Diffuse Large B-Cell Lymphoma with Anaplastic Clear Cells: A Rare Variant 153
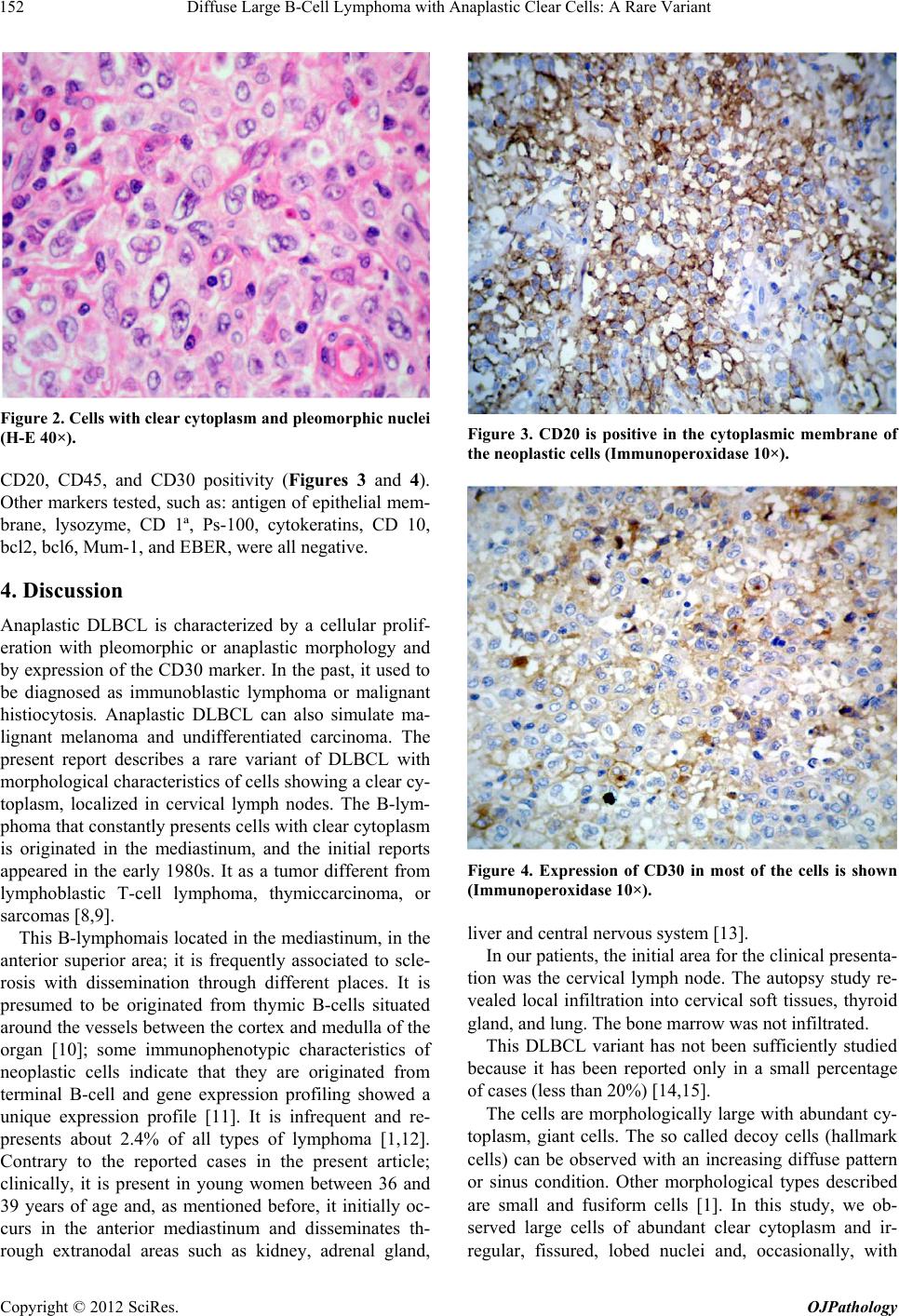
visible nucleolus. Among neoplastic cells, small lym-
phocytes and limited collagen fibers were observed. De-
coy cells were not visible in any of the two samples. By
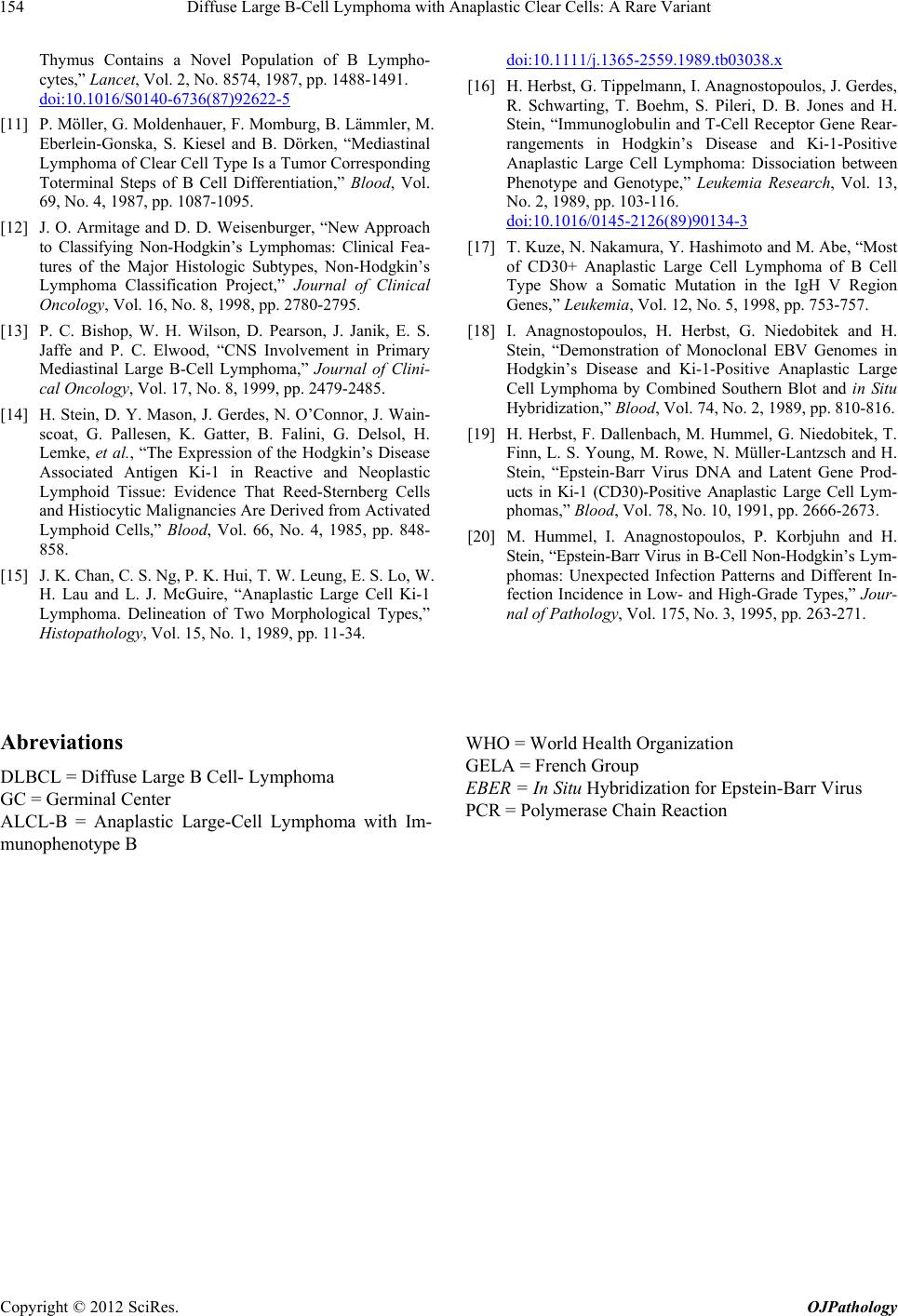
definition, neoplastic cells display expression of B mark-
ers such as CD19, CD20, and CD22 combined with
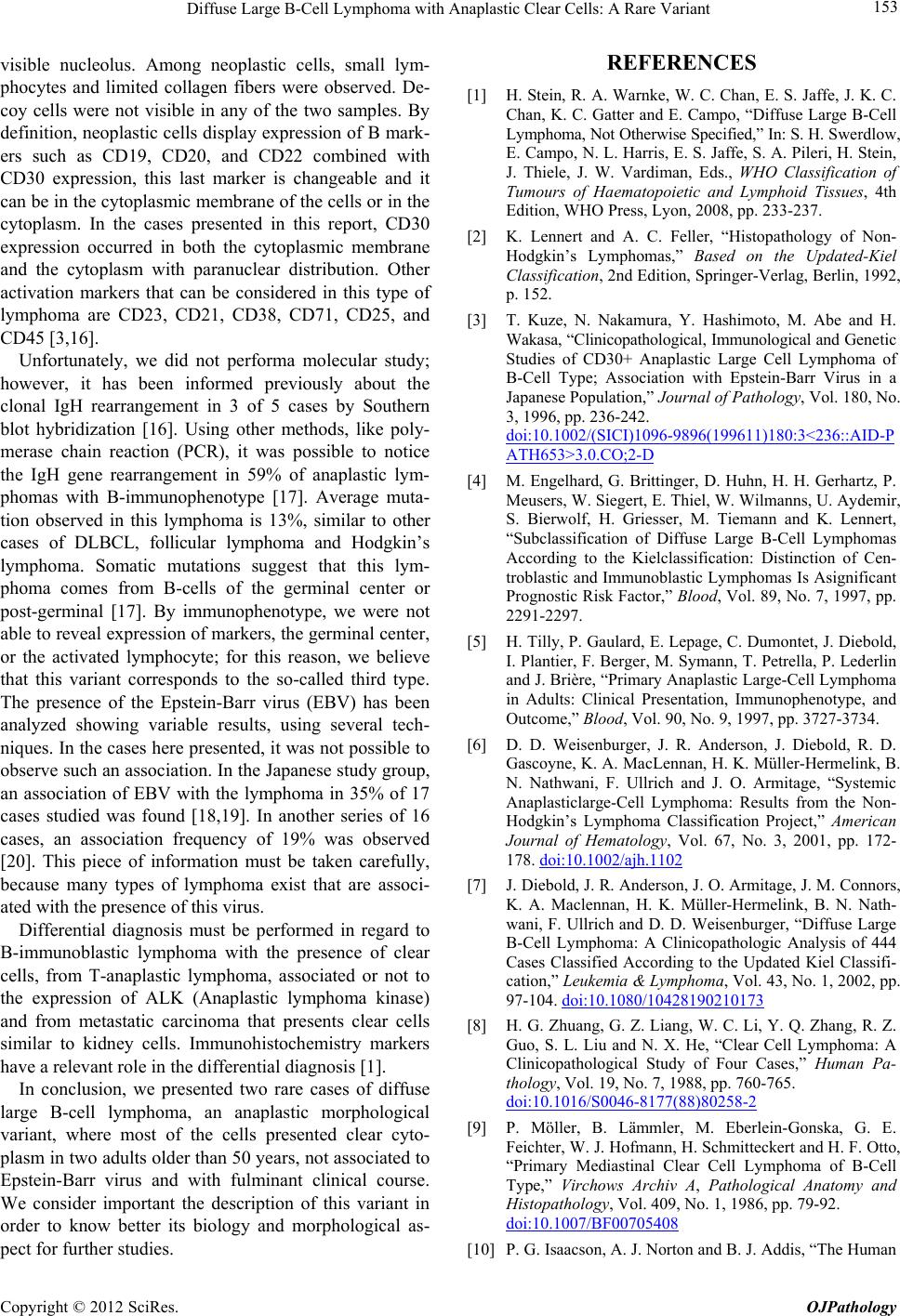
CD30 expression, this last marker is changeable and it
can be in the cytoplasmic membrane of the cells or in the
cytoplasm. In the cases presented in this report, CD30
expression occurred in both the cytoplasmic membrane
and the cytoplasm with paranuclear distribution. Other
activation markers that can be considered in this type of
lymphoma are CD23, CD21, CD38, CD71, CD25, and
CD45 [3,16].
Unfortunately, we did not performa molecular study;
however, it has been informed previously about the
clonal IgH rearrangement in 3 of 5 cases by Southern
blot hybridization [16]. Using other methods, like poly-
merase chain reaction (PCR), it was possible to notice
the IgH gene rearrangement in 59% of anaplastic lym-
phomas with B-immunophenotype [17]. Average muta-
tion observed in this lymphoma is 13%, similar to other
cases of DLBCL, follicular lymphoma and Hodgkin’s
lymphoma. Somatic mutations suggest that this lym-
phoma comes from B-cells of the germinal center or
post-germinal [17]. By immunophenotype, we were not
able to reveal expression of markers, the germinal center,
or the activated lymphocyte; for this reason, we believe
that this variant corresponds to the so-called third type.
The presence of the Epstein-Barr virus (EBV) has been
analyzed showing variable results, using several tech-
niques. In the cases here presented, it was not possible to
observe such an association. In the Japanese study group,
an association of EBV with the lymphoma in 35% of 17
cases studied was found [18,19]. In another series of 16
cases, an association frequency of 19% was observed
[20]. This piece of information must be taken carefully,
because many types of lymphoma exist that are associ-
ated with the presence of this virus.
Differential diagnosis must be performed in regard to
B-immunoblastic lymphoma with the presence of clear
cells, from T-anaplastic lymphoma, associated or not to
the expression of ALK (Anaplastic lymphoma kinase)
and from metastatic carcinoma that presents clear cells
similar to kidney cells. Immunohistochemistry markers
have a relevant role in the differential diagnosis [1].
In conclusion, we presented two rare cases of diffuse
large B-cell lymphoma, an anaplastic morphological
variant, where most of the cells presented clear cyto-
plasm in two adults older than 50 years, not associated to
Epstein-Barr virus and with fulminant clinical course.
We consider important the description of this variant in
order to know better its biology and morphological as-
pect for further studies.
REFERENCES
[1] H. Stein, R. A. Warnke, W. C. Chan, E. S. Jaffe, J. K. C.
Chan, K. C. Gatter and E. Campo, “Diffuse Large B-Cell
Lymphoma, Not Otherwise Specified,” In: S. H. Swerdlow,
E. Campo, N. L. Harris, E. S. Jaffe, S. A. Pileri, H. Stein,
J. Thiele, J. W. Vardiman, Eds., WHO Classification of
Tumours of Haematopoietic and Lymphoid Tissues, 4th
Edition, WHO Press, Lyon, 2008, pp. 233-237.
[2] K. Lennert and A. C. Feller, “Histopathology of Non-
Hodgkin’s Lymphomas,” Based on the Updated-Kiel
Classification, 2nd Edition, Springer-Verlag, Berlin, 1992,
p. 152.
[3] T. Kuze, N. Nakamura, Y. Hashimoto, M. Abe and H.
Wakasa, “Clinicopathological, Immunological and Genetic
Studies of CD30+ Anaplastic Large Cell Lymphoma of
B-Cell Type; Association with Epstein-Barr Virus in a
Japanese Population,” Journal of Pathology, Vol. 180, No.
3, 1996, pp. 236-242.
doi:10.1002/(SICI)1096-9896(199611)180:3<236::AID-P
ATH653>3.0.CO;2-D
[4] M. Engelhard, G. Brittinger, D. Huhn, H. H. Gerhartz, P.
Meusers, W. Siegert, E. Thiel, W. Wilmanns, U. Aydemir,
S. Bierwolf, H. Griesser, M. Tiemann and K. Lennert,
“Subclassification of Diffuse Large B-Cell Lymphomas
According to the Kielclassification: Distinction of Cen-
troblastic and Immunoblastic Lymphomas Is Asignificant
Prognostic Risk Factor,” Blood, Vol. 89, No. 7, 1997, pp.
2291-2297.
[5] H. Tilly, P. Gaulard, E. Lepage, C. Dumontet, J. Diebold,
I. Plantier, F. Berger, M. Symann, T. Petrella, P. Lederlin
and J. Brière, “Primary Anaplastic Large-Cell Lymphoma
in Adults: Clinical Presentation, Immunophenotype, and
Outcome,” Blood, Vol. 90, No. 9, 1997, pp. 3727-3734.
[6] D. D. Weisenburger, J. R. Anderson, J. Diebold, R. D.
Gascoyne, K. A. MacLennan, H. K. Müller-Hermelink, B.
N. Nathwani, F. Ullrich and J. O. Armitage, “Systemic
Anaplasticlarge-Cell Lymphoma: Results from the Non-
Hodgkin’s Lymphoma Classification Project,” American
Journal of Hematology, Vol. 67, No. 3, 2001, pp. 172-
178. doi:10.1002/ajh.1102
[7] J. Diebold, J. R. Anderson, J. O. Armitage, J. M. Connors,
K. A. Maclennan, H. K. Müller-Hermelink, B. N. Nath-
wani, F. Ullrich and D. D. Weisenburger, “Diffuse Large
B-Cell Lymphoma: A Clinicopathologic Analysis of 444
Cases Classified According to the Updated Kiel Classifi-
cation,” Leukemia & Lymphoma, Vol. 43, No. 1, 2002, pp.
97-104. doi:10.1080/10428190210173
[8] H. G. Zhuang, G. Z. Liang, W. C. Li, Y. Q. Zhang, R. Z.
Guo, S. L. Liu and N. X. He, “Clear Cell Lymphoma: A
Clinicopathological Study of Four Cases,” Human Pa-
thology, Vol. 19, No. 7, 1988, pp. 760-765.
doi:10.1016/S0046-8177(88)80258-2
[9] P. Möller, B. Lämmler, M. Eberlein-Gonska, G. E.
Feichter, W. J. Hofmann, H. Schmitteckert and H. F. Otto,
“Primary Mediastinal Clear Cell Lymphoma of B-Cell
Type,” Virchows Archiv A, Pathological Anatomy and
Histopathology, Vol. 409, No. 1, 1986, pp. 79-92.
doi:10.1007/BF00705408
[10] P. G. Isaacson, A. J. Norton and B. J. Addis, “The Human
Copyright © 2012 SciRes. OJPathology