the
high EE group raw figures are presented, as the subject
number was too small.
In Ta b le 4, the association between EE and relapse is
shown. When we adopted 3 CCs as the cutoff point, the
9-month relapse risk was 100% (3/3) for the high EE
group and 0% (0/9) for the low EE group (Fisher’s exact
test p = 0.005), with 100% sensitivity and specificity.
Two of the 3 were defined as having relapsed into a
manic state, and 1 as having relapsed into a depressive
state. When we used only CCs for the analysis, the result
was the same as in Ta b l e 4 . A similar analysis only for
EOI was impossible because of the small number of the
subjects scoring 2 or 3 for EOI.
4. DISCUSSION
We will briefly review the previous literature. Miklowitz
et al. conducted a cohort study to investigate the associ-
ation between the course of bipolar disorder and EE,
affective style, and lithium therapy among 24 patients [7].
Table 3. Comparison of past episodes by high and low EE.
Depressive Manic Total numbers
Mean (range)
Low EE (n = 9) 1.7 (1 - 3) 1.9 (1 - 6) 3.6 (2 - 8)
High EE (n = 3)* 1 (1 - 1) 2 (1 - 4) 3 (2 - 5)
High EE: (3 or more CC) or (3 or more EOI); CC: Critical comments; EOI:
Emotional overinvolvement.
*in detail
High EE (n = 3)*
Depressive Manic Total
Case 1 1 1 2
Case 2 1 4 5
Case 3 1 1 2
Table 4. Families’ EE and relapse of bipolar disorder.
Relapse (%)
None Relapsed
Total
Low 7 (100) 0 (0) 7
High 2 (40) 3 (60) 5 EEE1*1
Total 9 (75) 3 (25) 12
Low 9 (100) 0 (0) 9
High 0 (0) 3 (100) 3 EEE2*2
Total 9 (75) 3 (25) 12
*1p = 0.045 by Fisher’s exact test, sensitivity = 100%, specificity = 77.8%.
*2p = 0.005 by Fisher’s exact test, sensitivity = 100%, specificity = 100%;
High EE1: (1 or more CC) or (3 or more EOI); High EE2: (3 or more CC) or
(3 or more EOI); CC: Critical comments; EOI: Emotional overinvolvement.
They found a positive association between the families’
EE and relapse. Priebe et al. also conducted a cohort
study in 21 patients with bipolar and schizoaffective dis-
orders treated by lithium [8]. They observed an associa-
tion between EE and relapse. Kim et al. studied the ef-
fects of families’ EE on the course of 125 bipolar disor-
dered patients [17]. They followed-up the patients for 2
years, and found no relationship between EE and relapse.
In these 3 studies, the families’ EE was evaluated by CFI.
On the other hand, Yan et al. used FMSS (Five-Minute
Speech Sample) and conducted a 1-year cohort study
among bipolar I disordered patients [18]. They found that
the families’ EE was related to depressive relapse.
These previous studies suggest that the family envi-
ronment as evaluated by EE affects the course of bipolar
disorders, although one study showed negative findings.
In the current study, we support these findings and sub-
mit the first report from East Asia, where different cul-
tures and religions exist.
Concerning the CC cut-off point, the validity was best
when the subjects were divided between 3 or more and 2
or less. In this case, both sensitivity and specificity were
100%. However Miklowitz et al. used 6 CC as the cut-
off point [7]. This means that, in Japan, the CC cut-off
point for high EE should be changed, as families’ emo-
tional expression may be less salient in this culture.
If the high EE group has experienced more previous
manic/depressive episodes than the control group, this
would explain the current results. However, we found no
evidence for it (Table 3).
As the relapse during the follow-up period, in the high
EE group, 2 out of 3 were defined as having relapsed
into a manic state, and 1 into a depressive state. Because
of the small number of subjects, we could not find alter-
native reason for the 2 types of relapse.
Finally, we will discuss the limitations of the current
study. 1) Small sample size: We could not examine the
EE’s effect on the bipolar I disorder compared to the
bipolar II disorder; 2) The subjects were inpatients. There-
fore, the findings might be valid only among more se-
verely affected patients. Because the number of outpa-
tients is larger than that of inpatients, further studies are
required in outpatients including those with bipolar II
disorder. Also studies with adolescents are required since
this study was conducted mainly on middle-aged patients
[19].
5. ACKNOWLEDGEMENTS
The authors express their thanks to the patients and their families who
kindly participated in this study, and to Dr. Koichiro Sudo, Tosa Hospi-
tal for his assistance and discussion. This study was partly funded by a
grant-in-aid for scientific research (B) from the Japan Ministry of Edu-
Copyright © 2012 SciRes. OPEN ACCESS