A Case Report of an Inverted Papilloma of the Prostatic Urethra and a Synchronous
Low-Grade Papillary Carcinoma of the Bladder
Copyright © 2012 SciRes. OJPathology
142
3. Discussion
Inverted papilloma of the urinary tract is a rare benign
tumor most commonly diagnosed in older men present-
ing with hematuria or symptoms of lower urinary tract
obstruction [3,4]. It is most frequently identified in the
bladder neck or trigone as a polypoid growth with a
smooth surface. These lesions are usually small (<3 cm)
but can be large. Most are solitary although 1% - 4%
may be multifocal.
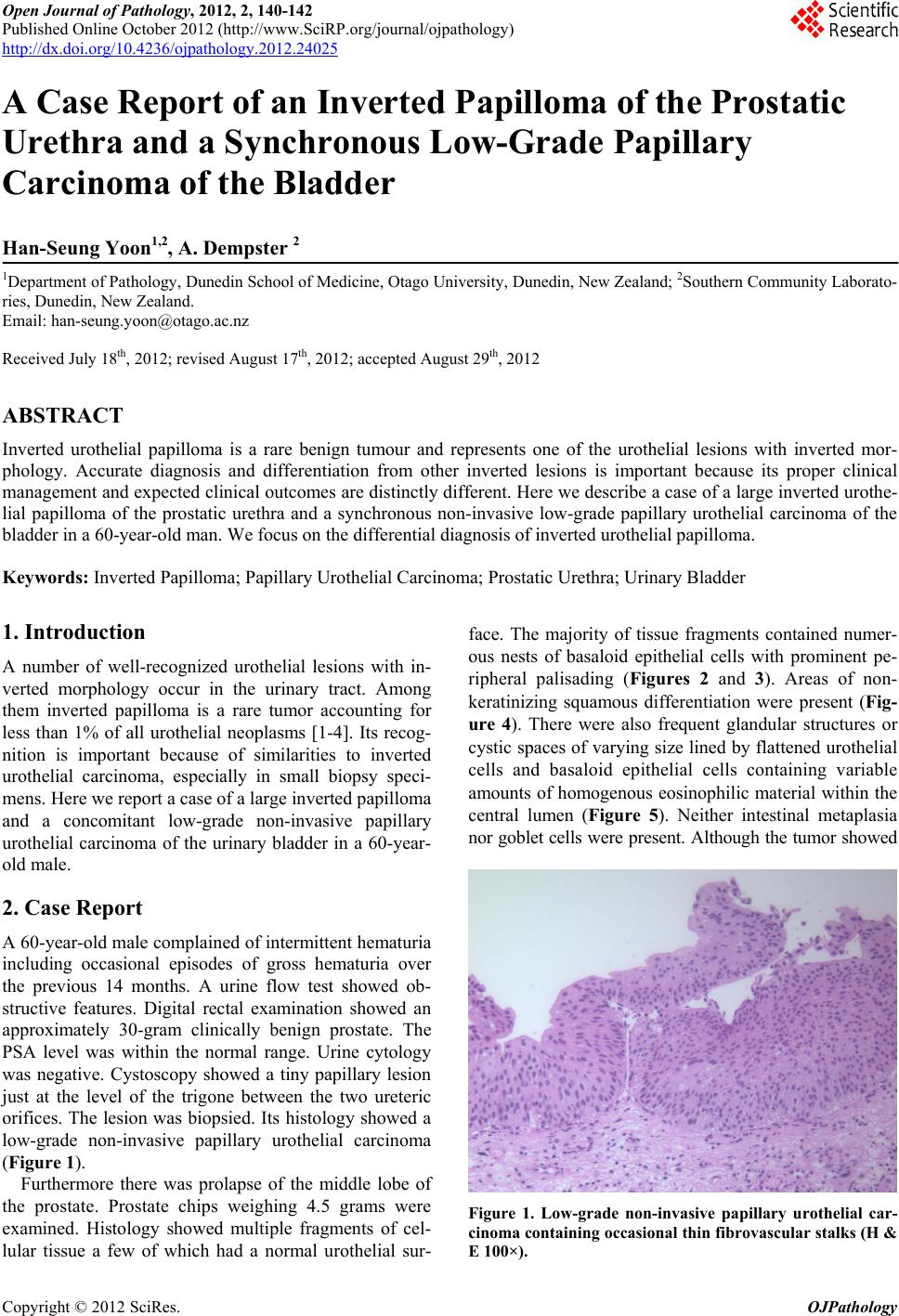
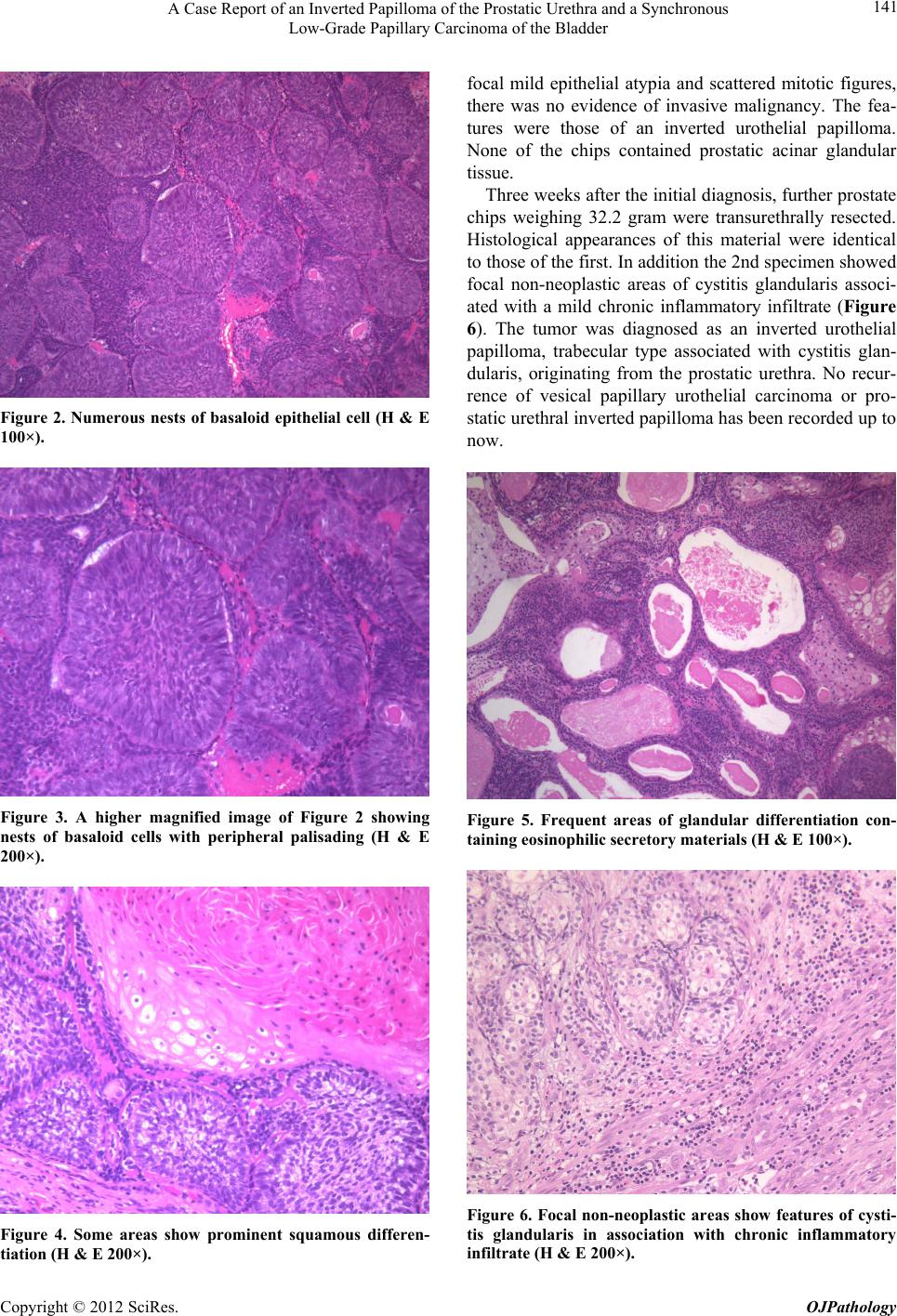
Histologically there are two main subtypes of inverted
papillomas; trabecular and glandular [1]. The former is
characterized by widely branched, anastomosing cords of
urothelial cells originating directly from the overlying
transitional epithelium. The latter is characterized by
multiple round to oval islands of proliferating urothelial
cells together with pseudoglandular and true glandular
structures, which are often connected with the surface
urothelium.
Although inverted papilloma is generally regarded to
be a benign neoplasm, sporadic cases of inverted papil-
loma with malignant features have been reported raising
concern that inverted papilloma may be a precursor le-
sion of utorhelial malignancy [5-8]. However most of
these patients had a history of previous or concurrent
urothelial carcinoma. Inverted papilloma is associated
with a low risk of recurrence (5%), in marked contrast to
the high recurrence rates of papillary urothelial carci-
noma [3]. Sung et al. [2] reported only one recurrence
among 75 patients with inverted papilloma (1.3%) during
a mean follow-up of 68 months after treatment. The au-
thors recommend that complete transurethral resection
appears to be adequate surgical therapy for inverted
papilloma [2].
The present case showed an inverted papilloma of the
prostatic urethra and a synchronous low-grade non-inva-
sive papillary urothelial carcinoma of the bladder. Spo-
radic cases with inverted papilloma have been reported to
show metachronous or synchronou s urothelial carcinoma.
Brown and Cohen in a series of 41 cases of inverted
papilloma reported 2 patients (4.9%) had a history of
urothelial carcinoma and one of the 2 (2.4%) was diag-
nosed with concomitant urothelial carcinoma [4]. The
authors recommend ed postoperativ e surveillance because
2 patients developed urothelial carcinoma among 25 pa-
tients during a 9 - 25 months cystoscopic follow-up for
non-recurrent inverted papilloma.
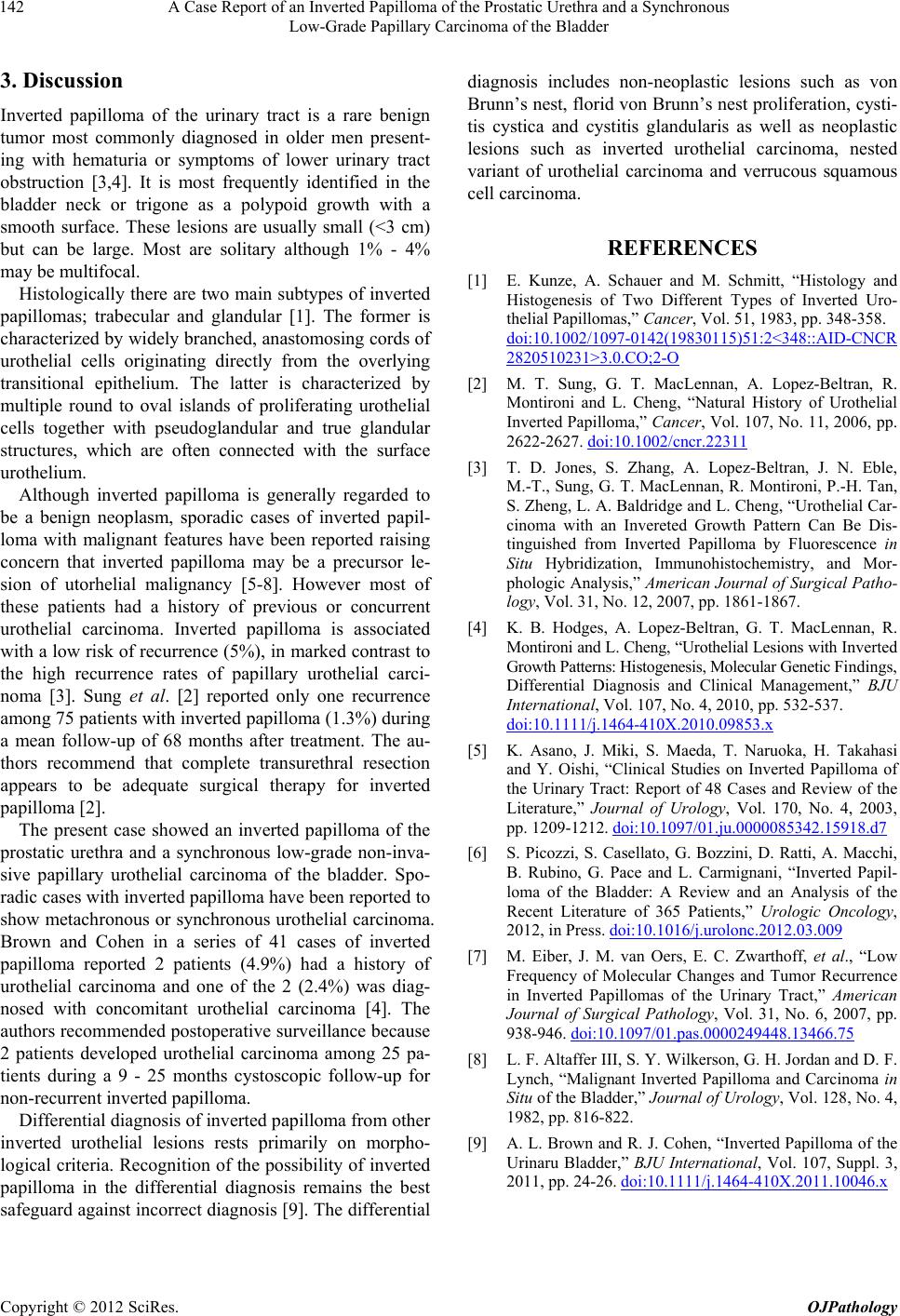
Differential diagnosis of inverted papilloma from other
inverted urothelial lesions rests primarily on morpho-
logical criteria. Recognition of the possibility o f inverted
papilloma in the differential diagnosis remains the best
safeguard against incorrect diagnosis [9]. The differential
diagnosis includes non-neoplastic lesions such as von
Brunn’s nest, florid von Brunn’s nest proliferation, cysti-
tis cystica and cystitis glandularis as well as neoplastic
lesions such as inverted urothelial carcinoma, nested
variant of urothelial carcinoma and verrucous squamous
cell carcinoma.
REFERENCES
[1] E. Kunze, A. Schauer and M. Schmitt, “Histology and
Histogenesis of Two Different Types of Inverted Uro-
thelial Pa pillomas,” Cancer, Vol. 51, 1983, pp. 348-358.
doi:10.1002/1097-0142(19830115)51:2<348::AID-CNCR
2820510231>3.0.CO;2-O
[2] M. T. Sung, G. T. MacLennan, A. Lopez-Beltran, R.
Montironi and L. Cheng, “Natural History of Urothelial
Inverted Papilloma,” Cancer, Vol. 107, No. 11, 2006, pp.
2622-2627. doi:10.1002/cncr.22311
[3] T. D. Jones, S. Zhang, A. Lopez-Beltran, J. N. Eble,
M.-T., Sung, G. T. MacLennan, R. Montironi, P.-H. Tan,
S. Zheng, L. A. Baldridge and L. Cheng, “Urothelial Car-
cinoma with an Invereted Growth Pattern Can Be Dis-
tinguished from Inverted Papilloma by Fluorescence in
Situ Hybridization, Immunohistochemistry, and Mor-
phologic Analysis,” American Journal of Surgical Patho-
logy, Vol. 31, No. 12, 2007, pp. 1861-1867.
[4] K. B. Hodges, A. Lopez-Beltran, G. T. MacLennan, R.
Montironi and L. Cheng, “Urothel ial Lesions with In v e rt e d
Growth Patterns: Histogenesis, Molecular Genetic Findings,
Differential Diagnosis and Clinical Management,” BJU
International, Vol. 107, No. 4, 2010, pp. 532-537.
doi:10.1111/j.1464-410X.2010.09853.x
[5] K. Asano, J. Miki, S. Maeda, T. Naruoka, H. Takahasi
and Y. Oishi, “Clinical Studies on Inverted Papilloma of
the Urinary Tract: Report of 48 Cases and Review of the
Literature,” Journal of Urology, Vol. 170, No. 4, 2003,
pp. 1209-1212. doi:10.1097/01.ju.0000085342.15918.d7
[6] S. Picozzi, S. Casellato, G. Bozzini, D. Ratti, A. Macchi,
B. Rubino, G. Pace and L. Carmignani, “Inverted Papil-
loma of the Bladder: A Review and an Analysis of the
Recent Literature of 365 Patients,” Urologic Oncology,
2012, in Press. doi:10.1016/j.urolonc.2012.03.009
[7] M. Eiber, J. M. van Oers, E. C. Zwarthoff, et al., “Low
Frequency of Molecular Changes and Tumor Recurrence
in Inverted Papillomas of the Urinary Tract,” American
Journal of Surgical Pathology, Vol. 31, No. 6, 2007, pp.
938-946. doi:10.1097/01.pas.0000249448.13466.75
[8] L. F. Altaffer III, S. Y. Wilkerson, G. H. Jordan and D. F.
Lynch, “Malignant Inverted Papilloma and Carcinoma in
Situ of the Bladder,” Journal of Urology, Vol. 128, No. 4,
1982, pp. 816-822.
[9] A. L. Brown and R. J. Cohen, “Inverted Papilloma of the
Urinaru Bladder,” BJU International, Vol. 107, Suppl. 3,
2011, pp. 24-26. doi:10.1111/j.1464-410X.2011.10046.x