Indications and Outcomes for Pedicled Pectoralis Major Myocutaneous Flaps at a
Primary Microvascular Head and Neck Reconstructive Center
106
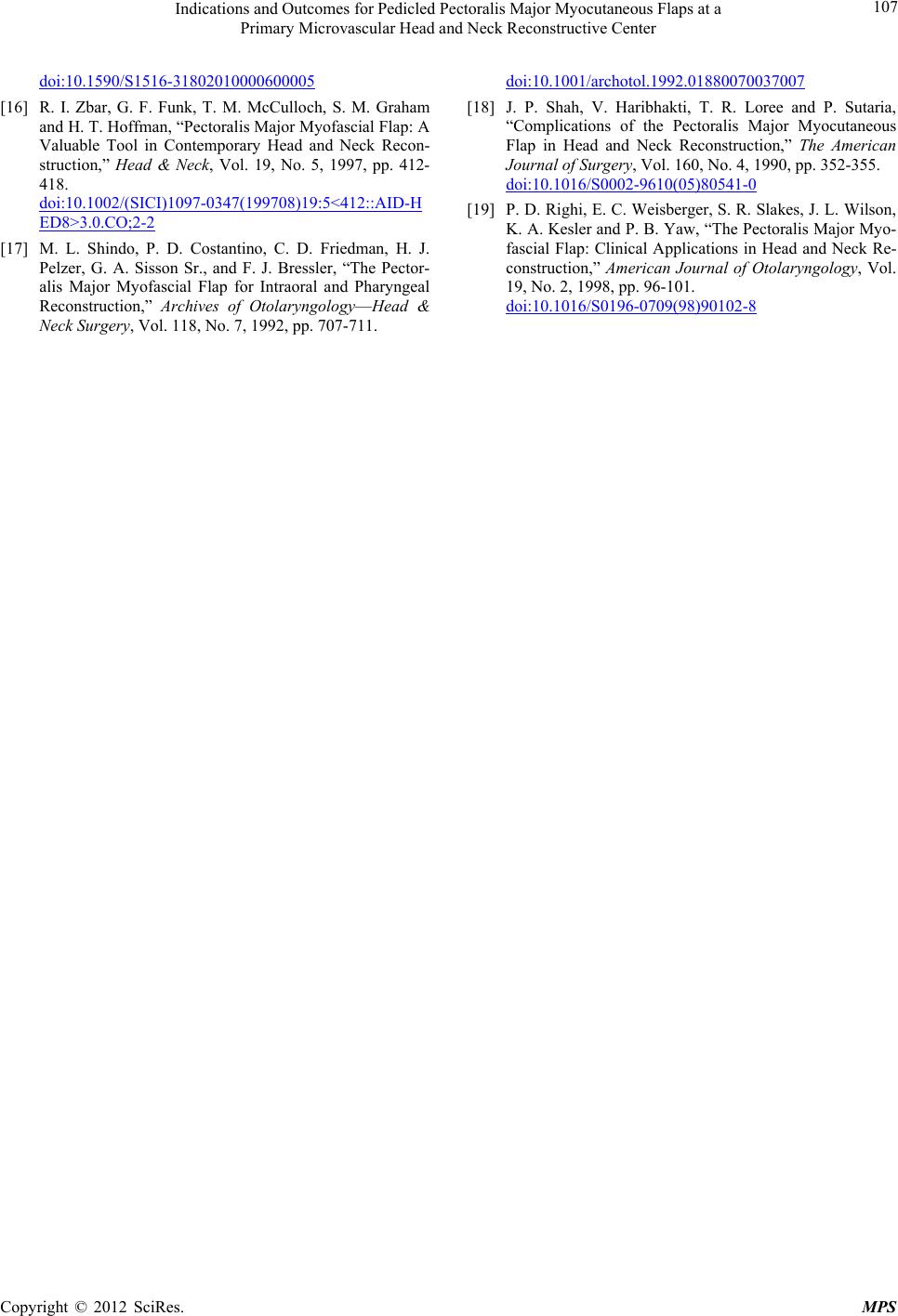
In our series, 5 out of the 6 patients (83%) who devel-
oped complications had a history of preoperative radio-
therapy, while only 1 of 6 patients (17%) who did not
develop complications had undergone preoperative ra-
diotherapy. However, this difference was not statistically
significant.
Three out of 5 patients with fistula had recurrences af-
ter the reconstructive procedures, with 2 of them devel-
oping fistula recurrence following partial flap loss. Since
many cases with fistula have a prior history of radiation,
which delays healing, when the primary indication of the
procedure is to repair a fistula, special care should be
taken to safely elevate the flap in order to minimize ne-
crosis.
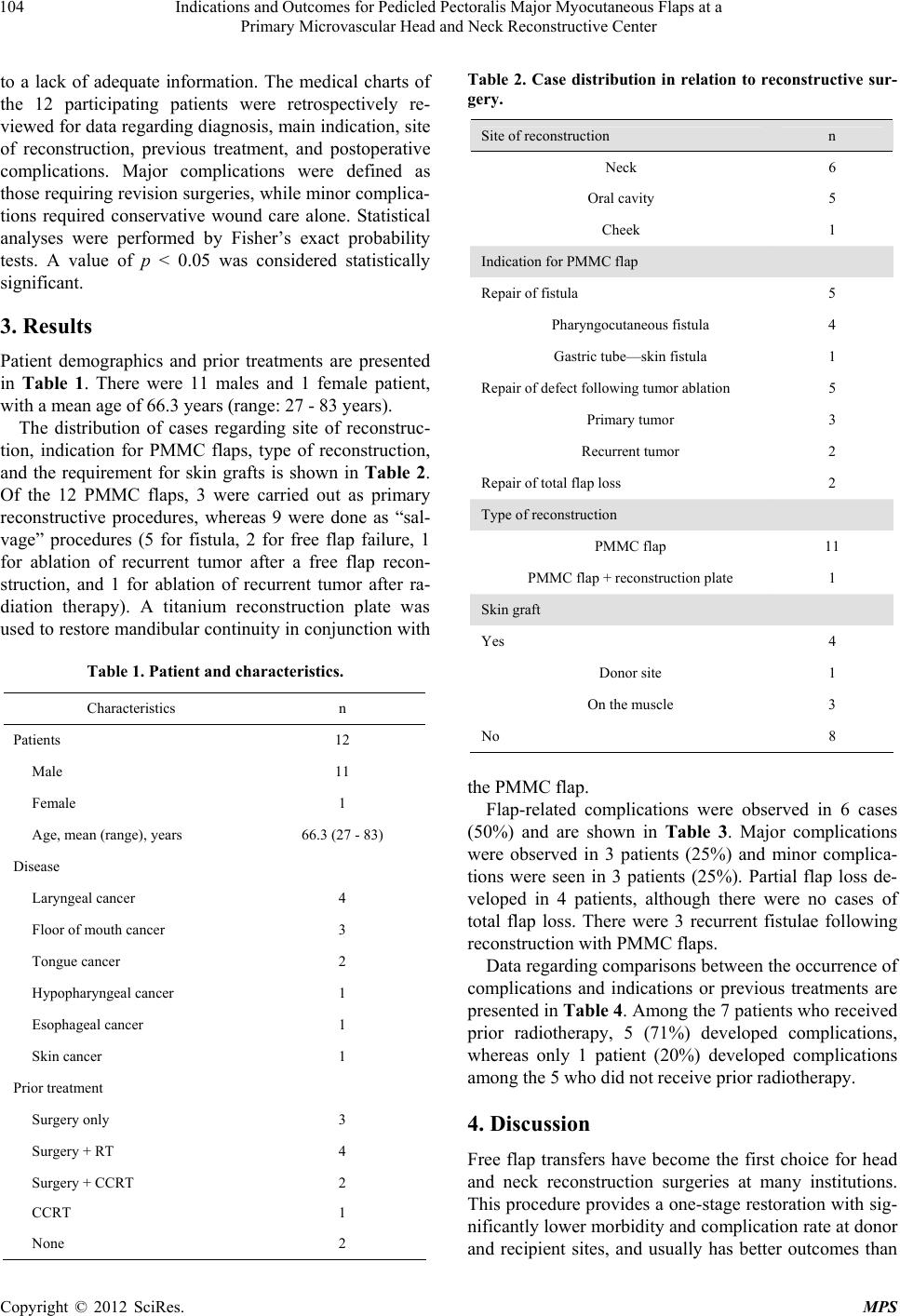
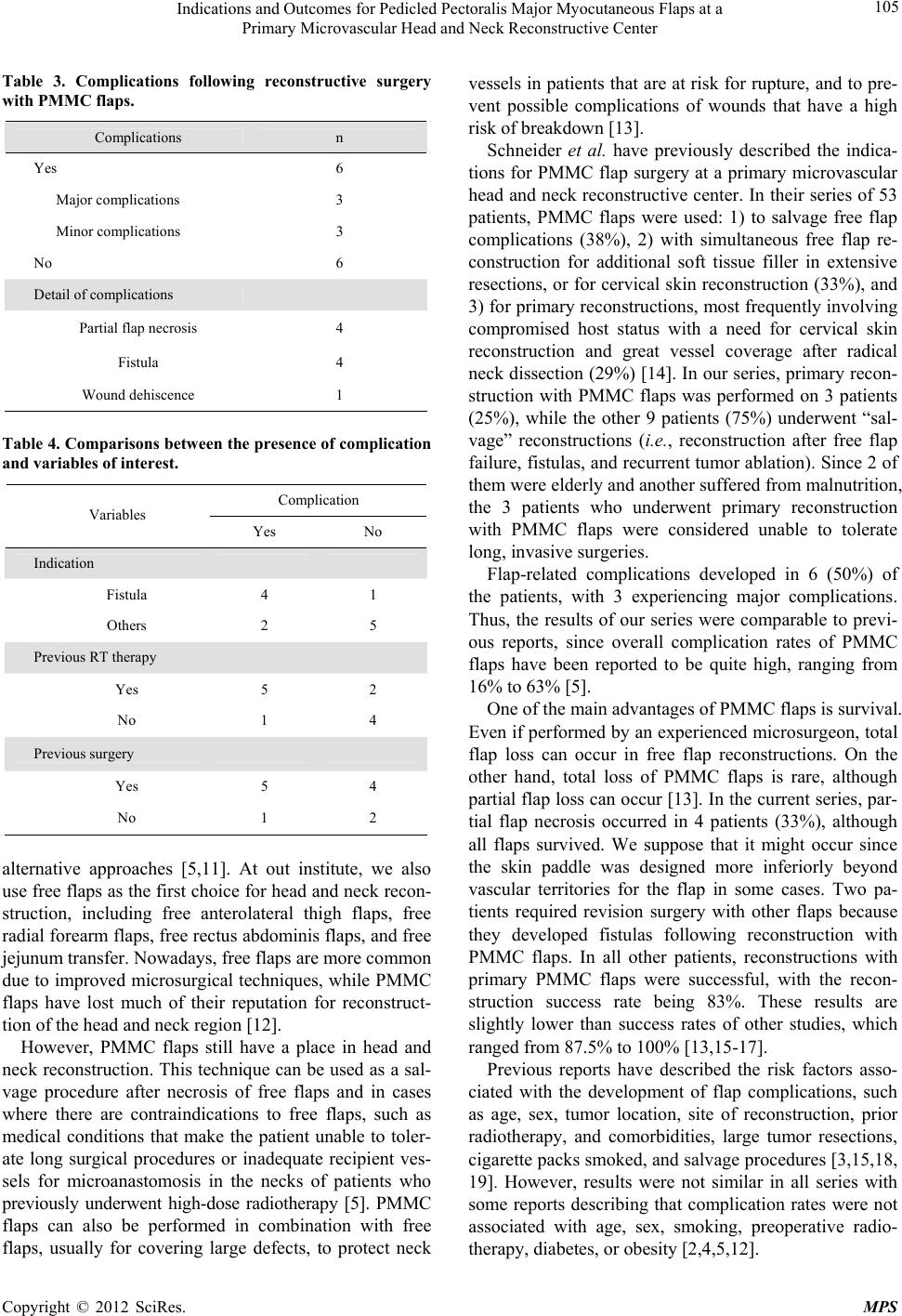
In conclusion, of 12 PMMC flap surgeries performed
at our institution, 3 were carried out as primary recon-
structive procedures, whereas 9 were done as “salvage”
procedures. Major complications were observed in 3 pa-
tients (25%), and minor complications were seen in 3
patients (25%). Partial flap loss developed in 4 patients
(33%), although there were no cases of total flap loss.
The preoperative goals of the flaps were met in 83% of
our cases.
5. Conclusion
The authors conclude that although free flap transfer is
most often the first choice for head and neck reconstruct-
tion, PMMC flaps can produce acceptable results in cer-
tain situations.
REFERENCES
[1] S. Ariyan, “The Pectoralis Major Myocutaneous Flap. A
Versatile Flap for Reconstruction in the Head and Neck,”
Plastic and Reconstructive Surgery, Vol. 63, No. 1, 1979,
pp. 73-81. doi:10.1097/00006534-197901000-00012
[2] I. J. CB, S. E. Hovius, B. L. ten Have, S. J. Wijthoff, G. J.
Sonneveld, C. A. Meeuwis and P. P. Knegt, “Is the Pec-
toralis Myocutaneous Flap in Intraoral and Oropharyngeal
Reconstruction Outdated?” The American Journal of Sur-
gery, Vol. 172, No. 3, 1996, pp. 259-262.
doi:10.1016/S0002-9610(96)00161-4
[3] S. Mehta, S. Sarkar, N. Kavarana, H. Bhathena and A.
Mehta, “Complications of the Pectoralis Major Myocuta-
neous Flap in the Oral Cavity: A Prospective Evaluation
of 220 Cases,” Plastic and Reconstructive Surgery, Vol.
98, No. 1, 1996, pp. 31-37.
doi:10.1097/00006534-199607000-00006
[4] R. Liu, P. Gullane, D. Brown and J. Irish, “Pectoralis
major Myocutaneous Pedicled Flap in Head and Neck
Reconstruction: Retrospective Review of Indications and
Results in 244 Consecutive Cases at the Toronto General
Hospital,” Journal of Otolaryngology, Vol. 30, No. 1,
2001, pp. 34-40. doi:10.2310/7070.2001.21011
[5] J. G. Vartanian, A. L. Carvalho, S. M. Carvalho, L.
Mizobe, J. Magrin and L. P. Kowalski, “Pectoralis Major
and Other Myofascial/Myocutaneous Flaps in Head and
Neck Cancer Reconstruction: Experience with 437 Cases
at a Single Institution,” Head & Neck, Vol. 26, No. 12,
2004, pp. 1018-1023. doi:10.1002/hed.20101
[6] A. L. McCrory and J. S. Magnuson, “Free Tissue Trans-
fer versus Pedicled Flap in Head and Neck Reconstruc-
tion.” Laryngoscope, Vol. 112, No. 12, 2002, pp. 2161-
2165. doi:10.1097/00005537-200212000-00006
[7] K. E. Blackwell, D. Buchbinder, H. F. Biller and M. L.
Urken, “Reconstruction of Massive Defects in the Head
and Neck: The Role of Simultaneous Distant and Re-
gional Flaps,” Head & Neck, Vol. 19, No. 7, 1997, pp.
620-628.
doi:10.1002/(SICI)1097-0347(199710)19:7<620::AID-H
ED10>3.0.CO;2-6
[8] C. Y. Hsing, Y. K. Wong, C. P. Wang, C. C. Wang, R. S.
Jiang, F. J. Chen and S. A. Liu, “Comparison between
Free Flap and Pectoralis Major Pedicled Flap for Recon-
struction in Oral Cavity Cancer Patients—A Quality of
Life Analysis,” Oral Oncology, Vol. 47, No. 6, 2011, pp.
522-527. doi:10.1016/j.oraloncology.2011.03.024
[9] D. B. Chepeha, G. Annich, M. A. Pynnonen, J. Beck, G.
T. Wolf, T. N. Teknos, C. R. Bradford, W. R. Carroll and
R. M. Esclamado, “Pectoralis Major Myocutaneous Flap
vs Revascularized Free Tissue Transfer: Complications,
Gastrostomy Tube Dependence, and Hospitalization,”
Archives of Otolaryngology—Head & Neck Surgery, Vol.
130, No. 2, 2004, pp. 181-186.
doi:10.1001/archotol.130.2.181
[10] D. Novakovic, R. S. Patel, D. P. Goldstein and P. J. Gul-
lane, “Salvage of Failed Free Flaps Used in Head and
Neck Reconstruction,” Head & Neck Oncology, Vol. 1,
2009, p. 33. doi:10.1186/1758-3284-1-33
[11] A. Talesnik, B. Markowitz, T. Calcaterra, C. Ahn and W.
Shaw, “Cost and Outcome of Osteocutaneous Free-Tissue
Transfer versus Pedicled Soft-Tissue Reconstruction for
Composite Mandibular Defects,” Plastic and Reconstruc-
tive Surgery, Vol. 97, No. 6, 1996, pp. 1167-1178.
doi:10.1097/00006534-199605000-00011
[12] H. H. El-Marakby, “The Reliability of Pectoralis Major
Myocutaneous Flap in Head and Neck Reconstruction,”
Journal of Egyptian National Cancer Institute, Vol. 18,
No. 1, 2006, pp. 41-50.
[13] J. N. McLean, G. W. Carlson and A. Losken, “The Pec-
toralis Major Myocutaneous Flap Revisited: A Reliable
Technique for Head and Neck Reconstruction,” Annals of
Plastic Surgery, Vol. 64, No. 5, 2010, pp. 570-573.
[14] D. S. Schneider, V. Wu and M. K. Wax, “Indications for
Pedicled Pectoralis Major Flap in a Free Tissue Transfer
Practice,” Head & Neck, Vol. 34, No. 8, 2012, pp. 1106-
1110. doi:10.1002/hed.21868
[15] F. R. Pinto, C. R. Malena, C. M. Vanni, A. Capelli Fde, L.
L. Matos and J. L. Kanda, “Pectoralis Major Myocutane-
ous Flaps for Head and Neck Reconstruction: Factors In-
fluencing Occurrences of Complications and the Final
Outcome,” Sao Paulo Medical Journal, Vol. 128, No. 6,
2010, pp. 336-341.
Copyright © 2012 SciRes. MPS