J. J. ESTRADA ET AL. 471
4. Discussion
The management of rectal cancer has dramatically
changed of the last 30 years. The use of neo-adjuvant
therapy and total mesorectal excision has significantly
improved the overall survival for patients diagnosed with
rectal cancer [10-13]. The treatment algorithms for pa-
tients with potentially curable disease have been well
established and effective. Despite maximal treatment, the
overall survival for patients with stage IV disease re-
mains poor. Furthermore, many patients spend a signifi-
cant number of their last days hospitalized for the man-
agement of complications related to their disease. The
optimal treatment strategies for these patients remain
controversial. While many studies have focused on de-
termining which treatment maximizes the overall sur-
vival, few have focused on the implication of a recom-
mended treatment on the patients quality life.
It has been well documented [11,14-17] that radiation
therapy improves palliation in patients with unresectable
rectal cancer with regards to pain and bleeding. But pa-
tients may still require frequent hospitalization for the
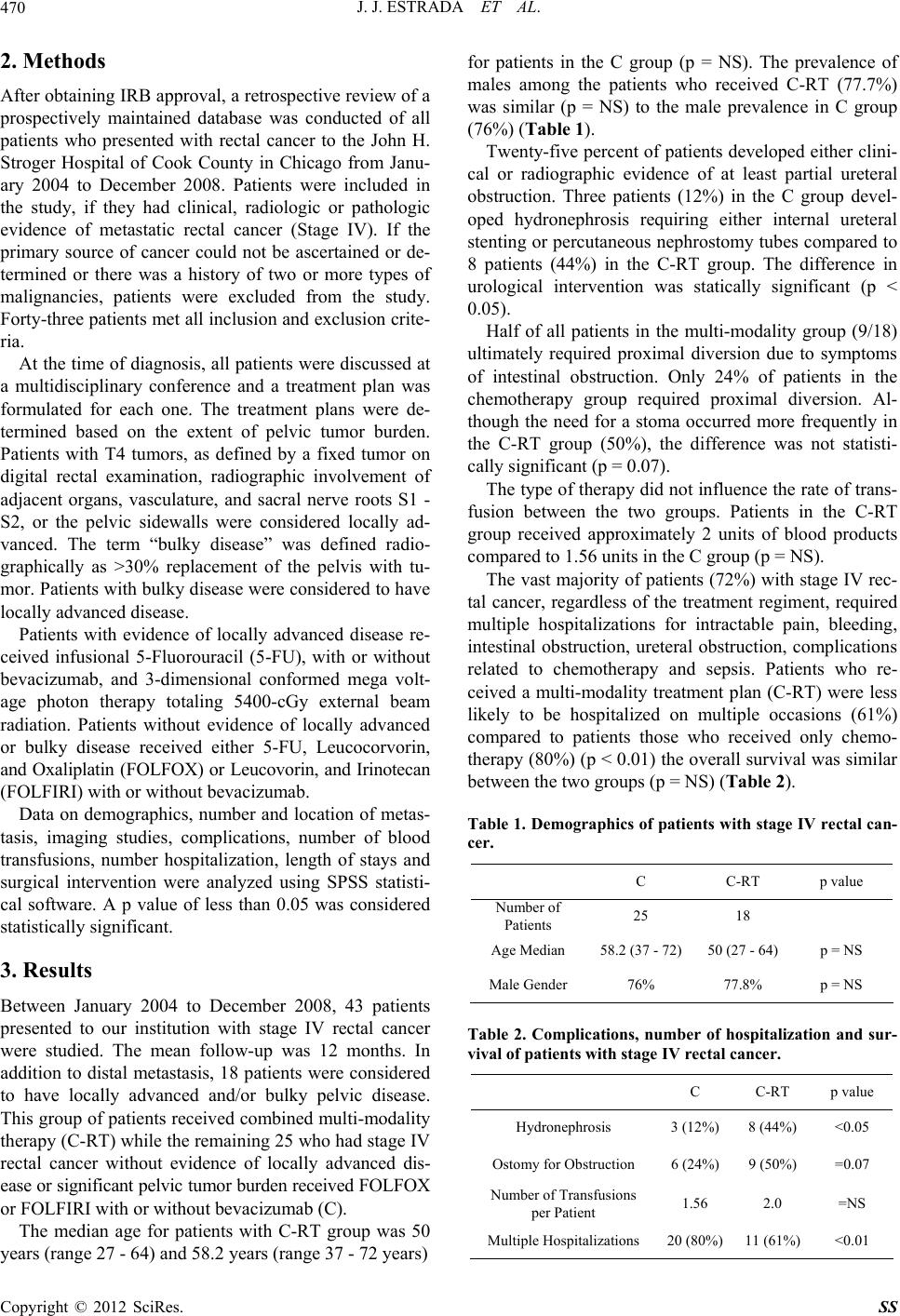
management of other complications. In our series, 72%
of all patients required multiple impatient hospital visits.
Fewer patients required multiple hospitalizations when
they received a combination of chemotherapy and radia-
tion rather than chemotherapy alone 61% vs. 80% (p <
0.01). This finding was somewhat surprising because the
patients who received multi-modality therapy tended to
have a significant tumor burden in the pelvis. This is
clearly evidenced by the fact that more patients in the
C-RT required proximal fecal diversion ureteral instru-
mentation, and blood transfusions. However, despite
these findings, patients required fewer inpatient hospital
visits.
One potential reason for the fewer observed inpatient
hospitalizations could be explained by the greater length
of stay (LOS) for the C-RT group. The mean LOS was
almost twice as long for the patients in the C-RT group
(17.3 vs. 8.9 days). However, three patients with ex-
tremely advanced disease dramatically influenced the
LOS. The mean LOS for these three patients was 78 days.
When these three patients are excluded, the LOS for the
C-RT group is 5.2 days. While hospice services were
suggested for the patients with the most advance disease,
these three patients elected to pursue a more aggressive
treatment strategy.
Although, formal qu ality of life surveys were not used
in this study, one may infer that less hosp ital visits could
translate into an improved quality of life. Larger pro-
spective randomized studies are needed to investigate
and validate this finding .
5. Conclusion
Chemo-radiation for patients with locally advanced un-
resectable stage IV rectal cancer is not a well established
protocol. In our series patients treated with C-RT for
bulky stage IV rectal cancer required fewer hospitaliza-
tions when compared to stage IV rectal cancer patients
treated with chemotherapy alone. In the properly selected
patient, fewer hospital visits may improve the quality of
life of patients with unresectable stage IV rectal cancer.
REFERENCES
[1] American Cancer Society, “Colorectal Cancer Facts &
Figures 2011-2013,” American Cancer Society, Atlanta,
2011.
[2] S. M. Ronnekleiv-Kelly and G. D. Kennedy, “Manage-
ment of Stage IV Rectal Cancer: Palliative Options,”
World Journal of Gastroenterology, Vol. 17, No. 7, 2011,
pp. 835-847. doi:10.3748/wjg.v17.i7.835
[3] A. Jemal, R. Siegel, E. Ward, Y. Hao, J. Xu and M. J.
Thun, “Cancer Statistics, 2009,” CA: A Cancer Journal
for Clinicians, Vol. 59, No. 4, 2009, pp. 225-249.
doi:10.3322/caac.20006
[4] R. Stangl, A. Altendorf-Hofmann, R. M. Charnley and J.
Scheele, “Factors Influencing the Natural History of Co-
lorectal Liver Metastases,” Lancet, Vol. 343, No. 8910,
1994, pp. 1405-1410.
doi:10.1016/S0140-6736(94)92529-1
[5] R. J. Heald and R. D. H. Ryall, “Recurrence and Survival
after Total Mesorectal Excision for Rectal Cancer,” Lan-
cet, Vol. 327, No. 8496, 1986, pp. 1479-1482.
doi:10.1016/S0140-6736(86)91510-2
[6] J. K. MacFarlane, R. D. H. Ryall and R. J. Heald, “Me-
sorectal Excision for Rectal Cancer,” Lancet, Vol. 341,
No. 8843, 1993, pp. 457-460.
doi:10.1016/0140-6736(93)90207-W
[7] Swedish Rectal Cancer Trial, “Improved Survival with
Preoperative Radiotherapy in Resectable Rectal Cancer,”
The New England Journal of Medicine, Vol. 336, No. 14,
1997, pp. 980-987. doi:10.1056/NEJM199704033361402
[8] C. Camma, M. Giunta, F. Fiorica, et al., “Preoperative
Radiotherapy for Resectable Rectal Cancer: A Meta-Ana-
lysis,” Journal of American Medical Association, Vol. 284,
No. 8, 2000, pp. 1008-1015.
doi:10.1001/jama.284.8.1008
[9] A. DeGramont, J. F. Bosset, C. Milan, P. Rougier, O.
Bouché, P. L. Etienne, F. Morvan, C. Louvet, T. Guillot,
E. François and L. Bedenne, “Randomized Trial Com-
paring Monthly Low-Dose Leucovorin and Fluorouracil
Bolus with Bimonthly High-Dose Leucovorin and Fluo-
rouracil Bolus Plus Continuous Infusion for Advanced
Colorectal Cancer: A French Intergroup Study,” Journal
of Clinical Oncology, Vol. 15, No. 2, 1997, pp. 808-815.
[10] T. Kramer, R. Share, K. Kiel, et al., “Intraoperative Ra-
diation Therapy of Colorectal Cancer,” In: M. Abe, Ed.,
Intraoperative Radiation Therapy, Pergamon Press, New
York, 1991, pp. 308-310.
[11] I. D. Nagtegaal, C. A. Marijnen, E. K. Kranenbarg, et al.,
“Circumferential Margin Involvement Is Still an Impor-
tant Predictor of Local Recurrence in Rectal Carcinoma:
Copyright © 2012 SciRes. SS