Plexiform Angiomyxoid Myofibroblastic Tumor of the Stomach 149
genesis and histology. However, the WHO classification
of tumors of the digestive system accepted “plexiform
fibromyxoma” as a diagnostic term instead of PAMT [6].
PAMT of the stomach is a very rare tumor without
distinctive clinical manifestations. Symptoms may in-
clude those of ulceration, hematemesis and anemia. Our
patient presented with intermittent epigastric discomfort
and abdominal pain. The endoscopist usually encounters
a submucosal-based or nodular mass. A very striking
feature is the almost exclusive location in the gastric an-
trum. The mucosa may be intact, dimpled or ulcerated.
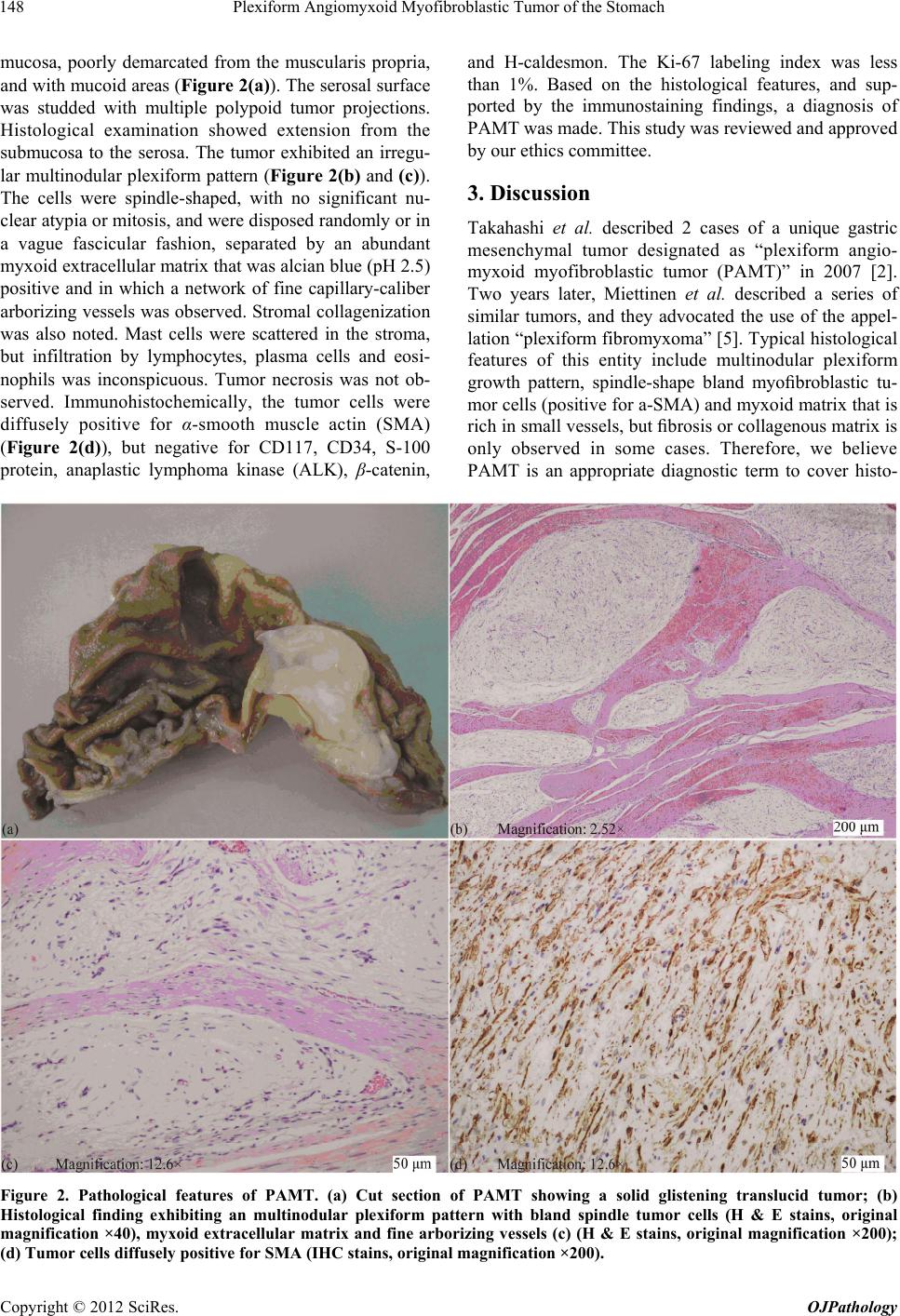
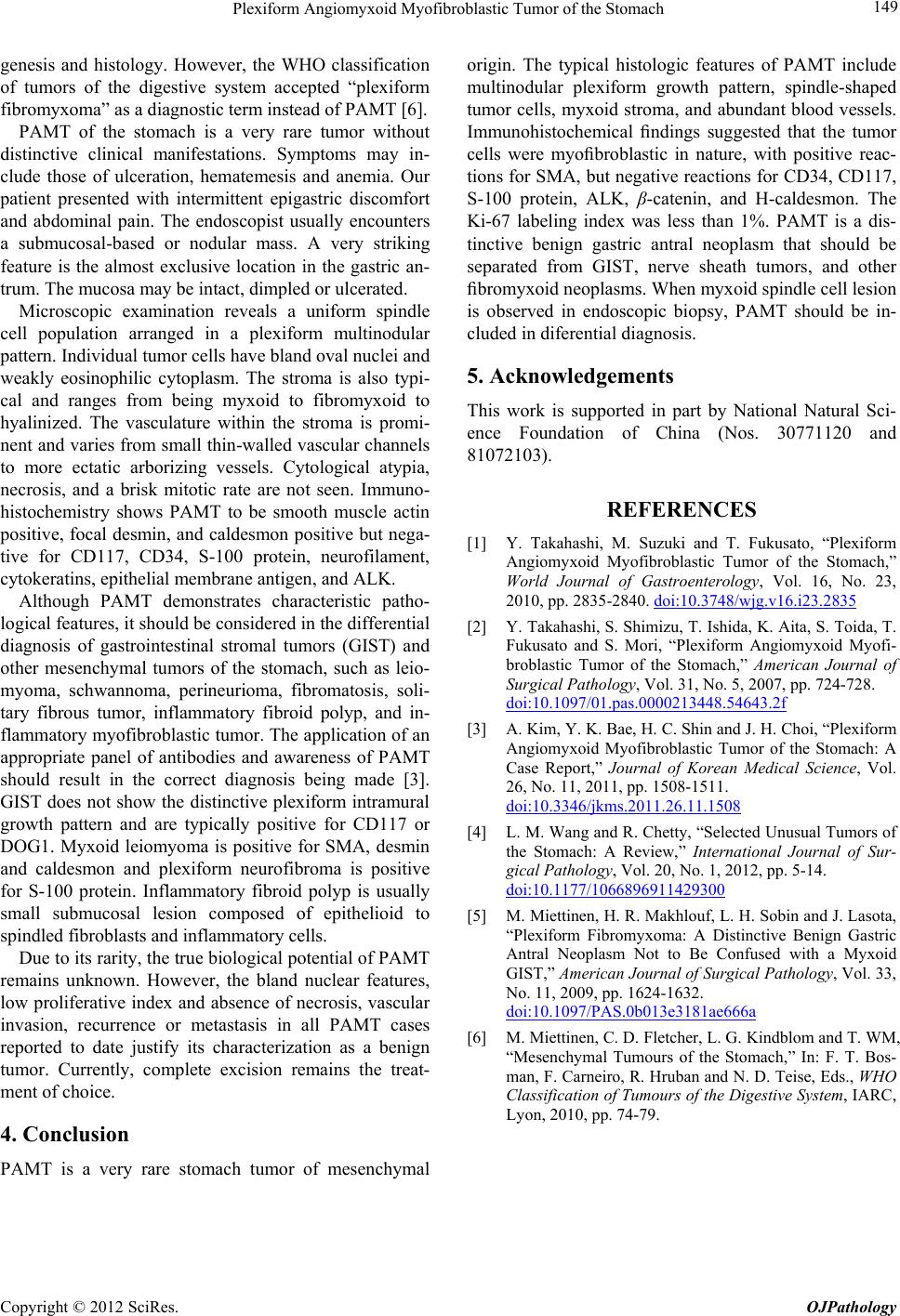
Microscopic examination reveals a uniform spindle
cell population arranged in a plexiform multinodular
pattern. Individual tumor cells have bland oval nuclei and
weakly eosinophilic cytoplasm. The stroma is also typi-
cal and ranges from being myxoid to fibromyxoid to
hyalinized. The vasculature within the stroma is promi-
nent and varies from small thin-walled vascular channels
to more ectatic arborizing vessels. Cytological atypia,
necrosis, and a brisk mitotic rate are not seen. Immuno-
histochemistry shows PAMT to be smooth muscle actin
positive, focal desmin, and caldesmon positive but nega-
tive for CD117, CD34, S-100 protein, neurofilament,
cytokeratins, epith elial membrane antigen, and ALK.
Although PAMT demonstrates characteristic patho-
logical features, it should be considered in the differential
diagnosis of gastrointestinal stromal tumors (GIST) and
other mesenchymal tumors of the stomach, such as leio-
myoma, schwannoma, perineurioma, fibromatosis, soli-
tary fibrous tumor, inflammatory fibroid polyp, and in-
flammatory myofibrob lastic tumor. The application of an
appropriate panel of antibodies and awareness of PAMT
should result in the correct diagnosis being made [3].
GIST does not show the distinctive plexiform intramural
growth pattern and are typically positive for CD117 or
DOG1. Myxoid leiomyoma is positive for SMA, desmin
and caldesmon and plexiform neurofibroma is positive
for S-100 protein. Inflammatory fibroid polyp is usually
small submucosal lesion composed of epithelioid to
spindled fibroblasts and inflamma tory cells.
Due to its rarity, the true biological potential o f PAMT
remains unknown. However, the bland nuclear features,
low proliferative index and absence of necrosis, vascular
invasion, recurrence or metastasis in all PAMT cases
reported to date justify its characterization as a benign
tumor. Currently, complete excision remains the treat-
ment of choice.
4. Conclusion
PAMT is a very rare stomach tumor of mesenchymal
origin. The typical histologic features of PAMT include
multinodular plexiform growth pattern, spindle-shaped
tumor cells, myxoid stroma, and abundant blood vessels.
Immunohistochemical findings suggested that the tumor
cells were myofibroblastic in nature, with positive reac-
tions for SMA, but negative reactions for CD34, CD117,
S-100 protein, ALK, β-catenin, and H-caldesmon. The
Ki-67 labeling index was less than 1%. PAMT is a dis-
tinctive benign gastric antral neoplasm that should be
separated from GIST, nerve sheath tumors, and other
fibromyxoid neoplasms. When myxoid spindle cell lesion
is observed in endoscopic biopsy, PAMT should be in-
cluded in diferential diagnosis.
5. Acknowledgements
This work is supported in part by National Natural Sci-
ence Foundation of China (Nos. 30771120 and
81072103).
REFERENCES
[1] Y. Takahashi, M. Suzuki and T. Fukusato, “Plexiform
Angiomyxoid Myofibroblastic Tumor of the Stomach,”
World Journal of Gastroenterology, Vol. 16, No. 23,
2010, pp. 2835-2840. doi:10.3748/wjg.v16.i23.2835
[2] Y. Takahashi, S. Shimizu, T. Ishida, K. Aita, S. Toida, T.
Fukusato and S. Mori, “Plexiform Angiomyxoid Myofi-
broblastic Tumor of the Stomach,” American Journal of
Surgical Pathology, Vol. 31, No. 5, 2007, pp. 724-728.
doi:10.1097/01.pas.0000213448.54643.2f
[3] A. Kim, Y. K. Bae, H. C. Shin and J. H. Choi, “Plexiform
Angiomyxoid Myofibroblastic Tumor of the Stomach: A
Case Report,” Journal of Korean Medical Science, Vol.
26, No. 11, 2011, pp. 1508-1511.
doi:10.3346/jkms.2011.26.11.1508
[4] L. M. Wang and R. Chetty, “Selected Unusual Tumors of
the Stomach: A Review,” International Journal of Sur-
gical Pathology, Vol. 20, No. 1, 2012, pp. 5-14.
doi:10.1177/1066896911429300
[5] M. Miettinen, H. R. Makhlouf, L. H. Sobin and J. Lasota,
“Plexiform Fibromyxoma: A Distinctive Benign Gastric
Antral Neoplasm Not to Be Confused with a Myxoid
GIST,” American Journal of Surgical Pathology, Vol. 33,
No. 11, 2009, pp. 1624-1632.
doi:10.1097/PAS.0b013e3181ae666a
[6] M. Miettinen, C. D. Fletcher, L. G. Kindblom and T. WM,
“Mesenchymal Tumours of the Stomach,” In: F. T. Bos-
man, F. Carneiro, R. Hruban and N. D. Teise, Eds., WHO
Classification of Tumours of the Digestive System, IARC,
Lyon, 2010, pp. 74-79.
Copyright © 2012 SciRes. OJPathology