 Pharmacology & Pharmacy, 2012, 3, 409-416 http://dx.doi.org/10.4236/pp.2012.34055 Published Online October 2012 (http://www.SciRP.org/journal/pp) 1 Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain* Khalid A. J. Al Khaja1#, Mohammed K. Al-Haddad2, Reginald P. Sequeira1, Adel R. Al-Offi3 1Department of Pharmacology & Therapeutics, Arabian Gulf University, Manama, Bahrain; 2Department of Psychiatry, Arabian Gulf University, Manama, Bahrain; 3Psychiatric Hospital, Ministry of Health, Manama, Bahrain. Email: #khlidj@agu.edu.bh Received May 7th, 2012; revised June 13th, 2012; accepted July 12th, 2012 ABSTRACT The aim of this study is to determine the antipsychotic prescribing pattern and the prevalence of concurrent anticho- linergic prescribing in a psychiatric referral hospital. A retrospective audit of prescriptions issued for outpatients was carried out at the Psychiatric Hospital, the only facility th at provides psychiatric services for bo th inpatients and outpa- tients in the Kingdom of Bahrain. Antipsychotic monotherapy was prescribed for 89.2% patients, whereas po lytherapy with two- and thr ee-drugs in 1 0.4% and 0.4%, r espectively. A typical antipsychotics w ere prescribed more of ten (67.7%) than typical antipsychotics. Risperidone and haloperidol were the most frequently prescribed antipsychotics. Long-act- ing risperidone injection was the only depot preparation prescribed. The mean antipsychotic dose expressed as chlor- promazine equivalent (CPZeq; mg/day) was 242 (220 for monotherapy and 414 for polytherapy). The prevalence of high dose antipsychotic (mean CPZeq > 1000 mg/day) was 1.8%, prescribed at a mean CPZeq dose of 1531 (1925 for monotherapy and 1137 for polytherapy), mainly attributed to haloperidol. Anticholinergics were co-prescribed for al- most two third of patients receiving antipsychotics, particularly for those on polytherapy (monotherapy 57.3%; poly- therapy 87.5 %). Antipsychotic polytherapy, high dose and co-prescription of an oral with a depot antipsycho tic prep ara- tion were strongly associated with concurrent prescription of anticholinergics. Procyclidine and orphenadrine were the most often prescribed anticholinergics. In Bahrain, antipsychotic monotherapy is a common practice for outpatients with psychotic disorders. Some of the antipsychotic polytherapies, dosage strategies, and high prevalence of anticho- linergic use are therapeutic issues that need to be addressed to foster evidence-based pr e scribing p ra c tice. Keywords: Anticholinergics; Antipsychotics; Best Evidence; Prescribing; Psychiatry 1. Introduction Numerous studies have reported that there are wide in- ter-country [1-4] and intra-country [4-6] variations in antipsychotic prescribing pattern for patients with psy- chotic disorders. These variations include the prevalence of antipsychotic polytherapy compared to monotherapy, typical versus atypica l antipsychotics, preference for hig h- dose antipsychotics or depot antip sychotics, and anticho- linergic co-prescription. Such variations have been at- tributed to difficulty in adhering to treatment guidelines and therapeutic alogarithms in clinical practice, differ- ences in healthcare settings, availability and cost of an- tipsychotics, introduction of atypical antipsychotics with improved adverse effects profile and efficacy, and socio- cultural determinants [3,4,7-9]. Extra-pyramidal symptoms (EPS) such as acute dysto- nia, akathesia and Parkinsonism are among the most common adverse effects of antipsychotics. In clinical practice, anticholinergics are widely used to treat and prevent antipsychotic—induced EPS. Anticholinergics should be prudently prescribed because these drugs in addition to their well-known peripheral side-effects, may worsen positive symptoms, appear to partially ameliorate negative symptoms and are associated with impaired cognitive functio ning of schizo phren ic [10] an d cogn itiv e impairment in elderly patients [11]. A recent report [12] has confirmed that there is a wide variation in anticho- linergic medication prescribing across various countries; a combination of clinical, social, economic and cultural factors are the determinants of the use of these drugs suggesting that there are considerable differences be- tween treatment guidelines and clinical practice. *The abstract of this paper was presented at the 19th European Con- gress of Psychi a try, 12-15 March 2011, Vienna, Aus t ria. #Corresponding author. Copyright © 2012 SciRes. PP  Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain 410 The initial enthusiasm about the second generation of atypical antipsychotic drugs has changed into criticism and debate culminating in the controversial CATIE (Clinical Antipsychotic Trials of Intervention Effective- ness), CUtLASS (Cost Utility of the Latest Antipsycho tic Drugs in Schizophrenia Study) and EUFEST (European First-Episode Schizophrenia Trial) trials. The debate seems to be driven more by values than by data; some place an emphasis on cost, others focus on extra-pyra- midal side effects, weight gain or efficacy [13,14]. Based on PubMed database searching (up to January 2011) using MeSH terms- antipsychotic/prescribing pat- tern/Middle East, we were unable to identify any public- cation in the last 30 years that has explored the antipsy- chotic prescription p attern in patients with psychotic dis- orders in Middle Eastern countries. The present study, therefore, focused on determining the antipsychotic pre- scribing pattern and the prevalence of concurrent anti- cholinergic prescribing to outpatients in a psychiatric referral hospital . 2. Material and Methods 2.1. Setting The Kingdom of Bahrain, with a population of 1.1 mil- lion is a group of small islands located in the Arabian Gulf. A Directorate of Health Centres, has a network of 21 primary-care health centres spread across the islands and provides free health care services to both citizens and expatriates, including dispensing of essential drugs. Pa- tients requiring psychiatric consultation are referred to the Psychiatric Hospital under the Ministry of Health. There are several well-established private hospitals. This prescription-based study was carried out at the Psychiatric Hospital, the only public hospital for psychi- atric services in Bahrain. This hospital with 201 beds provides both inpa tient and outpatient services, and is the only facility for substance abuse rehabilitation in the country. Data source and collection: All p r escriptions d ispen sed gratis at Psychiatric Hospital pharmacy for outpatients during September 2007 were collected. Prescriptions were initially screened and those with antipsychotics were analyzed. The following inclusion criteria were used: 1) prescriptions comprising one or more antipsychotic(s) alone or with an anticholinergic agent; 2) prescriptions with a refill period of minimum six weeks (in order to ensure that dose-titration has been achieved and to avoid prescription duplication). Prescriptions wherein antipsy- chotics were co-prescribed with antidepressant(s) were excluded to avoid the potential influence of intrinsic an- ticholinergic activity due to antidepressant(s) on pre- scribing rate of anticholinergic medications. The fol- lowing data were collected: age and gender for each pa- tient; type, route of administration and dose of antipsy- chotics; dose and type of co-prescribed anticholinergics. 2.2. Drugs Antipsychotics included on the psychiatric hospital es- sential drug list at the time of data collection were typical antipsychotics with high potency (haloperidol, trifluop- erazine), moderate potency (zuclopenthixol), and low potency (chlorpromazine and thioridazine). Atypical an- tipsychotics included clozapine, olanzapine, risperidone and sulpiride. Parenteral preparations included decanoate formulations of haloperidol, flupenthixol, fluphenazine and zuclopenthixol, and risperidone long-acting injection (LAI). 2.3. Operational Definitions According to evidence-based criteria [15] antipsychotic- induced EPS were categorized as follows: absent or neg- ligible (0) for clozapin e; low (1+) for olanzapin e, sulpirid e and thioridazine; moderate (2+) for chlorpromazine and risperidone; moderately severe (3+) for trifluoperazine and zuclopenthixol; and severe (4+) for haloperidol. Con- version of oral antipsychotic dose to chlorpromazine equivalent (CPZeq) dose was derived from evidence- based published data [1,15-17]. Antipsychotic polyther- apy (combination antipsychotic therapy) is defined as concomitant use of >2 antipsychotics (either typical/ atypical/combination of both). High-dose antipsychotics are defined as mean CPZeq doses > 1000 mg/day [18]. As per Diagnostic and Statistical Manual (DSM)-IV cri- teria, psychotic disorders include schizophrenias, schizo- affective and schizoform disorders. In this report, antip- sychotics, particularly atypical, may also be used as off- label medications for dementia, major depression disor- ders, autism spectrum disorders, obsessive compulsive disorders, combat-related post traumatic stress disorders and generalized anxiety disorders. 2.4. Statistical Analysis Data were analyzed using Statistical Package for the So- cial Sciences (SPSS/PC+, version 15). Chi-square (x2) and Fisher’s exact tests, as appropriate, were used to test differences between proportions, and two-tailed t-test was used for continuous variables. A p-value of <0.05 was considered statistically significant. 3. Results Out of 1591 prescription s, 454 (2 8.5%) met th e inclus ion criteria. However, 1137 outpatient prescriptions (71.4%) were excluded because: 912 (57.3%) were on antide- pressant(s) and 225 (14.1%) were on antipsychotic co-prescribed with antidepressant(s). The mean age (±SD) Copyright © 2012 SciRes. PP 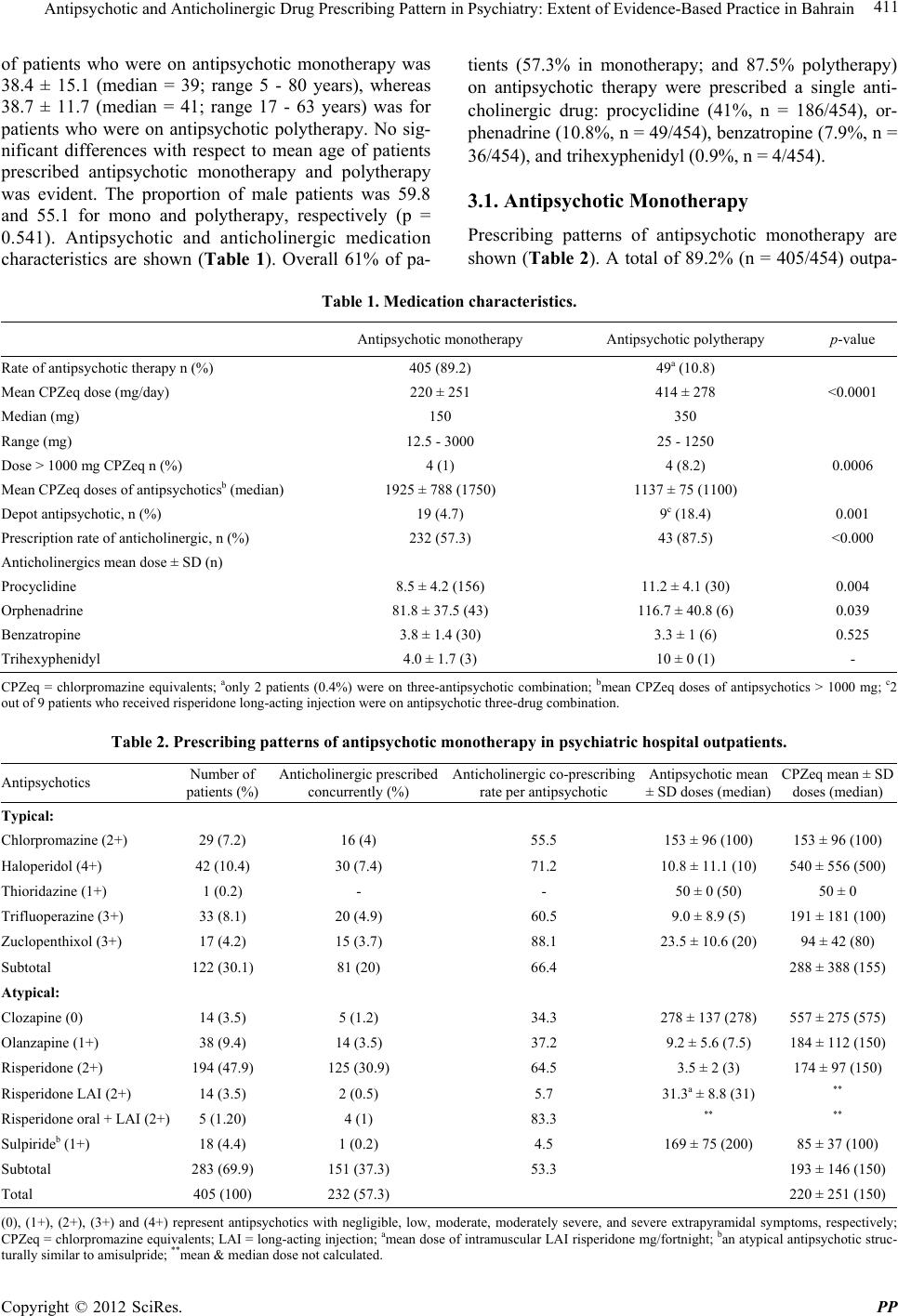 Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain Copyright © 2012 SciRes. PP 411 of patients who were on antipsychotic monotherapy was 38.4 ± 15.1 (median = 39; range 5 - 80 years), whereas 38.7 ± 11.7 (median = 41; range 17 - 63 years) was for patients who were on antipsychotic polytherapy. No sig- nificant differences with respect to mean age of patients prescribed antipsychotic monotherapy and polytherapy was evident. The proportion of male patients was 59.8 and 55.1 for mono and polytherapy, respectively (p = 0.541). Antipsychotic and anticholinergic medication characteristics are shown (Table 1). Overall 61% of pa- tients (57.3% in monotherapy; and 87.5% polytherapy) on antipsychotic therapy were prescribed a single anti- cholinergic drug: procyclidine (41%, n = 186/454), or- phenadrine (10.8%, n = 49/454), benzatropine (7.9%, n = 36/454), and trihexyphenidyl (0.9%, n = 4/454). 3.1. Antipsychotic Monotherapy Prescribing patterns of antipsychotic monotherapy are shown (Table 2). A total of 89.2% (n = 405/454) outpa- Table 1. Medication characteristics. Antipsychotic monotherapy Antipsychotic polytherapy p-value Rate of antipsychotic therapy n (%) 405 (89.2) 49a (10.8) Mean CPZeq dose (mg/day) 220 ± 251 414 ± 278 <0.0001 Median (mg) 150 350 Range (mg) 12.5 - 3000 25 - 1250 Dose > 1000 mg CPZeq n (%) 4 (1) 4 (8.2) 0.0006 Mean CPZeq doses of antipsychoticsb (median) 1925 ± 788 (1750) 1137 ± 75 (1100) Depot antipsychotic, n (%) 19 (4.7) 9c (18.4) 0.001 Prescription rate of anticholinergic, n (%) 232 (57.3) 43 (87.5) <0.000 Anticholinergics mean dose ± SD (n) Procyclidine 8.5 ± 4.2 (156) 11.2 ± 4.1 (30) 0.004 Orphenadrine 81.8 ± 37.5 (43) 116.7 ± 40.8 (6) 0.039 Benzatropine 3.8 ± 1.4 (30) 3.3 ± 1 (6) 0.525 Trihexyphenidyl 4.0 ± 1.7 (3) 10 ± 0 (1) - CPZeq = chlorpromazine equivalents; aonly 2 patients (0.4%) were on three-antipsychotic combination; bmean CPZeq doses of antipsychotics > 1000 mg; c2 out of 9 patients who received risperidone long-acting injection were on antipsychotic three-drug combination. Table 2. Prescribing patterns of antipsychotic monotherapy in psychiatric hospital outpatients. Antipsychotics Number of patients (%) Anticholinergic prescribed concurrently (%) Anticholinergic co-prescribing rate per antipsychotic Antipsychotic mean ± SD doses (median) CPZeq mean ±SD doses (median) Typical: Chlorpromazine (2+) 29 (7.2) 16 (4) 55.5 153 ± 96 (100) 153 ± 96 (1 00) Haloperidol (4+) 42 (10.4) 30 (7.4) 71.2 10.8 ± 11.1 (10) 540 ± 556 (500) Thioridazine (1+) 1 (0.2) - - 50 ± 0 (50) 50 ± 0 Trifluoperazine (3+) 33 (8.1) 20 (4.9) 60. 5 9.0 ± 8 .9 (5) 191 ± 181 (100) Zuclopenthixol (3+ ) 17 (4.2) 15 (3.7) 88.1 23.5 ± 10.6 (20) 94 ± 42 (80) Subtotal 122 (30.1) 81 (20) 66.4 288 ± 388 (155) Atypical: Clozapine (0) 14 (3.5) 5 (1.2) 34.3 278 ± 137 (278) 557 ± 275 (575) Olanzapine (1+) 38 (9.4) 14 (3.5) 37.2 9.2 ± 5.6 (7.5) 184 ± 112 (150) Risperidone (2+) 194 (47.9) 125 (30.9) 64.5 3.5 ± 2 (3) 174 ± 97 (150) Risperidone LAI (2+) 14 (3.5) 2 (0.5) 5.7 31.3a ± 8.8 (31) ** Risperidone oral + LAI (2+) 5 (1.20) 4 (1) 83.3 ** ** Sulpirideb (1+) 18 (4.4) 1 (0.2) 4.5 169 ± 75 (200) 85 ± 37 (100) Subtotal 283 (69.9) 151 (37.3) 53.3 193 ± 146 (150) Total 405 (100) 232 (57.3) 220 ± 251 (150) (0), (1+), (2+), (3+) and (4+) represent antipsychotics with negligible, low, moderate, moderately severe, and severe extrapyramidal symptoms, respectively; CPZeq = chlorpromazine equivalents; LAI = long-acting injection; amean dose of intramuscular LAI risperidone mg/fortnight; ban atypical antipsychotic struc- turally similar to amisulpride; **mean & median dose not calculated. 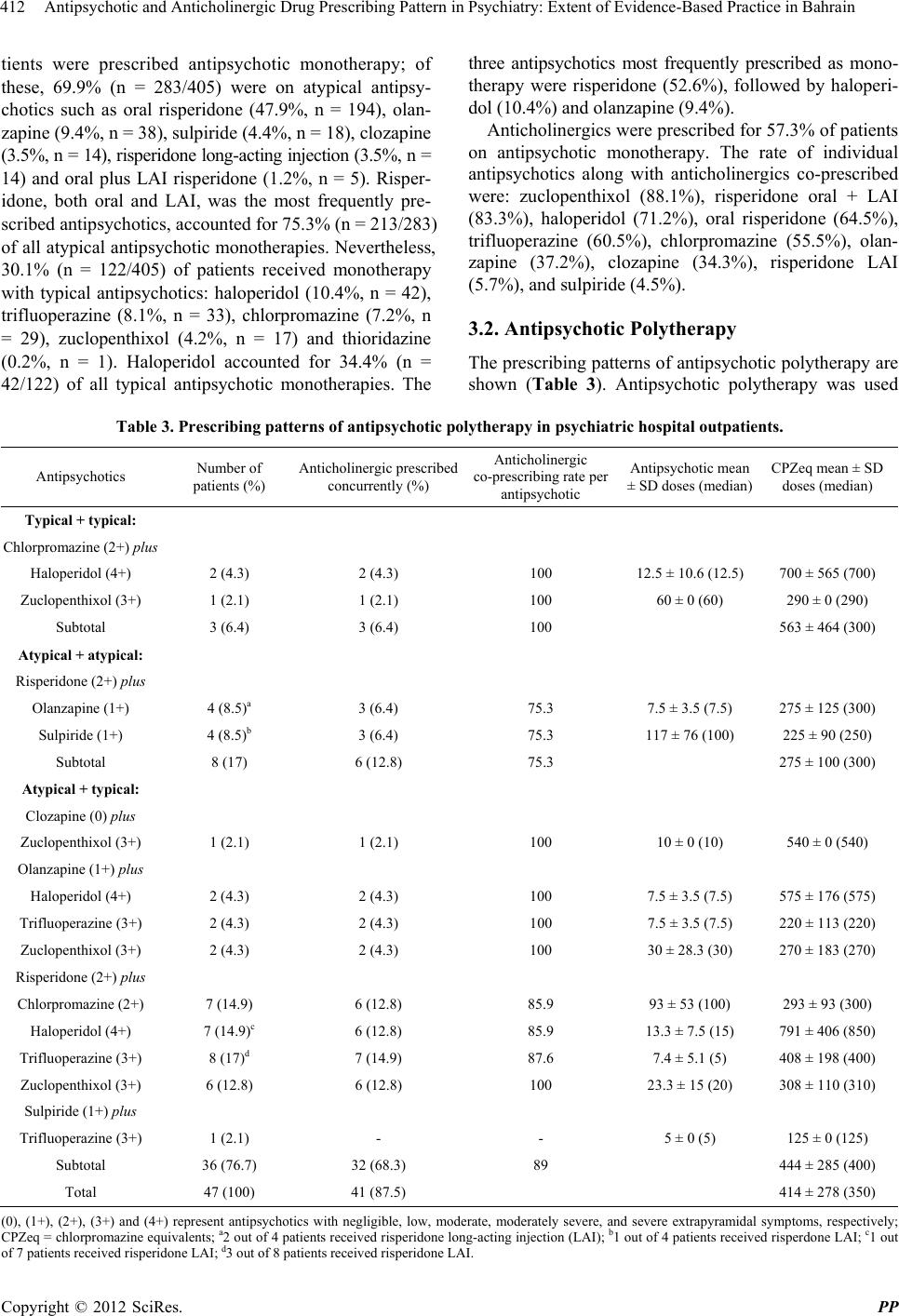 Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain 412 tients were prescribed antipsychotic monotherapy; of these, 69.9% (n = 283/405) were on atypical antipsy- chotics such as oral risperidone (47.9%, n = 194), olan- zapine (9.4%, n = 38), sulpiride (4.4%, n = 18), clozapine (3.5%, n = 14), risp eridone long-acting injection (3.5 %, n = 14) and oral plus LAI risperidone (1.2%, n = 5). Risper- idone, both oral and LAI, was the most frequently pre- scribed antipsychotics, accounted for 75.3% (n = 213/283) of all atypical antipsychotic monotherapies. Nevertheless, 30.1% (n = 122/405) of patients received monotherapy with typical antipsychotics: haloperidol (10.4%, n = 42), trifluoperazine (8.1%, n = 33), chlorpromazine (7.2%, n = 29), zuclopenthixol (4.2%, n = 17) and thioridazine (0.2%, n = 1). Haloperidol accounted for 34.4% (n = 42/122) of all typical antipsychotic monotherapies. The three antipsychotics most frequently prescribed as mono- therapy were risperidone (52.6%), followed by haloperi- dol (10.4%) a n d ol anzapine (9.4%) . Anticholinergics were prescribed for 57 .3% of patien ts on antipsychotic monotherapy. The rate of individual antipsychotics along with anticholinergics co-prescribed were: zuclopenthixol (88.1%), risperidone oral + LAI (83.3%), haloperidol (71.2%), oral risperidone (64.5%), trifluoperazine (60.5%), chlorpromazine (55.5%), olan- zapine (37.2%), clozapine (34.3%), risperidone LAI (5.7%), and sulpiride (4.5%). 3.2. Antipsychotic Polytherapy The prescribing pattern s of antipsycho tic polytherapy are shown (Table 3). Antipsychotic polytherapy was used Table 3. Prescribing patterns of antipsychotic polytherapy in psychiatric hospital outpatients. Antipsychotics Number of patients (%) Anticholinergic prescribed concurrently (%) Anticholinergic co-prescribing rate per antipsychotic Antipsychotic mean ± SD doses (median) CPZeq mean ± SD doses (median) Typical + typical: Chlorpromazine (2+) plus Haloperidol (4+) 2 (4.3) 2 (4.3) 100 12.5 ± 10.6 (12.5) 700 ± 565 (700) Zuclopenthixol (3+) 1 (2.1) 1 (2.1) 100 60 ± 0 (60) 290 ± 0 (290) Subtotal 3 (6.4) 3 (6.4) 100 563 ± 464 (300) Atypical + atypical: Risperidone (2+) plus Olanzapine (1+) 4 (8.5)a 3 (6.4) 75.3 7.5 ± 3.5 (7.5) 275 ± 125 (300) Sulpiride (1+) 4 (8.5)b 3 (6.4) 75.3 117 ± 76 (100) 225 ± 90 (250) Subtotal 8 (17) 6 (12.8) 75.3 275 ± 100 (300) Atypical + typical: Clozapine (0) plus Zuclopenthixol (3+) 1 (2.1) 1 (2.1) 100 10 ± 0 (10) 540 ± 0 (540) Olanzapine (1+) plus Haloperidol (4+) 2 (4.3) 2 (4.3) 100 7.5 ± 3.5 (7.5) 575 ± 176 (575) Trifluoperazine (3+) 2 (4.3) 2 (4.3) 100 7.5 ± 3.5 (7.5) 220 ± 113 (220) Zuclopenthixol (3+ ) 2 (4.3) 2 (4.3) 100 30 ± 28.3 (30) 270 ± 183 (270) Risperidone (2+) plus Chlorproma zi ne (2+) 7 (14.9) 6 (12.8) 85.9 93 ± 53 (10 0) 293 ± 93 (300) Haloperidol (4+) 7 (14.9)c 6 (12.8) 85.9 13.3 ± 7.5 (15) 791 ± 406 (850) Trifluoperazine (3+) 8 (17)d 7 (14.9) 87.6 7.4 ± 5.1 (5) 408 ± 198 (400) Zuclopenthixol (3+) 6 (12.8) 6 (12.8) 100 23.3 ± 15 (20) 308 ± 110 (310) Sulpiride (1+) plus Trifluoperazi ne (3+) 1 (2.1) - - 5 ± 0 (5) 125 ± 0 (125) Subtotal 36 (76.7) 32 (68.3) 89 444 ± 285 (400) Total 47 (100) 41 (87.5) 414 ± 278 (350) (0), (1+), (2+), (3+) and (4+) represent antipsychotics with negligible, low, moderate, moderately severe, and severe extrapyramidal symptoms, respectively; CPZeq = chlorpromazine equivalents; a2 out of 4 p atients r eceived r isper idone l ong-acti ng inj ection ( LAI); b1 ou t of 4 p atient s received risp erdone LAI ; c1 out of 7 patients received risperidone LAI; d3 out of 8 patients received risperidone LAI. Copyright © 2012 SciRes. PP  Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain 413 for 10.8% (n = 49/454) outpatients; of these 10.4% (n = 47/454) were on two antipsychotics, whereas 0.4% (n = 2/454) were on three antipsychotics. Pattern of antipsy- chotic two-drug therapy in descending order was as fol- lows: an atypical with a typ ical antip sycho tic (76.6 %, n = 36/47), two atypical antipsychotics (17%, n = 8/47), and two typical antipsychotics (6 .4 %, n = 3/47 ; Table 3). The antipsychotic two-drug combinations prescribed most often were risperidone/trifluoperazine (17%), followed by risperidone with either chlorpromazine (14.9%) or halop- eridol (14.9%) or zuclopenthixol (12.8%). The three an- tipsychotics most commonly prescribed as polytherapy were risperidone (73.5%), followed by haloperidol (22.4 % ) and trifluoperazine (22.4%). Anticholinergics were prescribed for 87 .5% of patien ts on antipsychotic polytherapy (two antipsychotic combi- nation); a typical antipsychotic co-prescribed with an- other typical or with an atypical antipsychotic had a greater likelihood of being prescribed with anticholiner- gic medications (Table 3). Antipsychotic three-drug combination comprising chlor- promazine plus zuclopenthixol plus risperidone LAI was prescribed for 0.4% (n = 2/454) outpatients (Data not shown). 4. Discussion Antipsychotics: This study provides insights, based on audit of prescriptions, into the prescribing patterns of antipsychotic and anticholinergic medications for outpa- tients with psychotic disorders receiving treatment at a public referral hospital in Bahrain. The data suggest that atypical antipsychotic monotherapy is the most preferred treatment. Antipsychotic monotherapy was prescribed for most of the patients (89.2%), a rate which is comparable to 86.5% reported in New Zealand [5], 87% in Australia [19], 87% - 91% in USA [20,21] and 82.6% in UK [22], consistent with clinical guidelines [8,16]. With the ex- ception of haloperidol and clozapine (Table 2), the indi- vidual antipsychotic daily dose for other monotherapies was generally lower than the recommended therapeutic range [8,18], deemed to be inadequate for many with psychosi s [ 8,18,23]. Despite the superior clinical effectiveness, EPS safety profile [24], and as being the preferred drug for patients with schizophrenia who are unresponsive to adequate multiple antipsychotic monotherapy trials [8,18], clozap- ine is significantly under-prescribed and accounted for only 3.3% of overall antipsychotics (Tables 2 and 3). In contrast, other studies reported clozapine to be the most commonly prescribed antipsychotic medication in up to 25% - 60% of schizophrenic inpatients in China [25] and in 34.5% of outpatients in New Zealand [2 6]. In general, limited clinical utility of clozapine appears to be due to propensity to cause agranulocytosis and the need for mandatory hematological monitoring of patients [27]. Psychiatrists, therefore, may find it appealing to pre- scribe antipsychotic polytherapy rather than to prescribe clozapine [21]. Moreover, clozapine was included in the drug list only few months prior to data collection and prescribing was restricted to consultants in psychiatric hospital in Bahrain at that time. The combination antipsychotic therapy in our study was rarely used (10.8%), and conforms with expert guid e- lines [8]. A low trend towards polytherapy may be re- lated to the nature of study population in our study, i.e., outpatients. Of note, symptoms of psychotic disorders in outpatients perhaps are less severe and persistent than those of inpatients. Thus outpatients may less often be prescribed with antipsychotic polytherapy than inpatients [21]. In our study, concomitant antipsychotic therapy (a typical with an atypical) comprised 76.6% of overall an- tipsychotic polytherapy (Table 3) which is in line with rates reported elsewhere [5,21]. Moreover, polytherapy in our survey may have resulted from adding a typical to an atypical (top up strategy) to improve persistent posi- tive symptoms [21,28], or adding an atypical to a typical to switch to the atypical regimen [21] or cross-tapering designed to chan ge antipsychotic regimen (cross-titration trap) [2,21,28]. A prospective study combining quantita- tive and qualitative approaches can address the primary reason for the use of anti psychotic po lytherapy. The overall prevalence of high-dose antipsychotics was 1.8%, prescribed at a mean daily CPZeq dose of 1531 ± 668 mg (median = 1225, data not shown). High- dose antipsychotic practice was found to be more likely related to antipsychotic polytherapy (8.2% [polytherapy] vs. 1% [monotherapy]; p = 0.0006, Table 1); it is mainly attributed to the high dose of haloperidol prescribed as both monotherap y an d co mbinatio n an tip sycho tic th erap y. The rate of high-dose antipsychotic was equivalent to that reported recently for psychiatric outpatients in Hong Kong (1.8%) [29]. Moreover, we found that the rate of high-dose antipsychotic monotherapy (1%) was less than the 2.5% reported for outpatients in USA [22]. Anticholinergics: Notwithstanding considerable dif- ferences between anticholinergics, these medications are the mainstay for treatment of EPS-induced by antipsy- chotics. EPS occur mostly with typical antipsychotics, particularly those with high potency, and occasionally with atypical antipsychotics. We found that anticholiner- gic drugs were co-prescribed extensively along with both typical and atypical antipsychotics. The prevalence of anticholinergic use was 57.3% and 87.5% for outpatients on antipsychotic monotherapy and polytherapy, respec- tively. These rates were significantly greater than those reported for outpatients elsewhere [2,5,9,30] (regardless of type and therapy of antipsychotics studied) which suggests the possibility that cultural and institutiona l pra- Copyright © 2012 SciRes. PP  Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain 414 ctices would have contributed to these findings. In our study anticholinergics may have been routinely pre- scribed even in the absence of EPS, although exp erts dis- agree about the prophylactic use of these agents [16,18]. This therapeutic dilemma ha s been addressed by Gjerden et al. [31] who viewed that anticholinergic use appears to be superfluous for at least one-third of patients, and their use exceeded the incidence of EPS [32]. Our study has identified that antipsychotic polyth erapy is a key predictor for the use of anticholinergics since both proportion and mean dose of co-prescribed anticho- linergic (specifically for most often prescribed procycli- dine and orphenadrine) increase proportionally with the increase in number of prescribed antipsychotic medica- tions (Table 1). Anticholinergics should be prudently prescribed because these drugs, in addition to their pe- ripheral side effects, can impair cognition, especially in the elderly patients [11]. Anticholinergics may worsen positive symptoms, appear to partially ameliorate nega- tive symptoms, and are associated with impaired cogni- tive functioning of schizophrenic patients [10]. Prescrib- ers should be aware of the potential anticholinergic—re- lated peripheral side effects, particularly, when anti-cho- linergic medications are prescribed with antipsychotics that have greater intrinsic anticholinergic activity, such as the phenothiazines. We also found that high anticholinergic drug preva- lence is less likely to b e associated with the mean CPZeq doses, particularly atypical antipsychotics (Table 2). These findings suggest that overt anticholinergic prescrib- ing may arguably be superfluous for several reasons. Fir s t, clozapine and olanzapine have significant intrinsic anti- cholinergic activity, which may be partly responsible for fewer EPS and obviates the need for an anticholinergic agents [33]. Approximately 35% of patients who received these medications were prescribed anticholinergic medi- cations (Table 2), perhaps to mitigate clozapine-induced hypersalivation [34]. Second, dose-dependent EPS have been reported to appear in 60% to 70% of patients taking risperidone at dosages of >6 mg/day (i.e., >300 mg/day CPZeq) [35-37]. Nonetheless, approximately 65% of patients on risperidone monotherapy (who received a mean dose of 3.5 mg/day, i.e., 175 mg/day CPZeq) were prescribed anticholinergic drugs (Table 2). Third, most guidelines converge on a recommendation that doses of antipsychotics should range between 300 and 1000 mg CPZeq in order to achieve effective control of positive symptoms [8,18] while avoiding EPS and the use of an- ticholinergic drugs [38]. In contrast to this, the mean CPZeq doses especially as monotherapy (Table 2), the most sought practice in our cohort, was significantly be- low this range [8,18,23]. Fourth, atypical antipsychotics as a class, generally produce fewer or no EPS relative to typical antipsychotics, which can produce clinically sig- nificant EPS in 60% of patients [33]. Moreover, risper- idone is considered the most likely atypical antipsychotic agent to produce EPS [15]. It is, therefore, the high pre- valence of anticho lin ergic co-p rescrip tion in patien ts who received atypical antipsychotic monotherapy (53.3%; Ta- ble 2) can be attributed, in addition to the suggested su- perfluous prescribing trend, to the frequent use of this agent in this group. Sulpiride was rarely prescribed with anticholinergic medications (4.5%, Table 2). This may be attributed to: 1) its classification as an atypical benzamide antipsychotic associated with low incidence of EPS; and 2) its pre- scription in low dose (85 mg CPZeq), a dose which is significantly lower than the recommended antipsychotic therapeutic range (400 - 1200 mg) required for control- ling both negative and positive symptoms of schizophre- nia [16]. In our study, different aspects related to prescription patterns of antipsychotics and the concurrent prescript- tions of anticholin ergics app ear either to be at variance or in agreement with a large body of literature worldwide. These inter-country variations may be due to several de- terminants such as healthcare setting, availability and cost of antipsychotics, population sample (outpatients versus inpatients), treatment settings (psychiatric ho spital versus psychiatric unit in a general hospital or emergency setting versus nonemergency setting), standard treatment guidelines, psychiatrists’ training background and socio- cultural context of clinical presentations [1,39]. We sug- gest that the cultural or institutionally biased approach may play a determinant role in prescribing patterns of these drugs. Moreover, inter-racial differences in effect- tive therapeutic dosage of antipsychotics in treating psy- chotic symptoms and variations in psychotic symptoms response to antipsychotic therapy should also be consid- ered [39,40]. 4.1. Limitations of the Study Several limitations need to be considered while inter- preting the findings of this study. Since the diagnosis of psychotic disorder is not stated in prescriptions, the therapeutic rationale for antipsychotics prescribed is un- certain. Moreover, factors that would influence the an- tipsychotic selection such as history of previous treat- ment response, drug safety in overdose, overall adverse effect profile, comorbid condition, non-psychotic medi- cations used, and patient preference, if any, are uncertain. Therefore the observations of this study need to be inter- preted with caution. 4.2. Conclusion In Bahrain, antipsychotic monotherapy is the common practice for outpatients with psychotic disorders. Some Copyright © 2012 SciRes. PP 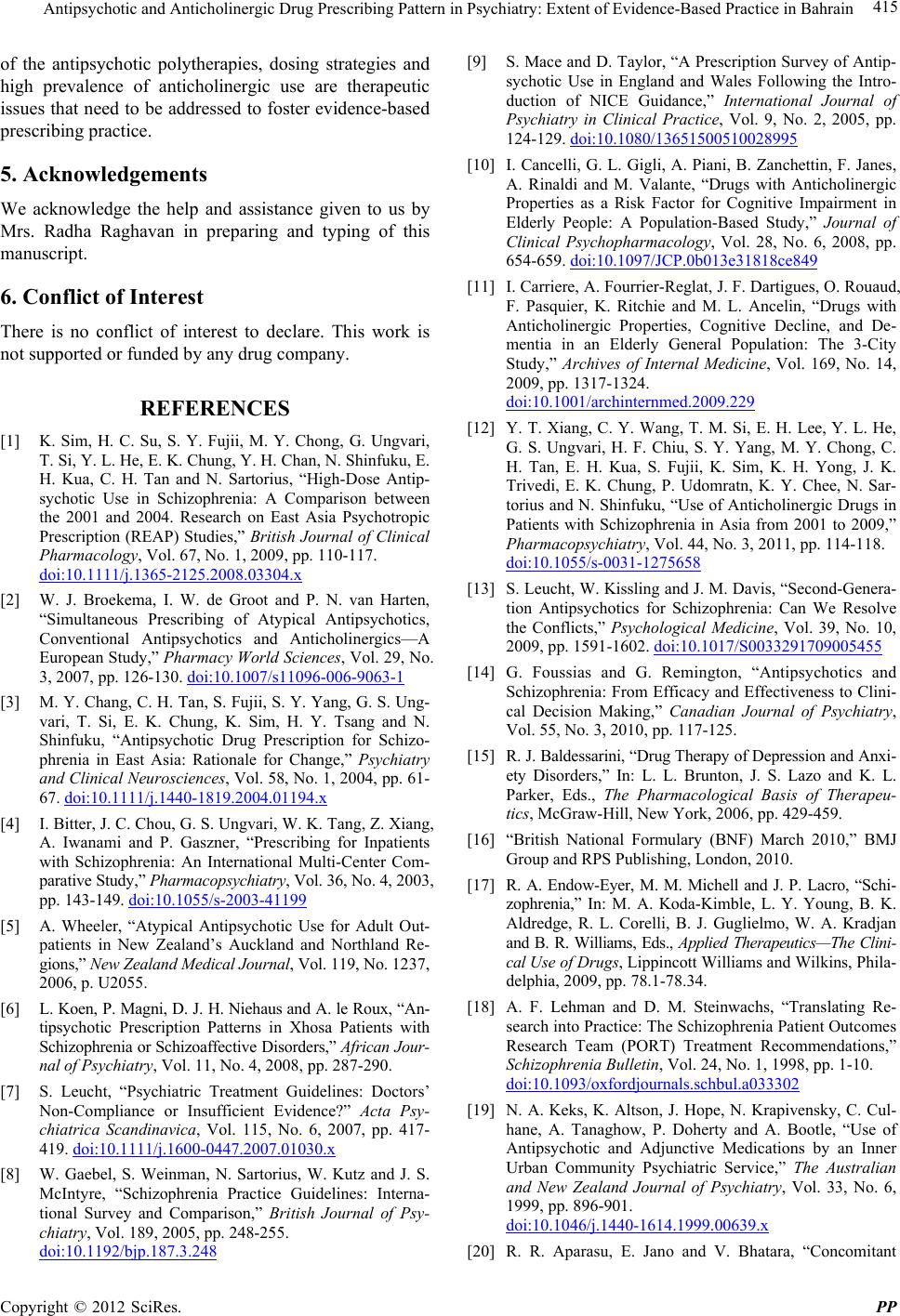 Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain 415 of the antipsychotic polytherapies, dosing strategies and high prevalence of anticholinergic use are therapeutic issues that need to be addressed to foster evidence-based prescribing practice. 5. Acknowledgements We acknowledge the help and assistance given to us by Mrs. Radha Raghavan in preparing and typing of this manuscript. 6. Conflict of Interest There is no conflict of interest to declare. This work is not supported or funded by any drug co mpany. REFERENCES [1] K. Sim, H. C. Su, S. Y. Fujii, M. Y. Chong, G. Ungvari, T. Si, Y. L. He, E. K. Chung, Y. H. Chan, N. Shinfuku, E. H. Kua, C. H. Tan and N. Sartorius, “High-Dose Antip- sychotic Use in Schizophrenia: A Comparison between the 2001 and 2004. Research on East Asia Psychotropic Prescription (REAP) Studies,” British Journal of Clinical Pharmacology, Vol. 67, No. 1, 2009, pp. 110-117. doi:10.1111/j.1365-2125.2008.03304.x [2] W. J. Broekema, I. W. de Groot and P. N. van Harten, “Simultaneous Prescribing of Atypical Antipsychotics, Conventional Antipsychotics and Anticholinergics—A European Study,” Pharmacy World Sciences, Vol. 29, No. 3, 2007, pp. 126-130. doi:10.1007/s11096-006-9063-1 [3] M. Y. Chang, C. H. Tan, S. Fujii, S. Y. Yang, G. S. Ung- vari, T. Si, E. K. Chung, K. Sim, H. Y. Tsang and N. Shinfuku, “Antipsychotic Drug Prescription for Schizo- phrenia in East Asia: Rationale for Change,” Psychiatry and Clinical Neurosciences, Vol. 58, No. 1, 2004, pp. 61- 67. doi:10.1111/j.1440-1819.2004.01194.x [4] I. Bitter, J. C. Chou, G. S. Ungvari, W. K. Tang, Z. Xiang, A. Iwanami and P. Gaszner, “Prescribing for Inpatients with Schizophrenia: An International Multi-Center Com- parative Study,” Pharmacopsychiatry, Vol. 36, No. 4, 2003, pp. 143-149. doi:10.1055/s-2003-41199 [5] A. Wheeler, “Atypical Antipsychotic Use for Adult Out- patients in New Zealand’s Auckland and Northland Re- gions,” New Zealand Medical Journal, Vol. 119, No. 1237, 2006, p. U2055. [6] L. Koen, P. Mag ni, D. J. H. Nie haus and A. le R oux, “An- tipsychotic Prescription Patterns in Xhosa Patients with Schizophrenia or Schizoaffective Disorders,” African Jour- na l of Psychiatr y , Vol. 11, No. 4, 2008, pp. 287-290. [7] S. Leucht, “Psychiatric Treatment Guidelines: Doctors’ Non-Compliance or Insufficient Evidence?” Acta Psy- chiatrica Scandinavica, Vol. 115, No. 6, 2007, pp. 417- 419. doi:10.1111/j.1600-0447.2007.01030.x [8] W. Gaebel, S. Weinman, N. Sartorius, W. Kutz and J. S. McIntyre, “Schizophrenia Practice Guidelines: Interna- tional Survey and Comparison,” British Journal of Psy- chiatry, Vol. 189, 2005, pp. 248-255. doi:10.1192/bjp.187.3.248 [9] S. Mace and D. Taylor, “A Prescription Survey of Antip- sychotic Use in England and Wales Following the Intro- duction of NICE Guidance,” International Journal of Psychiatry in Clinical Practice, Vol. 9, No. 2, 2005, pp. 124-129. doi:10.1080/13651500510028995 [10] I. Cancelli, G. L. Gigli, A. Piani, B. Zanchettin, F. Janes, A. Rinaldi and M. Valante, “Drugs with Anticholinergic Properties as a Risk Factor for Cognitive Impairment in Elderly People: A Population-Based Study,” Journal of Clinical Psychopharmacology, Vol. 28, No. 6, 2008, pp. 654-659. doi:10.1097/JCP.0b013e31818ce849 [11] I. Carriere, A. Fourrier-Reglat, J. F. Dartigues, O. Rouaud, F. Pasquier, K. Ritchie and M. L. Ancelin, “Drugs with Anticholinergic Properties, Cognitive Decline, and De- mentia in an Elderly General Population: The 3-City Study,” Archives of Internal Medicine, Vol. 169, No. 14, 2009, pp. 1317-1324. doi:10.1001/archinternmed.2009.229 [12] Y. T. Xiang, C. Y. Wang, T. M. Si, E. H. Lee, Y. L. He, G. S. Ungvari, H. F. Chiu, S. Y. Yang, M. Y. Chong, C. H. Tan, E. H. Kua, S. Fujii, K. Sim, K. H. Yong, J. K. Trivedi, E. K. Chung, P. Udomratn, K. Y. Chee, N. Sar- torius and N. Shinfuku, “Use of Anticholinergic Drugs in Patients with Schizophrenia in Asia from 2001 to 2009,” Pharmacopsychiatry, Vol. 44, No. 3, 2011, pp. 114-118. doi:10.1055/s-0031-1275658 [13] S. Leucht, W. Kissling and J. M. Davis, “Second-Genera- tion Antipsychotics for Schizophrenia: Can We Resolve the Conflicts,” Psychological Medicine, Vol. 39, No. 10, 2009, pp. 1591-1602. doi:10.1017/S0033291709005455 [14] G. Foussias and G. Remington, “Antipsychotics and Schizophrenia: From Efficacy and Effectiveness to Clini- cal Decision Making,” Canadian Journal of Psychiatry, Vol. 55, No. 3, 2010, pp. 117-125. [15] R. J. Baldessarini, “Drug Therapy of Dep ression and Anxi- ety Disorders,” In: L. L. Brunton, J. S. Lazo and K. L. Parker, Eds., The Pharmacological Basis of Therapeu- tics, McGraw-Hill, New York, 2006, pp. 429-459. [16] “British National Formulary (BNF) March 2010,” BMJ Group and RPS Publishing, London, 2010. [17] R. A. Endow-Eyer, M. M. Michell and J. P. Lacro, “Schi- zophrenia,” In: M. A. Koda-Kimble, L. Y. Young, B. K. Aldredge, R. L. Corelli, B. J. Guglielmo, W. A. Kradjan and B. R. Williams, Eds., Applied Therapeutics—The Clini- cal Use of Drugs, Lippincott Williams and Wilkins, Phila- delphia, 2009, pp. 78.1-78.34. [18] A. F. Lehman and D. M. Steinwachs, “Translating Re- search into Practice: The Schizophrenia Patient Outcomes Research Team (PORT) Treatment Recommendations,” Schizophrenia Bulletin, Vol. 24, No. 1, 1998, pp. 1-10. doi:10.1093/oxfordjournals.schbul.a033302 [19] N. A. Keks, K. Altson, J. Hope, N. Krapivensky, C. Cul- hane, A. Tanaghow, P. Doherty and A. Bootle, “Use of Antipsychotic and Adjunctive Medications by an Inner Urban Community Psychiatric Service,” The Australian and New Zealand Journal of Psychiatry, Vol. 33, No. 6, 1999, pp. 896-901. doi:10.1046/j.1440-1614.1999.00639.x [20] R. R. Aparasu, E. Jano and V. Bhatara, “Concomitant Copyright © 2012 SciRes. PP  Antipsychotic and Anticholinergic Drug Prescribing Pattern in Psychiatry: Extent of Evidence-Based Practice in Bahrain Copyright © 2012 SciRes. PP 416 Antipsychotic Prescription in US Outpatient Settings,” Research in Social and Administrative Pharmacy, Vol. 5, No. 3, 2009, pp. 234-241. doi:10.1016/j.sapharm.2008.08.005 [21] A. Tapp, A. E. Wood, L. Secrest, J. Erdmann, L. Cubber- ley and N. Kilzieh, “Combination Antipsychotic Therapy in Clinical Practice,” Psychiatric Services, Vol. 54, No. 4, 2003, pp. 55-59. doi:10.1176/appi.ps.54.4.574-a [22] N. Ranceva, W. Ashraf and D. Odelola, “Antipsychotic Polypharmacy in Outpatients at Birch Hill Hospital: In- cidence and Adherence to Guidelines,” Journal of Clini- cal Pharmacology, Vol. 50, No. 6, 2010, pp. 699-704. doi:10.1177/0091270009350625 [23] R. J. Baldessarini, B. M. Cohen and M. H. Teic her, “Sig- nificance of Neuroleptic Dose and Plasma Level in Phar- macological Treatment of Psychoses,” Archives of Gen- eral Psychiatry, Vol. 45, No. 1, 1988, pp. 79-90. doi:10.1001/archpsyc.1988.01800250095013 [24] A. Essali, N. Al-Haj Hassan, C. Li and J. Rathbone, “Clo- zapine versus Typical Neuroleptic Medication for Schi- zophrenia,” Cochrane Database System Review, Vol. 21, No. 1, 2009, CD 000059. [25] Y. L. Tang, P. X. Mao, F. Jiang, Q. Chen, C. Y. Wang, Z. J. Cai and P. B. Michell, “Clozapine in China,” Pharma- copsychiatry, Vol. 41, No. 1, 2008, pp. 1-9. doi:10.1055/s-2007-993224 [26] A. Wheeler, V. Humberstone, E. Robinson, J. Sheridan and P. Joyce, “Impact of Audit and Feed-Back on Antip- sychotic Prescription in Schizophrenia,” Journal of Ev alua- tion in Clinical Practice, Vol. 15, No. 3, 2009, pp. 441- 450. doi:10.1111/j.1365-2753.2008.01032.x [27] S. Miyamoto, G. E. Duncan, C. E. Marx and J. A. Lie- berman, “Treatments for Schizophrenia: A Critical Re- view of Pharmacology and Mechanisms of Action of An- tipsychotic Drugs,” Molecular Psychiatry, Vol. 10, No. 1, 2005, pp. 79-104. doi:10.1038/sj.mp.4001556 [28] S. M. Stahl, “Antipsychotic Polypharmacy. Part 1: Thera- peutic Option or Dirty Little Secret?” Journal of Clinical Psychiatry, Vol. 60, No. 7, 1999, pp. 425-426. doi:10.4088/JCP.v60n0701 [29] G. B. Hung and H. K. Cheung, “Predictors of High-Dose Antipsychotic Prescription in Psychiatric Patients in Hong Kong,” Hong Kong Medical Jou rnal, Vol. 14, No. 1, 2008, pp. 35-39. [30] Y. T. Xiang, Y. Z. Weng, C. M. Leung, W. K. Tang and U. G. Sandor, “Exploring the Clinical and Social Deter- minants of Prescribing Anticholinergic Medication for Chinese Patients with Schizophrenia,” Human Psychophar- macology, Vol. 22, No. 3, 2007, pp. 173-180. doi:10.1002/hup.830 [31] P. Gjerden, L. Slordal and J. G. Bramness, “The Use of Antipsychotic and Anticholinergic Antiparkinson Drugs in Norway after the Withdrawal of Orphenadrine,” British Journal of Clinical Pharmacology, Vol. 68, No. 2, 2009, pp. 238-242. doi:10.1111/j.1365-2125.2009.03446.x [32] I. S. Hong and J. R. Bishop, “Anticholinergic Use in Children and Adolescence after Initiation of Antipsy- chotic Therapy,” Annals of Pharmacotherapy, Vol. 44, No. 7, 2010, pp. 1171-1180. doi:10.1345/aph.1M643 [33] American Psychiatric Association, “American Psychiatric Association Practice Guidelines for the Treatment of Psy- chiatric Disorders, Compendium 2006,” American Psy- chiatric Publishing Inc., Arlington, 2006. [34] A. J. Wheeler, “Treatment Pathway and Patterns of Cloza- pine Prescribing for Schizophrenia in New Zealand,” An- nals of Pharmacotherapy, Vol. 42, No. 6, 2008, pp. 852- 860. doi:10.1345/aph.1K662 [35] P. Seeman, “Atypical Antipsychotics: Mechanism of Ac- tion,” Canadian Journal of Psychiatry, Vol. 47, No. 1, 2002, pp. 27-38. [36] S. Leucht, G. Pitschell-Walz, D. Abraham and W. Kissling, “Efficacy and Extrapyramidal Side-Effects of the New Antipsychotic Olanzapine, Quetiapine, Risperidone, and Sertindole Compared to Conventional Antipsychotics and Placebo: A Meta-Analysis of Randomized Controlled Trials,” Schizophrenia Research, Vol. 35, No. 1, 1999, pp. 51-68. doi:10.1016/S0920-9964(98)00105-4 [37] I. R. de Olivera, A. M. Mirand-Scippa, E. P. de Sena, E. L. Pereira, M. G. Ribeiro, E. de Castro-e-Silva and J. Ba- caltchuk, “Risperidone versus Haloperidol in the Treat- ment of Schizophrenia: A Meta-Analysis Comparing Their Efficacy and Safety,” Journal of Clinical Pharma- cology & Therapeutics, Vol. 21, No. 5, 1996, pp. 349-358. doi:10.1111/j.1365-2710.1996.tb00030.x [38] R. Tandon, R. H. Belmaker, W. F. Gattaz, J. J. Lopez-Iber Jr., A. Okasha, B. Singh, D. J. Stein, J. P. Olie, W. W. Fleischhacker and H. J. Moeller, “World Psychiatric As- sociation Pharmacopsychiatry Section Statement on Com- parative Effect of Antipsychotic in the Treatment of Schi- zophrenia,” Schizophrenia Research, Vol. 100, No. 1-3, 2008, pp. 20-38. doi:10.1016/j.schres.2007.11.033 [39] M. O. Bakare, “Effective Therapeutic Dosage of Antip- sychotic Medications in Patients with Psychotic Symp- toms: Is There a Racial Difference?” BMC Research Notes, Vol. 1, No. 1, 2008, pp. 1-25. [40] M. L. Chen, “Ethnic or Racial Differences Revisited: Im- pact of Dosage Regimen and Dosage form on Pharma- cokinetics and Pharmacodynamics,” Clinical Pharma- cokinetics, Vol. 45, No. 10, 2006, pp. 957-964. doi:10.2165/00003088-200645100-00001
|