Paper Menu >>
Journal Menu >>
 Surgical Science, 2010, 1, 20-23 doi:10.4236/ss.2010.11004 Published Online July 2010 (http://www.SciRP.org/journal/ss) Copyright © 2010 SciRes. SS Isolated Mediastinal Lymphangioma: Pr enatal Diagnosis and Thoracoscopic Treatmen t Varlet F.1, Guye E.1, Varlet M. N.2, Tronchet M.2, Maria t G.3, Chene G.2 1Departments of Pediatric Surgery, Centre Hospitalier Universitaire, Saint-Etienne, France 2Obstetrics and Gynecol o gy, C ent re Hos pi ta l i e r Universit aire, Saint-Eti en ne, France 3Anesthesiology Centre Hospitalier Universitaire, Saint-Etien ne, France E-mail: chenegautier@ yahoo.fr Received June 12, 2010; accepted July 13, 2010 Abstract Isolated mediastinal lymphangiomas are uncommon. We report a case of a 14 × 8 mm right paracardiac cyst diagnosed at 20 weeks’ gestation. The prenatal evolution was uneventful and a magnetic resonance im aging at 31 weeks showed the limited extension of the cyst into the anterior mediastinum. At birth, the baby was asymptomatic, but the size of the lesion increased steadily (48 × 29 mm). At 7 months of life, he underwent a thoracoscopic resection of the cyst without intra or postoperative complications. Histological examination showed a lymphangioma. This case is remarkable for its prenatal diagnosis, the thoracoscopic treatment and the 8 years of follow-up without recurrence. Keywords: Mediastinal Tumor; Mediastinal Lymphangioma; Thoracoscopic Treatment; Prenatal Diagnosis 1. Introduction Isolated anterior mediastinal lymphangiomas (ML) are uncommon, with an occurrence less than 1% of all the lymphangiomas [1], and most of them are asymptomatic during childhood. They can lead to compression of vital structures, even life-threatening airway compromise. A prenatal diagnosis is now possible, but several patholo- gies can be evocated when a paracardial cystic lesion is discovered. Once diagnosed, they should be resected, typically by thoracotomy or median sternotomy. We re- port a case of ML with prenatal diagnosis and thoraco- scopic treatment. 2. Case Report An 8 months old boy presented a 14 × 8 mm anecho- genic right-sided anterior mediastinal cyst, which had been diagnosed at 20 weeks’ gestation by ultrasono- graphic examination (Figure 1) and confirmed by mag- netic resonance imaging (MRI) at 31 weeks’ gestation (Figure 2). At 34 weeks, the cyst was heterogeneous and measured 27 × 23 mm (Figure 3), but no complications were observed during the pregnancy and the baby was delivered at 37 weeks, weighing 2870 g, without respi- ratory distress. In the first week of life, sonography and MRI showed a 33 × 26 mm cyst and it was decided to delay resection for a few months. By 7 months, the cyst had enlarged to 48 × 29 mm, without respiratory com- plication, and the baby was operated on account of this evolution. In the operating room, the patient was placed in left lateral decubitus position and 4 ports were neces- sary. The cyst was to the right of the thymus, close to the phrenic nerve. The posterior parietal pleura was opened over the cyst from its lower part and easily dissected off the thymus; the dissection was performed cephalad along the right phrenic nerve and the pedicle was ligated close to the superior vena cava. Pathological examination showed a typical lymphangioma. The postoperative course was uneventful and no phrenic palsy or pleural effusion was noted. The patient remains asymptomatic 8 years after surgical excision, without recurrence of the lym- phangioma. 3. Discussion Lymphangiomas are beni gn hamartomatous tumors of the lymphatic system and less than 1% of all cystic lym- phangiomas are purely mediastinal in origin [1]. They constitute about 3% of all mediastinal masses in children [2]. A prenatal diagnosis has already been reported in 8 cases for an isolated ML [3-10]. It may be s uspected when the sonographic examination shows a single or multilocated paracardiac anterior mediastinal cystic 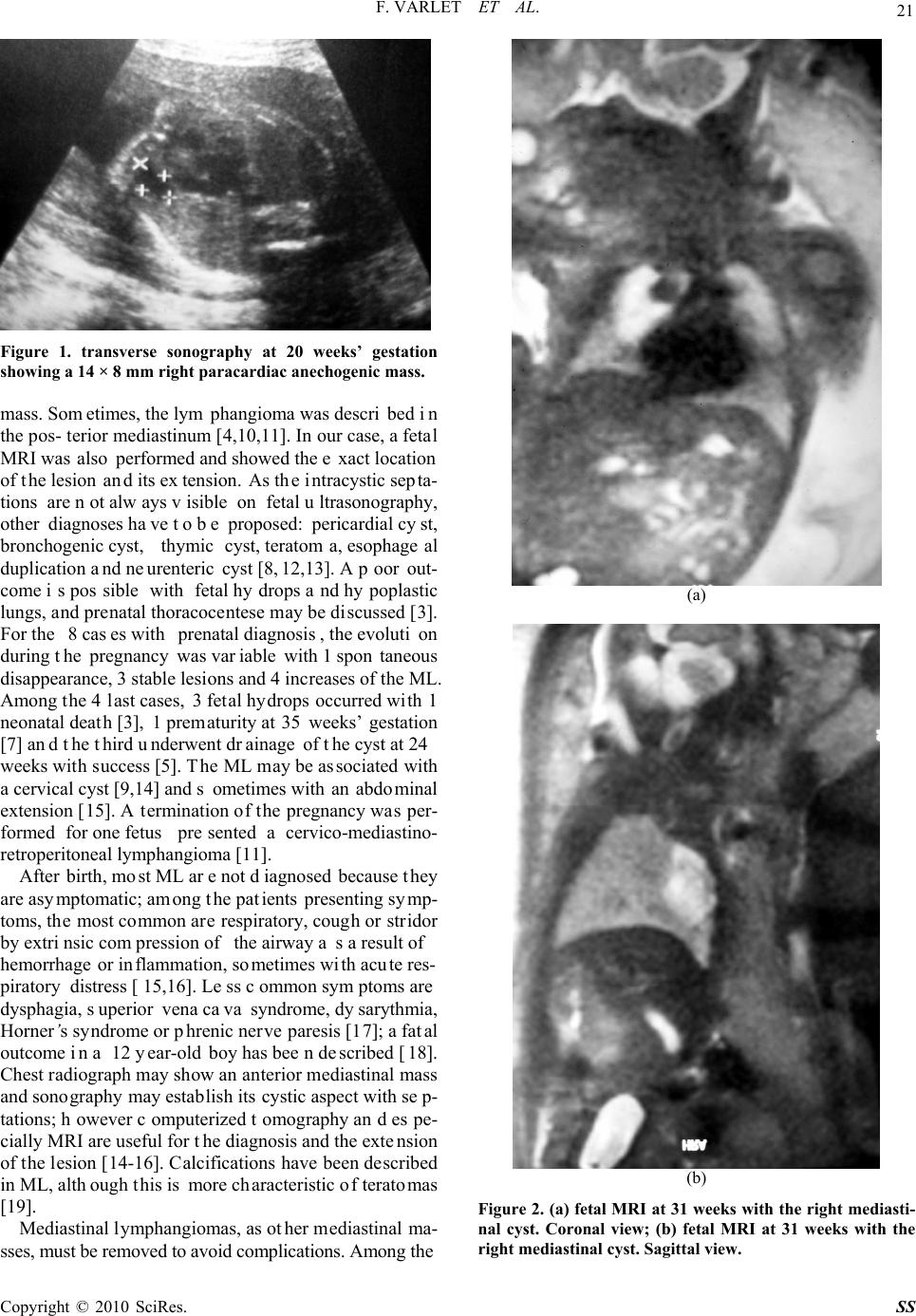 F. VARLET ET AL. 21 Figure 1. transverse sonography at 20 weeks’ gestation showing a 14 × 8 mm right paracardiac anechogenic mass. mass. Sometimes, the lymphangioma was described in the pos- terior mediastinum [4,10,11]. In our case, a fetal MRI was also performed and showed the exact location of the lesion and its extension. As the intracystic septa- tions are not always visible on fetal ultrasonography, other diagnoses have to be proposed: pericardial cyst, bronchogenic cyst, thymic cyst, teratoma, esophageal duplication and neurenteric cyst [8,12,13]. A poor out- come is possible with fetal hydrops and hypoplastic lungs, and prenatal thoracocentese may be discussed [3]. For the 8 cases with prenatal diagnosis, the evolution during the pregnancy was variable with 1 spontaneous disappearance, 3 stable lesions and 4 increases of the ML. Among the 4 last cases, 3 fetal hydrops occurred with 1 neonatal death [3], 1 prematurity at 35 weeks’ gestation [7] and the third underwent drainage of the cyst at 24 weeks with success [5]. The ML may be associated with a cervical cyst [9,14] and sometimes with an abdominal extension [15]. A termination of the pregnancy was per- formed for one fetus presented a cervico-mediastino- retroperitoneal lymphangioma [11]. After birth, most ML are not diagnosed because they are asymptomatic; among the patients presenting symp- toms, the most common are respiratory, cough or stridor by extrinsic compression of the airway as a result of hemorrhage or inflammation, sometimes with acute res- piratory distress [15,16]. Less common symptoms are dysphagia, superior vena cava syndrome, dysarythmia, Horner’s syndrome or phrenic nerve paresis [17]; a fatal outcome in a 12 year-old boy has been described [18]. Chest radiograph may show an anterior mediastinal mass and sonography may establish its cystic aspect with sep- tations; however computerized tomography and espe- cially MRI are useful for the diagnosis and the extension of the lesion [14-16]. Calcifications have been described in ML, although this is more characteristic of teratomas [19]. Mediastinal lymphangiomas, as other mediastinal ma- sses, must be removed to avoid complications. Among the (a) (b) Figure 2. (a) fetal MRI at 31 weeks with the right mediasti- nal cyst. Coronal view; (b) fetal MRI at 31 weeks with the right mediastinal cyst. Sagittal view. Copyright © 2010 SciRes. SS 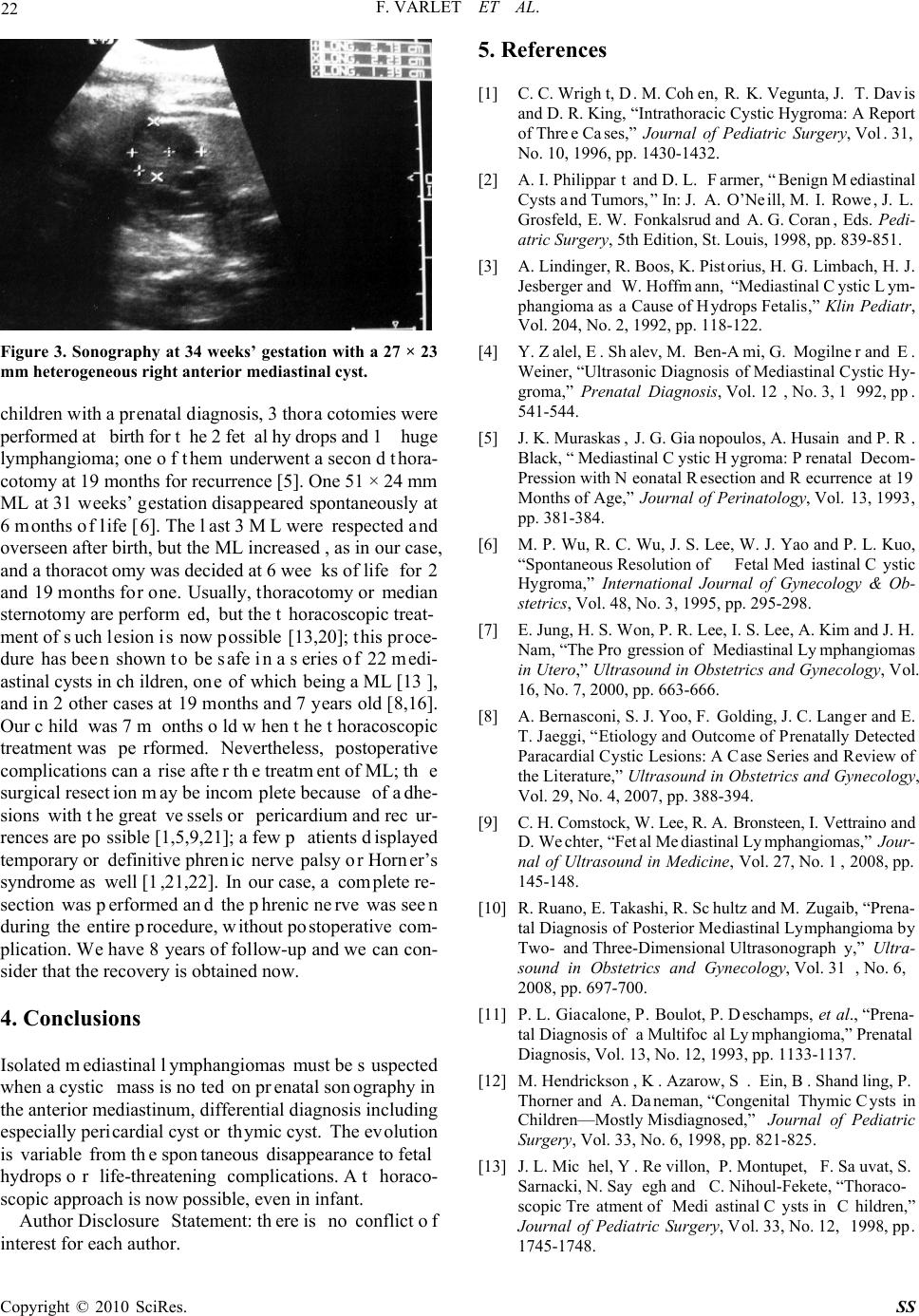 22 F. VARLET ET AL. Figure 3. Sonography at 34 weeks’ gestation with a 27 × 23 mm heterogeneous right anterior mediastinal cyst. children with a prenatal diagnosis, 3 thora cotomies were performed at birth for t he 2 fetal hydrops and 1 huge lymphangioma; one of them underwent a second thora- cotomy at 19 months for recurrence [5]. One 51 × 24 mm ML at 31 weeks’ gestation disappeared spontaneously at 6 months of life [6]. The last 3 ML were respected and overseen after birth, but the ML increased , as in our case, and a thoracotomy was decided at 6 weeks of life for 2 and 19 months for one. Usually, thoracotomy or median sternotomy are performed, but the thoracoscopic treat- ment of such lesion is now possible [13,20]; this proce- dure has been shown to be safe in a series of 22 medi- astinal cysts in children, one of which being a ML [13], and in 2 other cases at 19 months and 7 years old [8,16]. Our child was 7 m onths old when the thoracoscopic treatment was performed. Nevertheless, postoperative complications can arise after the treatment of ML; the surgical resection may be incomplete because of adhe- sions with the great vessels or pericardium and recur- rences are possible [1,5,9,21]; a few patients displayed temporary or definitive phrenic nerve palsy or Horner’s syndrome as well [1,21,22]. In our case, a complete re- section was performed and the phrenic nerve was seen during the entire procedure, without postoperative com- plication. We have 8 years of follow-up and we can con- sider that the recovery is obtained now. 4. Conclusions Isolated mediastinal lymphangiomas must be suspected when a cystic mass is noted on prenatal sonography in the anterior mediastinum, differential diagnosis including especially pericardial cyst or thymic cyst. The evolution is variable from the spontaneous disappearance to fetal hydrops or life-threatening complications. A thoraco- scopic approach is now possible, even in infant. Author Disclosure Statement: there is no conflict of interest for each author. 5. References [1] C. C. Wright, D. M. Cohen, R. K. Vegunta, J. T. Davis and D. R. King, “Intrathoracic Cystic Hygroma: A Report of Three Cases,” Journal of Pediatric Surgery, Vol. 31, No. 10, 1996, pp. 1430-1432. [2] A. I. Philippart and D. L. Farmer, “Benign Mediastinal Cysts and Tumors,” In: J. A. O’Neill, M. I. Rowe, J. L. Grosfeld, E. W. Fonkalsrud and A. G. Coran, Eds. Pedi- atric Surgery, 5th Edition, St. Louis, 1998, pp. 839-851. [3] A. Lindinger, R. Boos, K. Pistorius, H. G. Limbach, H. J. Jesberger and W. Hoffmann, “Mediastinal Cystic Lym- phangioma as a Cause of Hydrops Fetalis,” Klin Pediatr, Vol. 204, No. 2, 1992, pp. 118-122. [4] Y. Zalel, E. Shalev, M. Ben-Ami, G. Mogilner and E. Weiner, “Ultrasonic Diagnosis of Mediastinal Cystic Hy- groma,” Prenatal Diagnosis, Vol. 12, No. 3, 1992, pp. 541-544. [5] J. K. Muraskas, J. G. Gianopoulos, A. Husain and P. R. Black, “Mediastinal Cystic Hygroma: Prenatal Decom- Pression with Neonatal Resection and Recurrence at 19 Months of Age,” Journal of Perinatology, Vol. 13, 1993, pp. 381-384. [6] M. P. Wu, R. C. Wu, J. S. Lee, W. J. Yao and P. L. Kuo, “Spontaneous Resolution of Fetal Mediastinal Cystic Hygroma,” International Journal of Gynecology & Ob- stetrics, Vol. 48, No. 3, 1995, pp. 295-298. [7] E. Jung, H. S. Won, P. R. Lee, I. S. Lee, A. Kim and J. H. Nam, “The Progression of Mediastinal Lymphangiomas in Utero,” Ultrasound in Obstetrics and Gynecology, Vol. 16, No. 7, 2000, pp. 663-666. [8] A. Bernasconi, S. J. Yoo, F. Golding, J. C. Langer and E. T. Jaeggi, “Etiology and Outcome of Prenatally Detected Paracardial Cystic Lesions: A Case Series and Review of the Literature,” Ultrasound in Obstetrics and Gynecology, Vol. 29, No. 4, 2007, pp. 388-394. [9] C. H. Comstock, W. Lee, R. A. Bronsteen, I. Vettraino and D. Wechter, “Fetal Mediastinal Lymphangiomas,” Jour- nal of Ultrasound in Medicine, Vol. 27, No. 1, 2008, pp. 145-148. [10] R. Ruano, E. Takashi, R. Schultz and M. Zugaib, “Prena- tal Diagnosis of Posterior Mediastinal Lymphangioma by Two- and Three-Dimensional Ultrasonography,” Ultra- sound in Obstetrics and Gynecology, Vol. 31 , No. 6, 2008, pp. 697-700. [11] P. L. Giacalone, P. Boulot, P. Deschamps, et al., “Prena- tal Diagnosis of a Multifocal Lymphangioma,” Prenatal Diagnosis, Vol. 13, No. 12, 1993, pp. 1133-1137. [12] M. Hendrickson, K. Azarow, S . Ein, B. Shandling, P. Thorner and A. Daneman, “Congenital Thymic Cysts in Children—Mostly Misdiagnosed,” Journal of Pediatric Surgery, Vol. 33, No. 6, 1998, pp. 821-825. [13] J. L. Mic hel, Y. Revillon, P. Montupet, F. Sauvat, S. Sarnacki, N. Sayegh and C. Nihoul-Fekete, “Thoraco- scopic Treatment of Mediastinal Cysts in Children,” Journal of Pediatric Surgery, Vol. 33, No. 12, 1998, pp. 1745-1748. Copyright © 2010 SciRes. SS 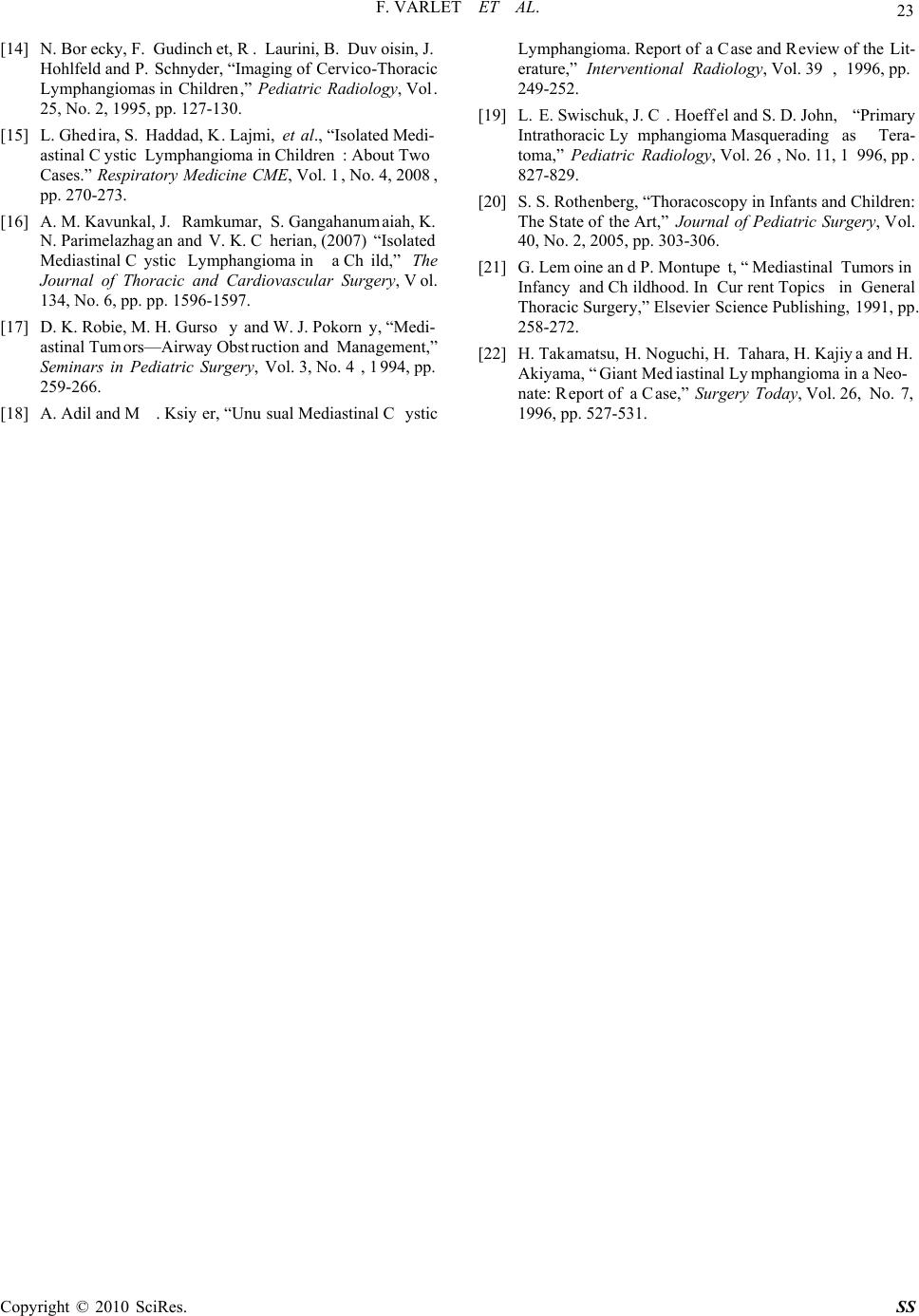 F. VARLET ET AL. Copyright © 2010 SciRes. SS 23 [14] N. Borecky, F. Gudinchet, R. Laurini, B. Duvoisin, J. Hohlfeld and P. Schnyder, “Imaging of Cervico-Thoracic Lymphangiomas in Children,” Pediatric Radiology, Vol. 25, No. 2, 1995, pp. 127-130. [15] L. Ghedira, S. Haddad, K. Lajmi, et al., “Isolated Medi- astinal Cystic Lymphangioma in Children: About Two Cases.” Respiratory Medicine CME, Vol. 1, No. 4, 2008, pp. 270-273. [16] A. M. Kavunkal, J. Ramkumar, S. Gangahanumaiah, K. N. Parimelazhagan and V. K. Cherian, (2007) “Isolated Mediastinal Cystic Lymphangioma in a Child,” The Journal of Thoracic and Cardiovascular Surgery, Vol. 134, No. 6, pp. pp. 1596-1597. [17] D. K. Robie, M. H. Gursoy and W. J. Pokorny, “Medi- astinal Tumors—Airway Obstruction and Management,” Seminars in Pediatric Surgery, Vol. 3, No. 4 , 1994, pp. 259-266. [18] A. Adil and M. Ksiyer, “Unusual Mediastinal Cystic Lymphangioma. Report of a Case and Review of the Lit- erature,” Interventional Radiology, Vol. 39 , 1996, pp. 249-252. [19] L. E. Swischuk, J. C . Hoeffel and S. D. John, “Primary Intrathoracic Lymphangioma Masquerading as Tera- toma,” Pediatric Radiology, Vol. 26, No. 11, 1996, pp. 827-829. [20] S. S. Rothenberg, “Thoracoscopy in Infants and Children: The State of the Art,” Journal of Pediatric Surgery, Vol. 40, No. 2, 2005, pp. 303-306. [21] G. Lemoine and P. Montupet, “Mediastinal Tumors in Infancy and Childhood. In Current Topics in General Thoracic Surgery,” Elsevier Science Publishing, 1991, pp. 258-272. [22] H. Takamatsu, H. Noguchi, H. Tahara, H. Kajiya and H. Akiyama, “Giant Mediastinal Lymphangioma in a Neo- nate: Report of a Case,” Surgery Today, Vol. 26, No. 7, 1996, pp. 527-531. |