Paper Menu >>
Journal Menu >>
 Surgical Science, 2010, 1, 15-19 doi:10.4236/ss.2010.11003 Published Online July 2010 (http://www.SciRP.org/journal/ss) Copyright © 2010 SciRes. SS Titanium Elastic Nails for Pediatric Femur Fracture s: Clinical and Radiological Study Nishikant Kumar*, Laljee Chaudhary Department of Ort h opaedics, Dar b ha n ga me di cal C ol l ege a nd Hospital, L aheriasar ai , Bi har, India E-mail: knishikant@ymail.com Received May 16, 2010; accepted July 14, 2010 Abstract Background: Management of femoral diaphyseal fractures in the age group 6-16 years is controversial. There has been a resurgence worldwide for operative fixation. Material and methods: Twenty children (15 boys, 5 girls) aged 6-16 years with femoral diaphyseal fractures (20 fractures, one in each) were stabilized with Titanium Elastic Nail (TEN). Patients underwent surgery within ten days of their injury. The results were evaluated using Flynn’s Scoring Criteria.Two nails were used in each fracture. Results: All 20 patients were available for evaluation and follow up for a mean duration of 24 months (15-32 months). Radiological union in all cases was achieved in a mean time of 8 weeks. Full weight bearing was possible in a mean time of 10 weeks (8-12 weeks). The results were excellent in 14 patients (70%) and successful in 6 patients (30%). Few complications that occurred were infection (in 2 cases), knee joint stiffness(in 4 cases), angulation less than 10 degrees( in 4 cases), shortening less than 10 mm(in 4 cases). Conclusion: Intramedullary fixation by TEN is an effective treatment of fracture of femur in properly selected patients of the 6-16 years age group. Keywords: Children, Intramedullary Fixation, Titanium Elastic Nail, Femoral Fracture, Diaphysis 1. Introduction Femoral shaft fracture is an incapacitating injury in chil- dren [1,2]. The treatment has traditionally been age re- lated, influenced by the type of injury, associated injuries and the location and type of fracture. The aim of fracture treatment is not only anatomical realignment, but also restoration of muscle and joint function as close as possible to the normal. Psychological recovery is accelerated by early resumption of functional activity, which encourages healing of fracture, mainte- nance of normal circulation, preservation of tone of the muscles and restoration of the movements of the joints. The aim therefore is early mobilization by early use of the injured part without movement at the fracture site. Because of rapid healing and spontaneous correction of angulations most of femoral shaft fractures in children younger than six years of age can be treated conserva- tively. Above six years of age all such fractures when treated non-operatively could have loss of reduction, malunion, intolerance and complication associated with plaster. Near the end of skeletal maturity accurate reduc- tion is necessary as angular deformity is no longer cor- rectable by growth. In skeletally mature adolescents, use of an antegrade solid locked intramedullary nail has be- come the standard of treatment. In patients between 6-16 years of age there has been a tendency towards operative approach. Titanium Elastic Nailing (TEN) which is variously known as elastic stable intramedullary nailing (ESIN), has become the choice of stabilization in pediatric long bone fractures, particularly the femoral shaft fracture. The present study is aimed at the evaluation of intramedullay fixation with TEN in children with femoral fractures. Until recently skeletal traction and application of a cast was the preferred method of treatment of diaphyseal femoral fractures in children and young adolescent. The device would exploit a child’s dense metaphyseal bone, rapid healing and abil- ity to remodel without risking damage to the epiphysis or the blood supply to the capital femoral epiphysis. 2. Material and Methods Twenty children (15 boys and 5 girls) in the age group of 6-16 years (average 10.8 years) with femoral shaft frac- ture were stabilized with TEN from April 2007 to Octo- ber 2009. The predominant mode of injury was due to fall from height (50%). Right-sided involvement was seen in 13 cas es (65%) and left side in 7 cases (35%). Mid-diaphyseal fracture of femur was found in 70% of  16 N. KUMAR ET AL. cases and subtrochanteric fracture in 30% cases. About 50% of the patients underwent surgery within 10 days of their injury. The surgery had been carried out in the De- partment of Orthopaedics, Darbhanga Medical College & Hospital, Laheriasarai, Darbhanga, Bihar, India. Nail comes in five diameters from 2.5 mm to 4.5 mm in a fixed length. The nails are colour coded for identifi- cation. The nails (Figure 1) are straight except for a bent tip. Special instruments include radiolucent reduction tool, nail holder, nail bender, Insertion device, nail ex- tractor, wice grip and a nail impactor were used. All the patients treated with TENs had skin/skeletal traction for approximately 1 week. As is the policy of our institution the traction pin (4.76 mm threaded Steinmann Pin) was inserted in the operating room under local an- aesthesia. The Pin was inserted in the region of tibial tuberosity anterolateral to posteromedial plane. Some patients were stabilised with skin traction. Compound fractures were primarily thoroughly debrided and upper tibial skeletal traction applied. The injured limb was put on a Bohler’s-Brawn splint and adequate weight applied. This is essen tial to minimize pain, muscle spasm and shortening. Appropriate tetanus prophylaxis, antibiotics and analgesics were instituted. In the period of rest and resuscitation, the patient was properly investigated and examined. As soon as the patient became fit for anaes- thesia and surgery he/she was posted for fixation of femoral shaft fractures with TEN. Good preoperative X-ray (Figure 2) of the injured femur was used to esti- mate the nail diameter and to develop an approach to supplement fixation and plan the incision. Half an hour before operation 1 ampoule of atropine was given intramuscularly. Intravenous line was setup. Prophylactic antibiotic 1 gm ceftriaxone was given in- travenously. 1 ampule perinorm was given intramuscu- larly. General/spinal (above 14 years) anaesthesia was given with full aseptic and antiseptic precautions on an image intensifier (IITV) compatible operation table. As soon as anaesthesia was effective, the patient was placed supine and upper tibial skeletal traction pin was removed with aseptic and antiseptic precaution. The pa- tient was placed on radiolucent fracture table. The limb was prepared and draped to give access to the entire fe- mur and knee joint and to permit manual manipulation of Figure 1. TEN with different length and diameter. Figure 2. Preoperative x-ray of femur (AP and Lat view). the thigh. The image intensifier was placed so that one could get antero-posterior and lateral view of the femoral shaft. The monitor was placed in such a way that surgeon could have clear vision when inserting the nail and re- ducing the fracture. The selection of the insertion point for the nails was medial and lateral at the top of the flare of the medial and lateral condyles so that after insertion they would tend to bind against the flare of the condyles. If the nails are inserted too low, they will tend to backout, which is a troublesome complication. In addition, the insertion should be posterior to mid line of the shaft so that if the nails backout, they will be less likely to enter the syno- vial pouch. A 5mm incision was made on the lateral side of the leg extending about two finger breadth above the superior pole of the Patella. (The superior pole of the patella lies slightly above the level of the physis). A guide wire for 6.5 mm cannulated screw was passed at 45 degrees angulation at the level of the superior pole of the patella. Over this a drill hole was made with the cannulated drill bit. Using a curved bone awl, the hole is extended cephalad to elongate the hole and avoid cracking of the cortex when the rod is inserted. The medial entry hole was similarly elongated using a curved bone awl in cephalad direction. The diameter of nail should be 2/5 of the internal diameter of t he medullary canal (Nail di- ameter = 0.4 x Canal diameter). Ideally, the lateral nail should extend to the level of the greater trochanter and the medial nail into the femo- ral neck. The amount of prebending should be equal for both the nails. (The amount of bending should be three times the inner diameter of the shaft).Both the nails were inserted through the entry holes one after another and were driven upto the fracture site. The reduction was helped by the use of F-tool which is a radiolucent device. The arms of the F-tool were readjusted depending on the fracture configuration and bulk of thigh viewing with the image intensifier. This nail was advanced about 2 cm and Copyright © 2010 SciRes. SS 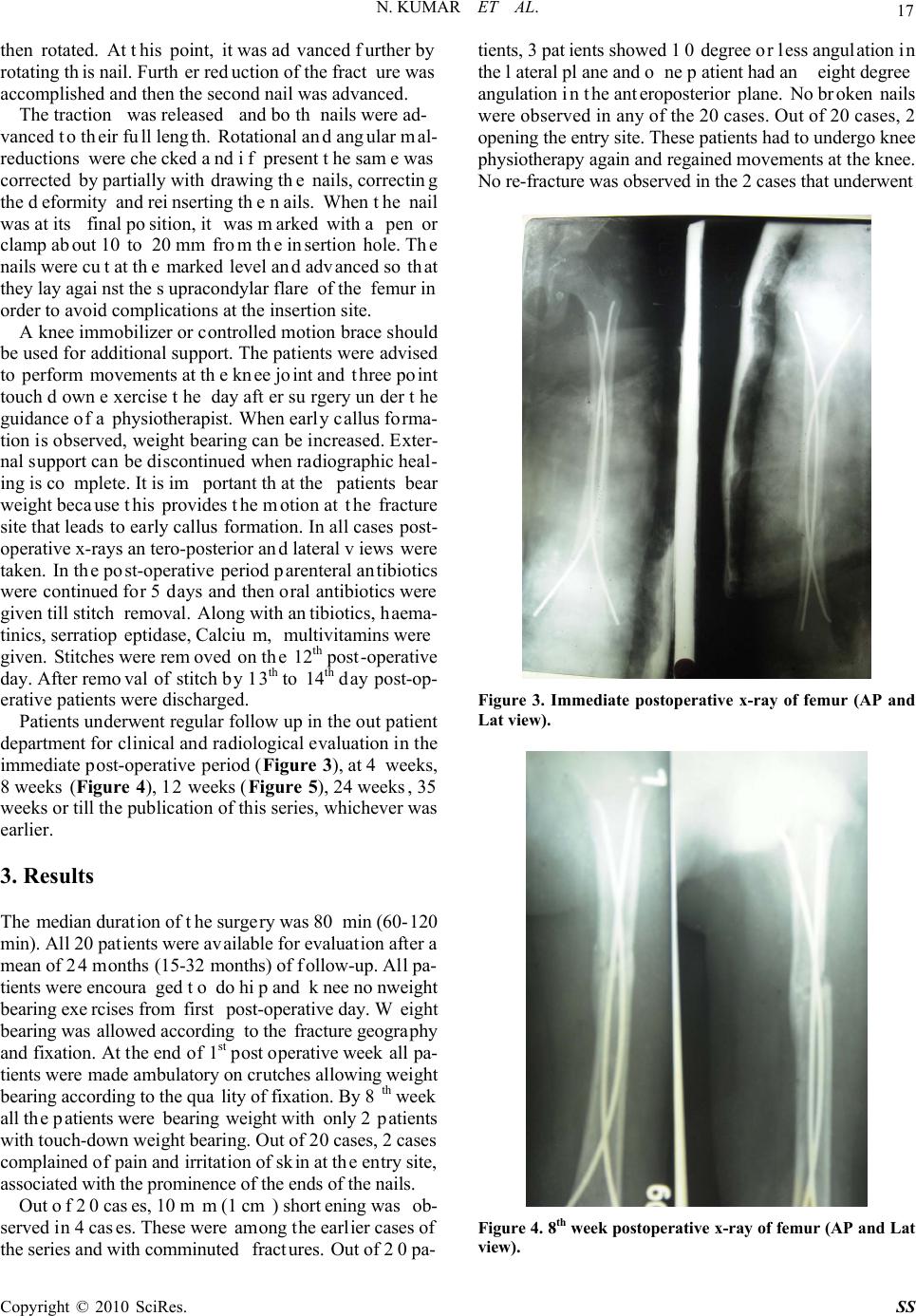 N. KUMAR ET AL. 17 then rotated. At this point, it was advanced further by rotating this nail. Further reduction of the fracture was accomplished and then the second nail was advanced. The traction was released and both nails were ad- vanced to their full length. Rotational and angular mal- reductions were checked and if present the same was corrected by partially withdrawing the nails, correcting the deformity and reinserting the nails. When the nail was at its final position, it was marked with a pen or clamp about 10 to 20 mm from the insertion hole. The nails were cut at the marked level and advanced so that they lay against the supracondylar flare of the femur in order to avoid complications at the insertion site. A knee immobilizer or controlled motion brace should be used for additional support. The patients were advised to perform movements at the knee joint and three point touch down exercise the day after surgery under the guidance of a physiotherapist. When early callus forma- tion is observed, weight bearing can be increased. Exter- nal support can be discontinued when radiographic heal- ing is co mplete. It is important that the patients bear weight because this provides the motion at the fracture site that leads to early callus formation. In all cases post- operative x-rays antero-posterior and lateral views were taken. In the post-operative period parenteral antibiotics were continued for 5 days and then oral antibiotics were given till stitch removal. Along with antibiotics, haema- tinics, serratiopeptidase, Calcium, multivitamins were given. Stitches were removed on the 12th post-operative day. After removal of stitch by 13th to 14th day post-op- erative patients were discharged. Patients underwent regular follow up in the out patient department for clinical and radiological evaluation in the immediate post-operative period (Figure 3), at 4 weeks, 8 weeks (Figure 4), 12 weeks (Figure 5), 24 weeks, 35 weeks or till the publication of this series, whichever was earlier. 3. Results The median duration of the surgery was 80 min (60-120 min). All 20 patients were available for evaluation after a mean of 24 months (15-32 months) of follow-up. All pa- tients were encoura ged to do hip and knee nonweight bearing exercises from first post-operative day. Weight bearing was allowed according to the fracture geography and fixation. At the end of 1st post operative week all pa- tients were made ambulatory on crutches allowing weight bearing according to the quality of fixation. By 8th week all the patients were bearing weight with only 2 patients with touch-down weight bearing. Out of 20 cases, 2 cases complained of pain and irritation of skin at the entry site, associated with the prominence of the ends of the nails. Out of 20 cases, 10 mm (1 cm) shortening was ob- served in 4 cases. These were among the earlier cases of the series and with comminuted fractures. Out of 20 pa- tients, 3 patients showed 10 degree or less angulation in the lateral plane and one patient had an eight degree angulation in the anteroposterior plane. No broken nails were observed in any of the 20 cases. Out of 20 cases, 2 opening the entry site. These patients had to undergo knee physiotherapy again and regained movements at the knee. No re-fracture was observed in the 2 cases that underwent Figure 3. Immediate postoperative x-ray of femur (AP and Lat view). Figure 4. 8th week postoperative x-ray of femur (AP and Lat view). Copyright © 2010 SciRes. SS 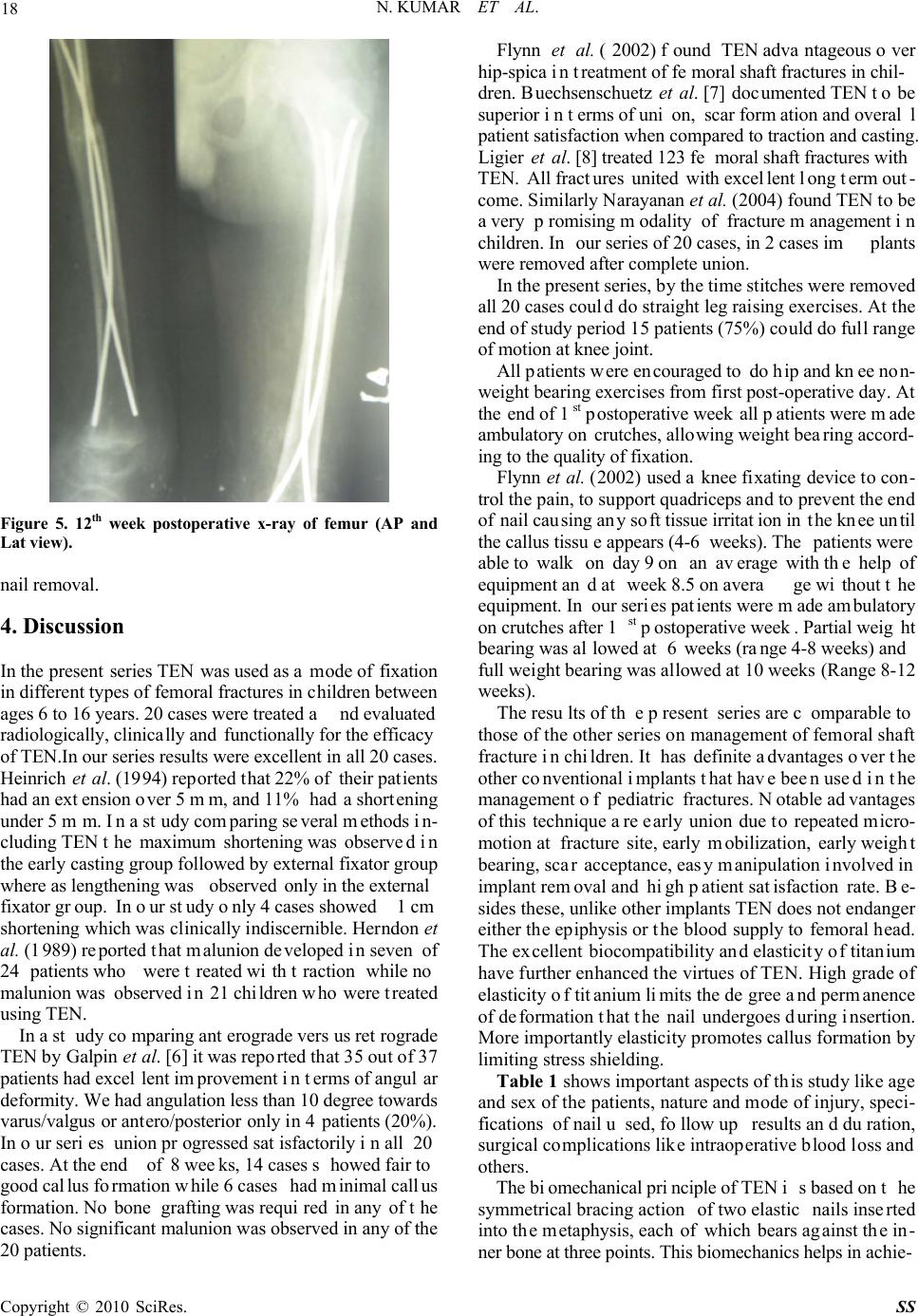 18 N. KUMAR ET AL. Figure 5. 12th week postoperative x-ray of femur (AP and Lat view). nail removal. 4. Discussion In the present series TEN was used as a mode of fixation in different types of femoral fractures in children between ages 6 to 16 years. 20 cases were treated and evaluated radiologically, clinically and functionally for the efficacy of TEN.In our series results were excellent in all 20 cases. Heinrich et al. (1994) reported that 22% of their patients had an extension over 5 mm, and 11% had a shortening under 5 mm. In a study comparing several methods in- cluding TEN the maximum shortening was observed in the early casting group followed by external fixator group where as lengthening was observed only in the external fixator group. In our study only 4 cases showed 1 cm shortening which was clinically indiscernible. Herndon et al. (1989) reported that malunion developed in seven of 24 patients who were treated with traction while no malunion was observed in 21 children who were treated using TEN. In a study comparing anterograde versus retrograde TEN by Galpin et al. [6] it was reported that 35 out of 37 patients had excellent improvement in terms of angular deformity. We had angulation less than 10 degree towards varus/valgus or antero/posterior only in 4 patients (20%). In our series union progressed satisfactorily in all 20 cases. At the end of 8 weeks, 14 cases showed fair to good callus formation while 6 cases had minimal callus formation. No bone grafting was required in any of the cases. No significant malunion was observed in any of the 20 patients. Flynn et al. (2002) found TEN advantageous over hip-spica in treatment of femoral shaft fractures in chil- dren. Buechsenschuetz et al. [7] documented TEN to be superior in terms of union, scar formation and overal l patient satisfaction when compared to traction and casting. Ligier et al. [8] treated 123 femoral shaft fractures with TEN. All fractures united with excellent long term out- come. Similarly Narayanan et al. (2004) found TEN to be a very promising modality of fracture management in children. In our series of 20 cases, in 2 cases implants were removed after complete union. In the present series, by the time stitches were removed all 20 cases could do straight leg raising exercises. At the end of study period 15 patients (75%) could do full range of motion at knee joint. All patients were encouraged to do hip and knee non- weight bearing exercises from first post-operative day. At the end of 1st postoperative week all patients were made ambulatory on crutches, allowing weight bearing accord- ing to the quality of fixation. Flynn et al. (2002) used a knee fixating device to con- trol the pain, to support quadriceps and to prevent the end of nail causing any soft tissue irritation in the knee until the callus tissue appears (4-6 weeks). The patients were able to walk on day 9 on an average with the help of equipment and at week 8.5 on average without the equipment. In our series patients were made ambulatory on crutches after 1st postoperative week. Partial weight bearing was allowed at 6 weeks (range 4-8 weeks) and full weight bearing was allowed at 10 weeks (Range 8-12 weeks). The results of th e present series are c omparable to those of the other series on management of femoral shaft fracture in children. It has definite advantages over the other conventional implants that have been used in the management of pediatric fractures. Notable advantages of this technique are early union due to repeated micro- motion at fracture site, early mobilization, early weight bearing, scar acceptance, easy manipulation involved in implant removal and high patient satisfaction rate. Be- sides these, unlike other implants TEN does not endanger either the epiphysis or the blood supply to femoral head. The excellent biocompatibility and elasticity of titanium have further enhanced the virtues of TEN. High grade of elasticity of titanium limits the degree and permanence of deformation that the nail undergoes during insertion. More importantly elasticity promotes callus formation by limiting stress shielding. Table 1 shows important aspects of this study like age and sex of the patients, nature and mode of injury, speci- fications of nail used, follow up results and duration, surgical complications like intraoperative blood loss and others. The biomechanical principle of TEN is based on the symmetrical bracing action of two elastic nails inserted into the metaphysis, each of which bears against the in- ner bone at three points. This biomechanics helps in achie- Copyright © 2010 SciRes. SS 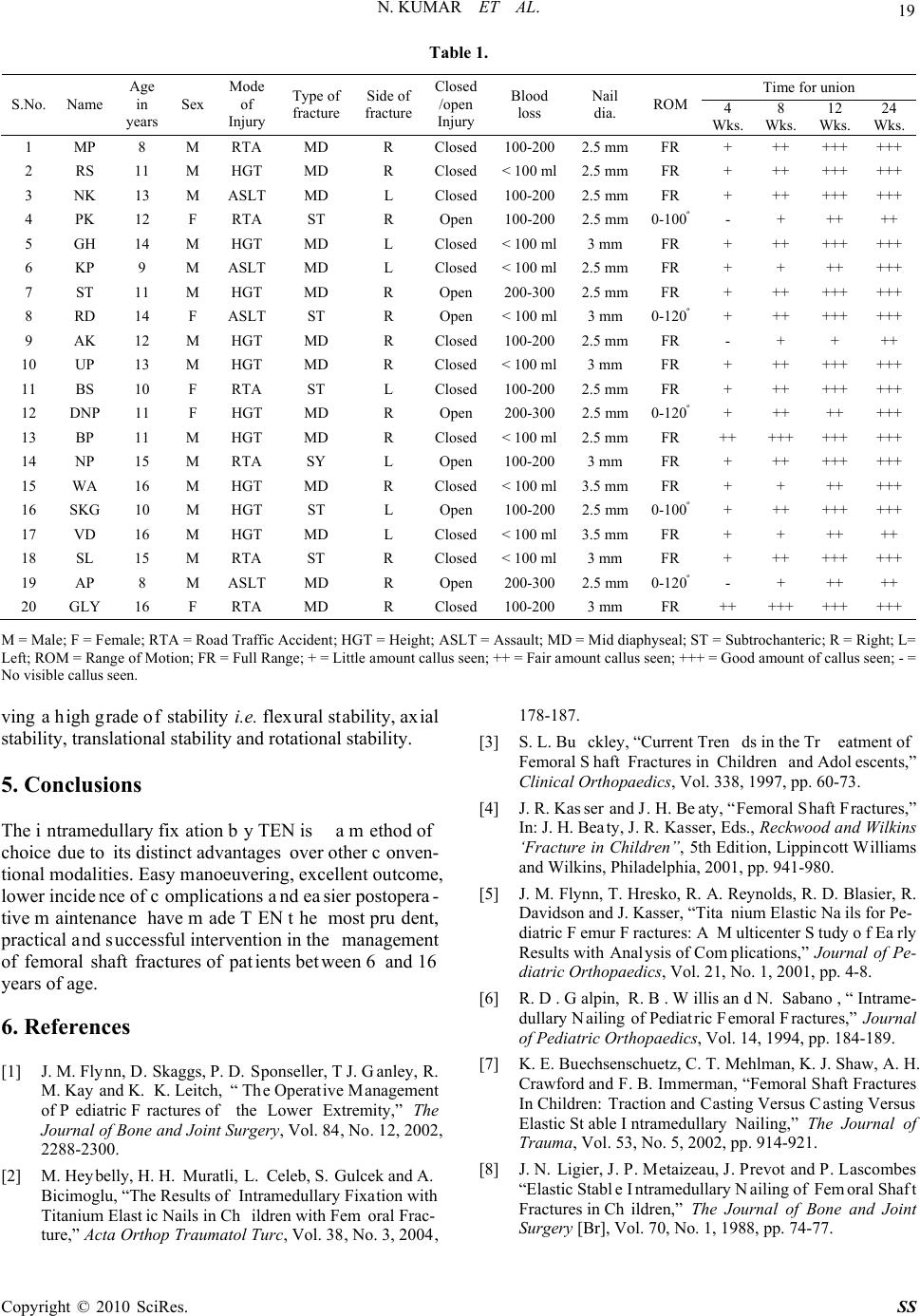 N. KUMAR ET AL. Copyright © 2010 SciRes. SS 19 Table 1. Time for union S.No. Name Age in years Sex Mode of Injury Type of fracture Side of fracture Closed /open Injury Blood loss Nail dia. ROM 4 Wks. 8 Wks. 12 Wks. 24 Wks. 1 MP 8 M RTA MD R Closed100-200 2.5 mmFR + ++ ++++++ 2 RS 11 M HGT MD R Closed< 100 ml2.5 mmFR + ++ ++++++ 3 NK 13 M ASLT MD L Closed100-200 2.5 mmFR + ++ ++++++ 4 PK 12 F RTA ST R Open 100-200 2.5 mm0-100º- + ++ ++ 5 GH 14 M HGT MD L Closed< 100 ml3 mm FR + ++ ++++++ 6 KP 9 M ASLT MD L Closed< 100 ml2.5 mmFR + + ++ +++ 7 ST 11 M HGT MD R Open 200-300 2.5 mmFR + ++ ++++++ 8 RD 14 F ASLT ST R Open < 100 ml3 mm 0-120º+ ++ ++++++ 9 AK 12 M HGT MD R Closed100-200 2.5 mmFR - + + ++ 10 UP 13 M HGT MD R Closed< 100 ml3 mm FR + ++ ++++++ 11 BS 10 F RTA ST L Closed100-200 2.5 mmFR + ++ ++++++ 12 DNP 11 F HGT MD R Open 200-300 2.5 mm0-120º+ ++ ++ +++ 13 BP 11 M HGT MD R Closed< 100 ml2.5 mmFR ++ +++ ++++++ 14 NP 15 M RTA SY L Open 100-200 3 mm FR + ++ ++++++ 15 WA 16 M HGT MD R Closed< 100 ml3.5 mmFR + + ++ +++ 16 SKG 10 M HGT ST L Open 100-200 2.5 mm0-100º+ ++ ++++++ 17 VD 16 M HGT MD L Closed< 100 ml3.5 mmFR + + ++ ++ 18 SL 15 M RTA ST R Closed< 100 ml3 mm FR + ++ ++++++ 19 AP 8 M ASLT MD R Open 200-300 2.5 mm0-120º- + ++ ++ 20 GLY 16 F RTA MD R Closed100-200 3 mm FR ++ +++ ++++++ M = Male; F = Female; RTA = Road Traffic Accident; HGT = Height; ASLT = Assault; MD = Mid diaphyseal; ST = Subtrochanteric; R = Right; L= Left; ROM = Range of Motion; FR = Full Range; + = Little amount callus seen; ++ = Fair amount callus seen; +++ = Good amount of callus seen; - = No visible callus seen. ving a high grade of stability i.e. flexural stability, axial stability, translational stability and rotational stability. 5. Conclusions The intramedullary fixation by TEN is a method of choice due to its distinct advantages over other conven- tional modalities. Easy manoeuvering, excellent outcome, lower incidence of complications and easier postopera- tive maintenance have made TEN the most prudent, practical and successful intervention in the management of femoral shaft fractures of patients between 6 and 16 years of age. 6. References [1] J. M. Flynn, D. Skaggs, P. D. Sponseller, T J. Ganley, R. M. Kay and K. K. Leitch, “ The Operative Management of Pediatric Fractures of the Lower Extremity,” The Journal of Bone and Joint Surgery, Vol. 84, No. 12, 2002, 2288-2300. [2] M. Heybelly, H. H. Muratli, L. Celeb, S. Gulcek and A. Bicimoglu, “The Results of Intramedullary Fixation with Titanium Elastic Nails in Children with Fem oral Frac- ture,” Acta Orthop Traumatol Turc, Vol. 38, No. 3, 2004, 178-187. [3] S. L. Buckley, “Current Trends in the Treatment of Femoral Shaft Fractures in Children and Adolescents,” Clinical Orthopaedics, Vol. 338, 1997, pp. 60-73. [4] J. R. Kasser and J. H. Beaty, “Femoral Shaft Fractures,” In: J. H. Beaty, J. R. Kasser, Eds., Reckwood and Wilkins ‘Fracture in Children”, 5th Edition, Lippincott Williams and Wilkins, Philadelphia, 2001, pp. 941-980. [5] J. M. Flynn, T. Hresko, R. A. Reynolds, R. D. Blasier, R. Davidson and J. Kasser, “Titanium Elastic Nails for Pe- diatric Femur Fractures: A Multicenter Study of Early Results with Analysis of Complications,” Journal of Pe- diatric Orthopaedics, Vol. 21, No. 1, 2001, pp. 4-8. [6] R. D. Galpin, R. B. Willis and N. Sabano, “Intrame- dullary Nailing of Pediatric Femoral Fractures,” Journal of Pediatric Orthopaedics, Vol. 14, 1994, pp. 184-189. [7] K. E. Buechsenschuetz, C. T. Mehlman, K. J. Shaw, A. H. Crawford and F. B. Immerman, “Femoral Shaft Fractures In Children: Traction and Casting Versus Casting Versus Elastic Stable Intramedullary Nailing,” The Journal of Trauma, Vol. 53, No. 5, 2002, pp. 914-921. [8] J. N. Ligier, J. P. Metaizeau, J. Prevot and P. Lascombes “Elastic Stable Intramedullary Nailing of Femoral Shaft Fractures in Children,” The Journal of Bone and Joint Surgery [Br], Vol. 70, No. 1, 1988, pp. 74-77. |