Paper Menu >>
Journal Menu >>
 J. Biomedical Science and Engineering, 2010, 3, 811-815 JBiSE doi:10.4236/jbise.2010.38108 Published Online August 2010 (http://www.SciRP.org/journal/jbise/). Published Online August 2010 in SciRes. http://www.scirp.org/journal/jbise Shoulder joint flexibility in top athletes Hassan Daneshmandi*, Farhad Rahmaninia, Hossein Shahrokhi, Pegah Rahmani, Saeid Esmaeili Guilan University, Rasht, Iran. Email: Danesh@guilan.ac.ir, Daneshmandi_ph@yahoo.com Received 17 April 2010; revised 17 May 2010; accepted 22 May 2010. ABSTRACT Joint range of motion (ROM) is very important in daily activities, sport and in clinical diagnosis. Many factors have been reported to influence joint ROM. Muscu- loskeletal adaptation and some special side effects due to his or her physical demands and movement patterns in professional athletes are very important subjects in sport sciences. The present study is a comparison of shoulder joint ROM in elite athlete and non-athlete groups and its relationship to their age, post and years of their tournament play. The subjects in this study included 106 men with mean age (23.65 ± 3.45) and mean years of tournament play (5.60 ± 2.23). The groups of subjects included 26 handball players, 25 volleyball players, 25 soccer players and 30 non-athletes. Data were collected through questionnaires and inspection, and subjects’ ROM was measured by “Leighton flex- ometer” (r = 0.90 – 0.99) in external rotation and ab- duction of shoulder joint in dominant and non-domi- nant hands. Data were analyzed by correlation coeffi- cient, t – test, ANOVA and post hock Schaffe test. The results showed that an increase in age and years of tournament play reduced the shoulder ROM of sub- jects (p ≤ 0.05). There were significant differences in shoulder ROM among athletic groups. Additionally, there are significant differences between dominant and non-dominant hands (p ≤ 0.05). It can be concluded that more specific stretching exercises and warm-up for shoulder in all athletes and especially in older and ex- perienced players should be performed by coaches. The results also emphasized routine screening, corrective exercise programs and a design of preventing strategies by athletic trainers and coaches. Keywords: Range of Motion; Shoulder Joint; Handball; Volleyball; Soccer; Age; Years of Tournament Play; Playing Post 1. INTRODUCTION Joint range of motion (ROM) data is a very important reference in job and workplace design as well as in clinical diagnosis. Many factors have been reported to influence joint ROM. With an increase in age, the de- generation in these tissues becomes progressively more apparent, and results in a reduction in joint ROM. Other factors such as pain, dominant side, and the time of day may also have effects on joint ROM [1]. The physical demands of sport performance on the athletes’ body cause certain musculoskeletal adaptation. Professional athletes spend most of their sporting life in training and competition [2]. Load placed on the musculoskeletal system may be generally classified as tensile or com- pressive. Repeated demands on a musculotendinous unit may cause it to shorten, decreasing normal joint range of motion [3]. Musculoskeletal adaptation and some special side effects due to his or her physical demands and movement patterns in professional athletes are very im- portant subjects in sport sciences. The musculoskeletal adaptation at this point is called maladaptation, reducing joint range of motion, changing biomechanical patterns, decreasing the efficiency of force production, and in- creasing the chance of injuries to the musculoskeletal system [4]. Faulty posture could be also the result of that adaptation [5]. However, faulty posture does not neces- sarily indicate a disorder but it could cause a loss of op- timum body mechanics [6]. There is a general agreement that the appropriate amount of exercise is important for the healthy growth and optimal development of the body [7]. By contrast, too much or too little exercise and inappropriate training may have some adverse effects [8]. Overtraining is an imbalance between training and recovery. This term is not new. The symptoms of prolonged fatigue, loss of motivation, burn out and staleness have been described in athletes for many decades. They are the maladaptive responses to the stimulus of training and an extended period of overload. Maladaptation flexibility due to fre- quent and old injuries has been recognized for some time [9]. Each sport has specific patterns of movement which has an effect on related joint range of motion (ROM) because skeletal tissue possesses an intrinsic ability to  812 H. Daneshmandi et al. / J. Biomedical Science and Engineering 3 (2010) 811-815 Copyright © 2010 SciRes. JBiSE adapt to these physical activities. Adaptations take place in response to exercise training and those specific pat- terns of movements. In general, exercise programs usu- ally include strength, power, endurance and flexibility training. In shoulder researches, measurements of range of motion (ROM) have been used as outcome measures in the vast majority of reported trials [10]. Therefore, the present study was proposed to compare the range of mo- tion of shoulder joint (ROM) in elite athlete and non-athlete groups and its relationship to their age, post and years of tournament play. 2. METHODOLOGY The subjects of this study were members of league teams with more than 2 years of play in league competitions. These subjects included 106 men with mean age (23.65 ± 3.45) and mean of participation in tournament play (5.60 ± 2.23). The groups of subjects included 26 hand- ball players (mean age 23.57 ± 2.67, mean playing his- tory 6.38 ± 2.07), 25 volleyball players (mean age 22.8 ±4.31, mean playing history 4.56 ± 2.43), 25 soccer players (mean age 25.08 ± 2.53, mean playing history 5.84 ± 1.84) and 30 non-athletes (mean age 23.23 ± 3.71). The players completed questionnaires about age, play- ing post, past or current shoulder injuries, duration of dominant and non-dominant glenohumeral joints were made by Leighton flexometer (r = 0.90 – 0.99) in stan- dard position. Goniometric measurement of the gle- nohumeral join is difficult because of the multi-join na- ture of the shoulder complex. In general, the literature would appear to indicate that the Leighton flexometer is a reliable measuring tool, especially when used by a sin- gle experienced tester. All ROMs of subjects were measured in the morning and before play or participating in warm-up drills. No goniometric measurements were taken in the afternoon or after participating in play or warm-up drills to mini- mize the effect of intense activity or play on range of motion. All testing took place with the subject in a stan- dard position in special bar and plastic cast and stabi- lized scapula by three special wide tapes on the hip, chest and head areas. Shoulder external and internal ro- tations were measured with the arm positioned in 90° of glenohumeral abduction and 90° of elbow flexion. Dur- ing testing, the subjects were asked to actively move the joint as far as possible through the range of motion (Graph 1). For each direction, three measurements were taken and the mean measurements were calculated. We performed t- test on dominant versus non-dominant hands of subjects for all measurements. Correlation co- efficients were computed to determine the strength of the relationships among variables. We analyzed these groups Graph 1. Flexion & hyper extension measurements posi- tion (photo from Ackland et al. [6]). and the relationship between shoulder ROM and age, post and history of play were analyzed by ANOVA and Post hock Scheffe test. 2.1. Reliability of the Measuring Method The commonly used clinical methods for detecting mus- cle tightness, described by Kendall [11] are subjective. When precision and objectivity are needed, estimation of range of motion by eye (eyeballing) is too inaccurate and therefore a goniometer was used in this research. Also, standardized methods of joint motion measurement by American academy of orthopedic surgeons (AAOS) 1966 and others were advised [12]. The measuring de- vice is always important. In addition to the accuracy of a measuring device, an instrument should be easy to be used by the tester and comfortable for the subjects. Cer- tain joint movements, especially axial rotations are more difficult to measure than others and that with a standard universal goniometer, axial measurements are only ap- proximates [13]. In this study all ROMs were measured with the Leighton flexometer, model WA, Spokan because it was valid, reliable, easy to use and it has been frequently used by other researchers. There are sufficient studies to prove the reliability of the Leighton flexometer: Lei- ghton [14], Bloomfield et al. [6], and Daneshmandi [3]. The reliability and validity of this device were proved by the researchers. Ekstrand et al. [15] also used the Leighton flexometer to measure the hip ROM in soccer players. 3. RESULTS The results of the present study showed that the volleyball players were also less flexible than other soccer players and non-athlete groups for internal rotation (p ≤ 0.05). The results of this study showed significant differences of ROM of medial rotation of the shoulder in the four 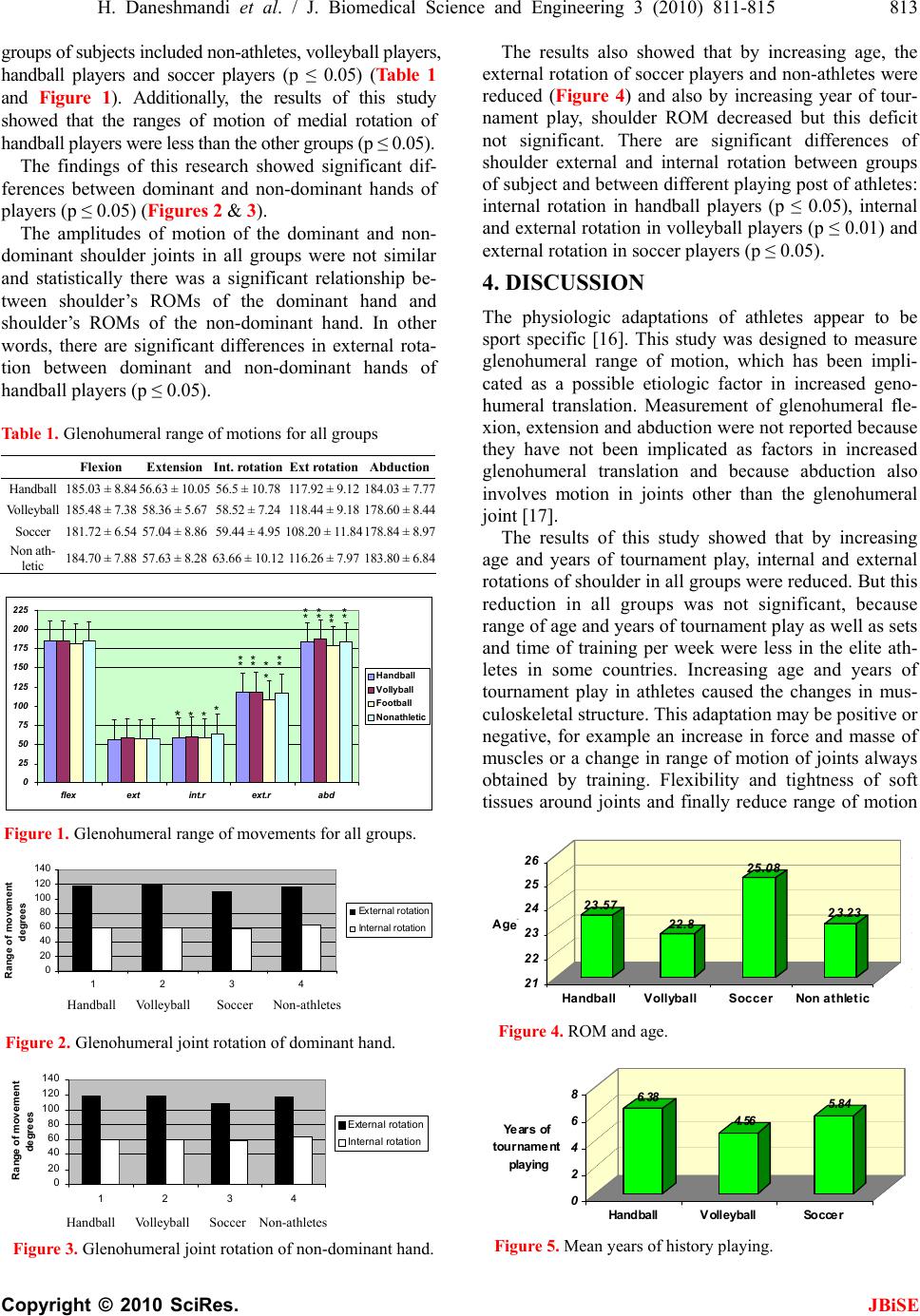 H. Daneshmandi et al. / J. Biomedical Science and Engineering 3 (2010) 811-815 813 Copyright © 2010 SciRes. JBiSE groups of subjects included non-athletes, volleyball players, handball players and soccer players (p ≤ 0.05) (Table 1 and Figure 1). Additionally, the results of this study showed that the ranges of motion of medial rotation of handball players were less than the other groups (p ≤ 0.05). The findings of this research showed significant dif- ferences between dominant and non-dominant hands of players (p ≤ 0.05) (Figures 2 & 3). The amplitudes of motion of the dominant and non- dominant shoulder joints in all groups were not similar and statistically there was a significant relationship be- tween shoulder’s ROMs of the dominant hand and shoulder’s ROMs of the non-dominant hand. In other words, there are significant differences in external rota- tion between dominant and non-dominant hands of handball players (p ≤ 0.05). Table 1. Glenohumeral range of motions for all groups Flexion Extension Int. rotation Ext rotation Abduction Handball 185.03 ± 8.84 56.63 ± 10.05 56.5 ± 10.78 117.92 ± 9.12 184.03 ± 7.77 Volleyball 185.48 ± 7.38 58.36 ± 5.67 58.52 ± 7.24 118.44 ± 9.18 178.60 ± 8.44 Soccer 181.72 ± 6.54 57.04 ± 8.86 59.44 ± 4.95 108.20 ± 11.84178.84 ± 8.97 Non ath- letic 184.70 ± 7.88 57.63 ± 8.28 63.66 ± 10.12 116.26 ± 7.97 183.80 ± 6.84 0 25 50 75 100 125 150 175 200 225 flexextint.r ext.rabd Handball Vollyball Football Non ath letic **** * ** ** ** * * ** ** ** * Figure 1. Glenohumeral range of movements for all groups. 0 20 40 60 80 100 120 140 1234 Range of movement degrees External rot ation Int e rnal rotation Handball Volleyball Soccer Non-athletes Figure 2. Glenohumeral joint rotation of dominant hand. 0 20 40 60 80 100 120 140 1234 Range of movement degrees External rotation Internal rotation Handball Volleyball Soccer Non-athletes Figure 3. Glenohumeral joint rotation of non-dominant hand. The results also showed that by increasing age, the external rotation of soccer players and non-athletes were reduced (Figure 4) and also by increasing year of tour- nament play, shoulder ROM decreased but this deficit not significant. There are significant differences of shoulder external and internal rotation between groups of subject and between different playing post of athletes: internal rotation in handball players (p ≤ 0.05), internal and external rotation in volleyball players (p ≤ 0.01) and external rotation in soccer players (p ≤ 0.05). 4. DISCUSSION The physiologic adaptations of athletes appear to be sport specific [16]. This study was designed to measure glenohumeral range of motion, which has been impli- cated as a possible etiologic factor in increased geno- humeral translation. Measurement of glenohumeral fle- xion, extension and abduction were not reported because they have not been implicated as factors in increased glenohumeral translation and because abduction also involves motion in joints other than the glenohumeral joint [17]. The results of this study showed that by increasing age and years of tournament play, internal and external rotations of shoulder in all groups were reduced. But this reduction in all groups was not significant, because range of age and years of tournament play as well as sets and time of training per week were less in the elite ath- letes in some countries. Increasing age and years of tournament play in athletes caused the changes in mus- culoskeletal structure. This adaptation may be positive or negative, for example an increase in force and masse of muscles or a change in range of motion of joints always obtained by training. Flexibility and tightness of soft tissues around joints and finally reduce range of motion 23.57 22.8 25.08 23.23 21 22 23 24 25 26 Ageَ HandballVollyballSoccerNon athletic Figure 4. ROM and age. 6.38 4.56 5.84 0 2 4 6 8 Ye ars of tourname nt pla ying Handball VolleyballSoccer Figure 5. Mean years of history playing.  814 H. Daneshmandi et al. / J. Biomedical Science and Engineering 3 (2010) 811-815 Copyright © 2010 SciRes. JBiSE of joints as well [18,19]. If the normal flexibility of the surrounding tissue of a joints is not maintained, over a period of time a decrease in joint range of motion could happen leading to a possible decrease in performance or an increase in chance of injury [4,5]. In this study, the range of external and internal shoulder rotations was different in sports and in play- ing posts of athletes, which can be related to their spe- cific sport demands and emphasizes this point that flexibility is very specific in any joint, playing post and sport field. Glenohumeral internal rotation of handball and volleyball players was less than other groups in this study. A reduction in shoulder internal rotation, particularly in the dominant side, can be ex- plained as an adaptation of the posterior shoulder musculature and capsular structure to the handball and volleyball stroke. The increase in external rotation of shoulder in these athletes is also a likely adaptation to the overhead movement in these sports. The occur- rence of an excessive range of external rotation may be a product of a successful training program to increase movement and thus the range over which force can be applied to throwing or stroke [19,20]. The implication of this point is that excessive external shoulder rotation can create excessive anterior humeral head displacement [17,21,22]. Current research has con- vincingly showed that deficits of internal rotation of shoulder occur as the athlete adapts to the demands of the sport. It is unclear whether these are normal adapta- tions that are beneficial, either locally or throughout the kinetic chain, or whether these are mal-adaptations that create potentially harmful local or kinetic chain biome- chanics. Also, the role this adaptation may play in injury causation or risk is unclear. Several recent papers sug- gest that decreased internal rotation and total rotation may adversely affect shoulder performance, and this effect may increase the risk of injury [22,23]. There are studies which show that inflexibility is a risk factor for further injury [24,25]. Achievement of full range of motion is one of the first goals in rehabilitation programs [20,22]. Most shoulder rehabilitation protocols now emphasize on a corrective exercise for internal rota- tion of shoulder of athletes. The study of water polo players showed that special repetitive movement in water polo is the same as base- ball and handball throwing, volleyball service and stroke and other sports with overhead movements. All these sports emphasize shoulder adduction and internal rota- tion that cause force, torque and mass of adductor and internal rotator muscles can lead to reduction of these ROMs [2,26]. The study of shoulder movement suggests that de- creased internal and total rotation may not be optimal conditions to allow the best athletic performance with minimal risk of injury. From a performance standpoint, these conditions create inefficient biomechanics that interfere with normal coupled motion and may decrease optimal arm momentum. This paper showed degrees of asymmetry in dominant and non-dominant hands of handball and volleyball players. If we do not note it carefully and do not use correct stretch exercise program, this imbalance in musculature of shoulder girdle leads the athletes to decrease their performance or an increase in the chance of injury. For example, Young et al. [27] reported a prevalence imbalance in musculature of shoulder girdle and scoliosis in volleyball players rather than in non-athletic groups. Improvement of imbalance musculature due to hard training created scoliosis in volleyball players. Therefore, if handball and volleyball players train more and harder bilaterally, this maladapta- tion will be rapid. 5. CONCLUSIONS Once again the results of this research showed the limi- tation of shoulder ROM in athletes. On the basis of this study and other investigations, it could be suggested that the specific demands, poor training, particularly lack of adequate flexibility exercises and inadequate warm-up exercises for shoulder, may be responsible for such problems. Exercising muscles without an appropriate stretching exercise program tends to decrease the motion in shoulder joints. Very importantly, the overall (contact or non-contact sports), hard and stressful competitions, over-training, exhausting repeated movements, faulty techniques, pre- vious injuries and probably anthropometric characteris- tics of players can be also considered as other factors involved in the limitation of shoulder flexibility. How- ever, each factor will need more research. Also, it can be recommended that more stretching ex- ercises should be considered for older and experienced players and specific stretching exercises are recom- mended for different sports and playing posts. Based on the demands of any sport, coaches and athletes should apply corrective exercise programs to prevent muscular imbalance in shoulder girdle. Much more work is needed to study the exact implica- tions of our findings. Several directions for future study are raised by this study. Can these deficits be modified and, if so, what is the most efficient method of modifica- tion? If they are modified, what is the relationship be- tween performance and risk of injury? Do these deficits continue to decline in a linear direction, or is there a curvilinear pattern with an absolute maximum? Were these deficits compounded by variables such as the amount of weight training exercises and previous child- hood activities?  H. Daneshmandi et al. / J. Biomedical Science and Engineering 3 (2010) 811-815 815 Copyright © 2010 SciRes. JBiSE REFERENCES [1] Chung, M.-J. and Wang, M.-J.J. (2009) The effect of age and gender on joint range of motion of worker population in Taiwan. International Journal of Industrial Ergonom- ics, 39(4), 596-600. [2] Crockett, H.C. (2002) Osseus adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. American Journal of Sports Medicine, 30(1), 20-26. [3] Hassan, D. and Shacklady, C. (2002) Hip rotation flexi- bility in professional athletes. International Journal of Collected Acad emi c Articles , 1, 81. [4] Hall, S.J. and Martin, M. (2002) Sport injury manage- ment. Williams & Wilkins, Philadelphia. [5] Chandler. T.J., Kibler, W.B., Uhl, T.L., Wooten, B., Kiser, A. and Stone, E. (1990) Flexibility comparisons of junior elite tennis player to other athletes. American Journal of Sports Medicine, 18(2), 134-136. [6] Ackland, T.R., Elliott, B.C. and Bloomfield, J. (1995) Applied anatomy and biomechanics in sport. Human Ki- netics Publishers, Champaign. [7] Holland, G.J., et al. (2002) Flexibility and physical func- tions of older adults: A review. Journal of Aging and Physical A ctivi ty , 10(2), 169-206. [8] Kugler, A., Krüger-Franke, M., Reininger, S., Trouillier, H.H. and Rosemeyer, B. (1996) Muscular imbalance and shoulder pain in volleyball attackers. British Journal of Sports Medicine, 30(3), 256-259. [9] Alter, M.J. (1996) Science of stretching. Human Kinetics Publishers, Champaign. [10] Tveitå, E.K., et al. (2008) Range of shoulder motion in patients with adhesive capsulitis; Intra-tester reproduci- bility is acceptable for group comparisons. BMC Muscu- loskeletal Disorders, 9, 49. [11] Kendall, F., et al. (2005) Muscle testing and function with posture and pain. 5th Edition, Lippincott Williams & Wilkins Publisher, Philadelphia. [12] Norkin, C.C. and White, D.J. (1995) Measurement of joint motion: A guide to goniometry. 2nd Edition, F. A. Davis Company, Philadelphia. [13] Ellenbecker, T.S., et al. (1996) Glenohumeral joint inter- nal and external rotation range of motion in elite junior tennis players. Journal of Orthopaedic & Sports Physical Therapy, 24(6), 336-341. [14] Leighton, J.R. (1957) Flexibility characteristics of three specialized skill groups of champion athletes. Archives of Physical Medicine and Rehabilitation, 38(9), 580-583. [15] Ekstrand, J., et al. (1982) Lower extremity goniometric measurement: A study to determine their reliability. Ar- chives of Physical Medicine and Rehabilitation, 63(4), 171-175. [16] Harryman, D.T., et al. (1992) The role of the rotator in- terval capsule in passive motion and stability of the shoulder. The Journal of Bone and Joint Surgery, 74(1), 53-66. [17] Reagan, K.M., et al. (2002) Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball player. American Journal of Sports Medi - cine, 30(3), 354-360. [18] Leatt, P., et al. (1987) Specific muscular development in under-18 soccer player. Journal of Sports Sciences, 5(2), 165-175. [19] Herington, L., et al. (1998) Glenohumeral joint: Internal and external rotation range of motion in javelin throwers. British Journal of Sports Medicine, 32(3), 226-228. [20] Silliman, J.F. and Hawkins, R.J. (1991) Current concepts and recent advances in the athlete’s shoulder. Clinics in Sports Medicine, 10(4), 693-705. [21] Wilk, K.E., et al. (2002) Current concepts in the reha- bilitation of the overhead throwing athlete. American Journal of Sports Medicine, 30(1), 136-151. [22] Wilk, K.E., et al. (1997) Current concept: The stabilizing structures of the glenohumeral joint. Journal of Ortho- paedic & Sports Physical Therapy, 25(6), 364-379. [23] Kibler, W.B. (1995) Clinical examination of the shoulder: Athletic injuries of the shoulder. McGraw-Hill, Inc., New York. [24] Kibler, W.B., Chandler, T.J. and Pace, B.K. (1992) Prin- ciples of rehabilitation after chronic tendon injuries. Clin- ics in Sports Medicine, 11(3), 661-671. [25] Pieper, H.G. (1998) Humeral torsion in the throwing arm of handball players. American Journal of Sports Medi- cine, 26(2), 247-253. [26] McMaster, W.C., et al. (1992) Shoulder torque changes in the swimming athlete. American Journal of Sports Medicine, 20(3), 323-327. [27] Kim, Y.K., et al. (2003) The relationship between hu- meral retroversion and shoulder rotation in maggot league baseball pitchers. 5th Asian Federation of Sports Medicine Congress, Seoul, 15 September 2003. |