Obstructive Azoospermia in a Patient with VATER Association
160
(a)
(b)
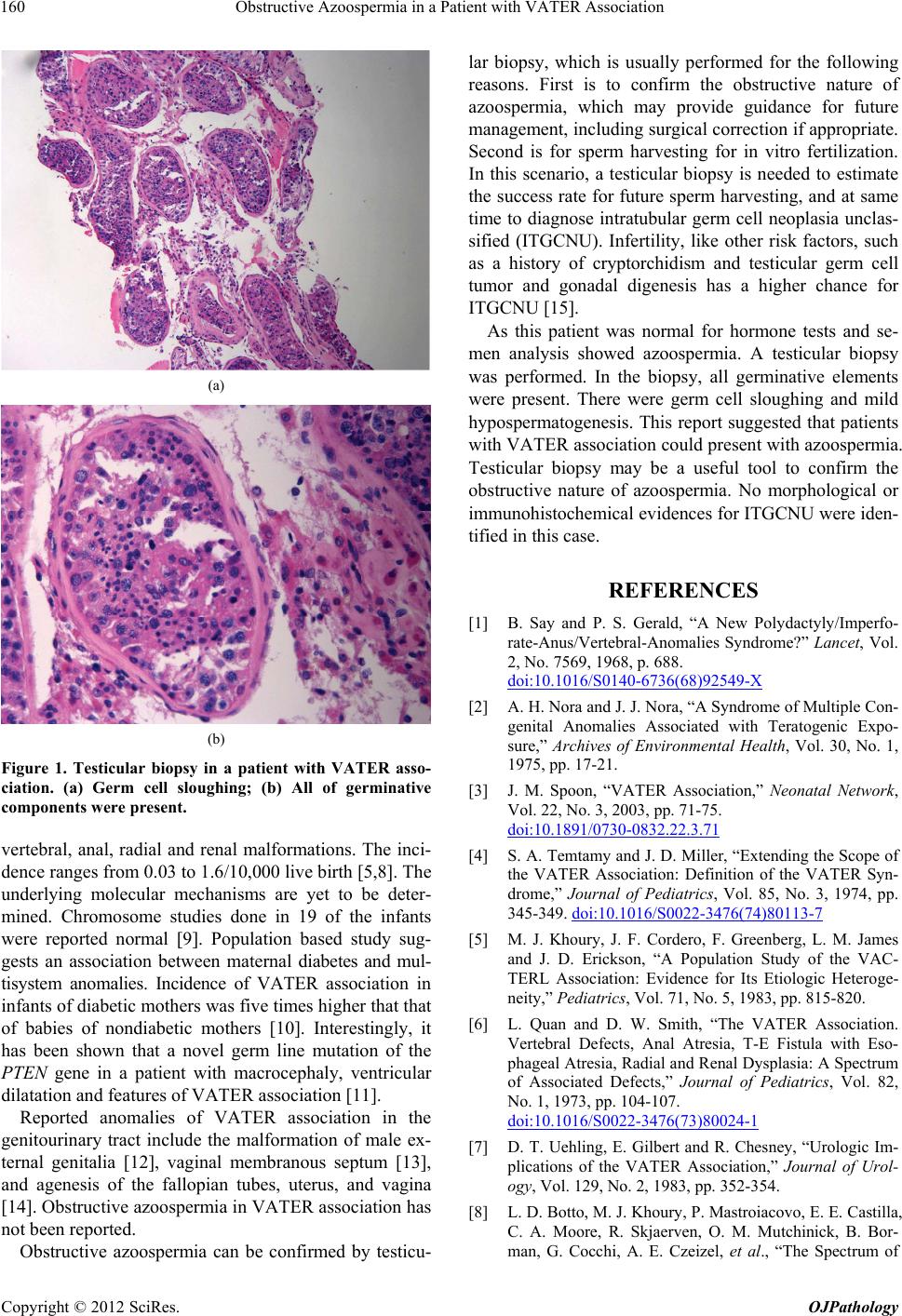
Figure 1. Testicular biopsy in a patient with VATER asso-
ciation. (a) Germ cell sloughing; (b) All of germinative
components were present.
vertebral, anal, radial and renal malformations. The inci-
dence ranges from 0.03 to 1.6/10,000 live birth [5,8]. The
underlying molecular mechanisms are yet to be deter-
mined. Chromosome studies done in 19 of the infants
were reported normal [9]. Population based study sug-
gests an association between maternal diabetes and mul-
tisystem anomalies. Incidence of VATER association in
infants of diabetic mothers was five times high er that that
of babies of nondiabetic mothers [10]. Interestingly, it
has been shown that a novel germ line mutation of the
PTEN gene in a patient with macrocephaly, ventricular
dilatation and features of VATER association [11].
Reported anomalies of VATER association in the
genitourinary tract include the malformation of male ex-
ternal genitalia [12], vaginal membranous septum [13],
and agenesis of the fallopian tubes, uterus, and vagina
[14]. Obstructive azoospermia in VATER association has
not been reported.
Obstructive azoospermia can be confirmed by testicu-
lar biopsy, which is usually performed for the following
reasons. First is to confirm the obstructive nature of
azoospermia, which may provide guidance for future
management, including surgical correction if appropriate.
Second is for sperm harvesting for in vitro fertilization.
In this scenario, a testicular biopsy is needed to estimate
the success rate for future sperm harvesting, and at same
time to diagnose intratubular germ cell neoplasia unclas-
sified (ITGCNU). Infertility, like other risk factors, such
as a history of cryptorchidism and testicular germ cell
tumor and gonadal digenesis has a higher chance for
ITGCNU [15].
As this patient was normal for hormone tests and se-
men analysis showed azoospermia. A testicular biopsy
was performed. In the biopsy, all germinative elements
were present. There were germ cell sloughing and mild
hypospermatogenesis. This report suggested that patients
with VATER association could present with azoospermia.
Testicular biopsy may be a useful tool to confirm the
obstructive nature of azoospermia. No morphological or
immunohistochemical evidences for ITGCNU were iden-
tified in this case.
REFERENCES
[1] B. Say and P. S. Gerald, “A New Polydactyly/Imperfo-
rate-Anus/Vertebral-Anomalies Syndrome?” Lancet, Vol.
2, No. 7569, 1968, p. 688.
doi:10.1016/S0140-6736(68)92549-X
[2] A. H. Nora and J. J. Nora, “A Syndrome of Multiple Con-
genital Anomalies Associated with Teratogenic Expo-
sure,” Archives of Environmental Health, Vol. 30, No. 1,
1975, pp. 17-21.
[3] J. M. Spoon, “VATER Association,” Neonatal Network,
Vol. 22, No. 3, 2003, pp. 71-75.
doi:10.1891/0730-0832.22.3.71
[4] S. A. Temtamy and J. D. Miller, “Extending the Scope of
the VATER Association: Definition of the VATER Syn-
drome,” Journal of Pediatrics, Vol. 85, No. 3, 1974, pp.
345-349. doi:10.1016/S0022-3476(74)80113-7
[5] M. J. Khoury, J. F. Cordero, F. Greenberg, L. M. James
and J. D. Erickson, “A Population Study of the VAC-
TERL Association: Evidence for Its Etiologic Heteroge-
neity,” Pediatrics, Vol. 71, No. 5, 1983, pp. 815-820.
[6] L. Quan and D. W. Smith, “The VATER Association.
Vertebral Defects, Anal Atresia, T-E Fistula with Eso-
phageal Atresia, Radial and Renal Dysplasia: A Spectrum
of Associated Defects,” Journal of Pediatrics, Vol. 82,
No. 1, 1973, pp. 104-107.
doi:10.1016/S0022-3476(73)80024-1
[7] D. T. Uehling, E. Gilbert and R. Chesney, “Urologic Im-
plications of the VATER Association,” Journal of Urol-
ogy, Vol. 129, No. 2, 1983, pp. 352-354.
[8] L. D. Botto, M. J. Khoury, P. Mastroiacovo, E. E. Castilla,
C. A. Moore, R. Skjaerven, O. M. Mutchinick, B. Bor-
man, G. Cocchi, A. E. Czeizel, et al., “The Spectrum of
Copyright © 2012 SciRes. OJPathology

