 Psychology 2012. Vol.3, Special Issue, 787-794 Published Online September 2012 in SciRes (http://www.SciRP.org/journal/psych) http://dx.doi.org/10.4236/psych.2012.329119 Copyright © 2012 SciRes. 787 Comorbidity of Depression and Diabetes: In a Nutshell Anisha Heeramun-Aubeeluck1, Zheng Lu1,2*, Yanli Luo1 1Department of Psychosomatic Medicine, Tongji Hospital, Shanghai, China 2Department of Adult Psychiatry, Shanghai Mental Health Center, Shanghai, China Email: *luzheng@tongji.edu.cn Received June 2nd, 2012; revised July 1st, 2012; accepted August 2nd, 2012 Depression and diabetes mellitus (DM) have existed since ages. Yet, the etiologies of both diseases are unclear till date. However, the effects resulting from these diseases are well documented. Comorbidity of both disorders leads to increase disability and mortality rates. Besides presenting the epidemiological status of depression in DM, this review aims to highlight the different hypotheses governing the associa- tion of depression in DM and summarize the current trend in detection and management of depression. A high index of suspicion is required to detect depression in diabetic patients. There seems to be higher prevalence of depression in type 2 diabetes than in type 1 diabetes. Treatment should be tailored as per the individual needs and presence of comorbidity. Though there is no gold standard treatment for depressive diabetics, combinations of both pharmacological and non-pharmacological interventions are likely to im- prove outcomes. Selective serotonin reuptake inhibitors (SSRIs) and selective norepinephrine reuptake inhibitors (SNRIs) are preferred to conventional antidepressants. Collaborative care, psychoeducation and behavioral interventions are helpful in motivating patients to maintain treatment and improve psycho- logical well-being and quality of life. Untreated depression in diabetics is costly to the health care and economic system as there is an increase in functional impairment and mortality rate. More efforts need to be made to effectively screen, diagnose and treat patients with comorbidity of diabetes and depression. Keywords: Diabetes Mellitus; Depression; Management; Epidemiology Introduction Thomas Willis (1621-1675), a famous British physician, was the first to describe the relationship between depression and diabetes mellitus. He claimed that diabetes was a consequence of prolonged sorrows (Willis, 1675). This concept has flour- ished over the past three centuries and still remains a hotly debated subject amongst researchers in psychosomatic medi- cine. Though the concept of mind-body unity and the effect of psychological factors on the course of general medical condi- tions are the crux of psychosomatic medicine, the exact mecha- nisms underlying depression in diabetes mellitus (DM) is yet unknown. Depression as per the World Health Organization (WHO) represents a common mental disorder. It is character- ized by depressed mood, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, low energy, and poor concentration. On a darker side, it is also associated with increased risk of suicidal behavior estimated at approxi- mately 850,000 lives per year (WHO, 2012). As per the Diag- nostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR), depression is classified as major depressive disorder. It can be further sub classified as single or recurrent episode. Degree of severity can also be specified and include mild, moderate and severe with/without psychotic fea- tures. The International Classification of Disease, 10th Edition (ICD-10) subdivides depression into depressive episode and recurrent depressive episode. Each type can be graded depend- ing on severity namely mild, moderate, and severe with or without psychotic symptoms. Furthermore, each diagnosis may be rated as with or without somatic syndrome. The diagnostic criteria between ICD-10 and DSM-IV have some differences. Depressive episode as per ICD-10 should last at least 2 weeks and for mild, moderate and severe episodes a total of at least 6, 8 and >8 symptoms must be met. Irrespective of the degree of the severity, ICD-10 requires any 2 of these core symptoms to be present: 1) Depressed mood sustained during almost all days for at least 2 weeks; 2) Loss of interest or pleasure; 3) Decreased energy or increased fatigability. Recurrent depressive disorder (ICD-10) is diagnosed when there has been one previous episode (mild, moderate or severe) which lasted at least 2 weeks and time period between the pre- vious episode and current one is a minimum of 2 months. The degree of severity is rated similar to depressive episode. On the other hand, as per DSM-IV-TR, major depressive disorder is characterized by a total of 5 or more symptoms lasting for a continuous 2 week period and a change from previous func- tioning. The core symptom of depression as per DSM-IV is one of these 2: 1) Depressed mood; 2) Loss of interest or pleasure. Recurrent major depressive disorder (DSM-IV-TR) repre- sents 2 more or previous episodes separated by a continuous 2 month period without depression. Severity is graded upon num- ber of symptoms and degree of impairment in social and occu- pational functioning. Dysthymia, which represents a chronic and milder depression is grouped under the depressive disorders constellation in DSM-IV-TR while in ICD-10, it represents persistent mood disorders. The diagnostic criteria for dysthymia in ICD-10 re- *Corresponding author.  A. HEERAMUN-AUBEELUCK ET AL. quire a minimum of 3 symptoms while DSM-IV-TR requires 2 symptoms. Though the duration is similar in both classification systems, the list of symptoms differ. DM is a metabolic disorder of multiple etiologies character- ized by chronic hyperglycemia with disturbances of carbohy- drate, fat and protein metabolism resulting from defects in insu- lin secretion, insulin action, or both. DM can be broadly classi- fied into four main categories namely: 1) Type 1 diabetes—onset usually in childhood and adoles- cence and results in β cell destruction leading to absolute insu- lin deficiency. 2) Type 2 diabetes—due to progressive insulin secretory de- fect superimposed on insulin resistance; common in adult with obesity, unhealthy diets and lack of physical activity. 3) Gestational diabetes mellitus—diabetes diagnosed during pregnancy but which has not yet reached overt diabetes). 4) Other categories such as drug-induced, genetic disorders, and exocrine pancreatic disorders. The diagnostic criteria for diabetes is either one of the fol- lowing: 1) A1C ≥ 6.5%. The test should be performed in a laboratory using a method that is National Glycohemoglobin Standardiza- tion Program (NGSP) certified and standardized to the Diabetes Control and Complications Trial (DCCT) reference assay. 2) FPG ≥ 126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 hours. 3) 2 hour plasma glucose ≥ 200 mg/dL (11.1 mmol/L) during an Oral Glucose Tolerance Test (OGTT). The test should be performed as described by the WHO, using a glucose load con- taining the equivalent of 75 g anhydrous glucose dissolved in water. The diagnosis of DM itself can be a major life stress event to an individual. Vulnerable subjects fail to cope with the complex and wide-arrayed physical and mental accommodations re- quired. Consequently, the affected individual may lose interest or lack energy in maintaining his diabetic management. Un- healthy eating habits are also frequent and may contribute to jeopardizing the control of DM. Risks of suicide through insu- lin overdose may also increase due to easy access to insulin. Furthermore, the complications of DM such as retinopathy, neuropathy and nephropathy overwhelm the already vulnerable subjects. These scenarios accentuate the seriousness of detect- ing and treating depression in DM. Besides presenting the epidemiological status of depression in DM, this review aims to highlight the different hypotheses governing the association of depression in DM and summarize the current trend in detection and management of depression. Epidemiological Status of Depression and DM As per Greden et al. (2003) depression was a serious global health issue affecting approximately 340 million people world- wide. The WHO survey conducted in 2000, depression was the 4th leading factor to global burden of disease in women while in men it was on 7th position (Ustun et al., 2004). The lifetime pre- valence of depression in different countries varied: US 16.6%, Europe 14%, Asia-Pacific 1.1% - 19.9% and South Africa 9.7% (Kessler et al., 2005; Alonso et al., 2005; Chui, 2004; Tomlin- son et al., 2009). A meta-analytical study had previously reported 11% of people with DM suffered from depression and that 31% of them had clinically relevant depression (Anderson et al., 2001). In a more recent systematic review the co-existence of DM and depression was confirmed (Egede & Ellis, 2010). Interest- ingly rates for undiagnosed depression in DM patients as per the study conducted by Li et al. (2008) equaled to 45%. The WHO World Health Survey studied adults aged 18 and above in 60 different countries worldwide and concluded that 1 year prevalence for depression in diabetes was 2% (Moussavi et al., 2007). TA systematic review reported the prevalence of depres- sion in young adults with type 1 diabetes as inconclusive (Johnson et al., 2012). On the other hand, a meta-analytic re- view supported claim for raised rate of depression in type 2 diabetes, which is also the most common type of diabetes (Ali et al., 2006). The International Diabetes Federation (IDF) estimated around 280 million people with DM in 2010 and this figure is thought to increase to 439 million in 2030 (IDF, 2009). DM currently holds the 7th place in cause of death (Murphy et al., 2012). With depression superimposed in DM, the mortality rate is likely to increase. Furthermore, there is evidence showing that depression was significantly associated with a wide range of diabetes complications with effect sizes of .17 - .32 (Groot et al., 2001). In sum, untreated depression is one of contributing factors for increased mortality rate in DM. Risk Factors for Depression in DM The feeling of “sadness” is a normal emotional reaction elic- ited by many events such as loss and disease. This reaction produces a variety of effects on the subject affecting his physi- cal appearance, physical and mental functioning (neurobiologi- cal, hormonal and psychological) as well as his family, social and occupational activities and relationships (Levenson, 2001). Genetic predisposition and/or childhood adverse events leading to maladaptive coping strategies increase the vulnerability of a person to depression. Coupled with multiple or recurrent stressful events, the subject with the above characteristics has a higher probability of developing depression. Furthermore, vul- nerability might also be increased due to unhealthy life style or behavior such as obesity, inadequate exercise, poor diet and smoking. There are several predisposing factors for comorbid- ity of depression and diabetes and include: 1) Age—A Canadian survey suggested that prevalence of depression in diabetic patients is higher in the younger age group (20 - 39 years) as compared to the middle aged groups (40 - 64 years). This finding has been supported by study con- ducted by Katon et al. (2004). In a survey of However, Trief (2007) argued that elderly (above 65 years) were also at high risk. A study in elderly Spanish revealed that diabetes was as- sociated with an increased risk of prevalent (odds ratio = 1.47) and incident (odds ratio = 1.40) depression. Another survey in elderly Chinese on Homg Kong found that of that 26% of eld- erly had diabetes and elevated depressive symptoms (Chou & Chi., 2005). 2) Gender—The impact of depression in diabetes is thought to be higher in females. A large prospective women cohort conducted in 11 US states found that women with diabetes and comorbid depression had increased mortality rate (95% C.I of 3.11) (Pan et al., 2011). However, it should be pointed out that generally fewer males than females seek treatment for depres- sion. Furthermore, depression in males is more likely to pro- duce irritability, anger or violent behavior rather than depressed Copyright © 2012 SciRes. 788 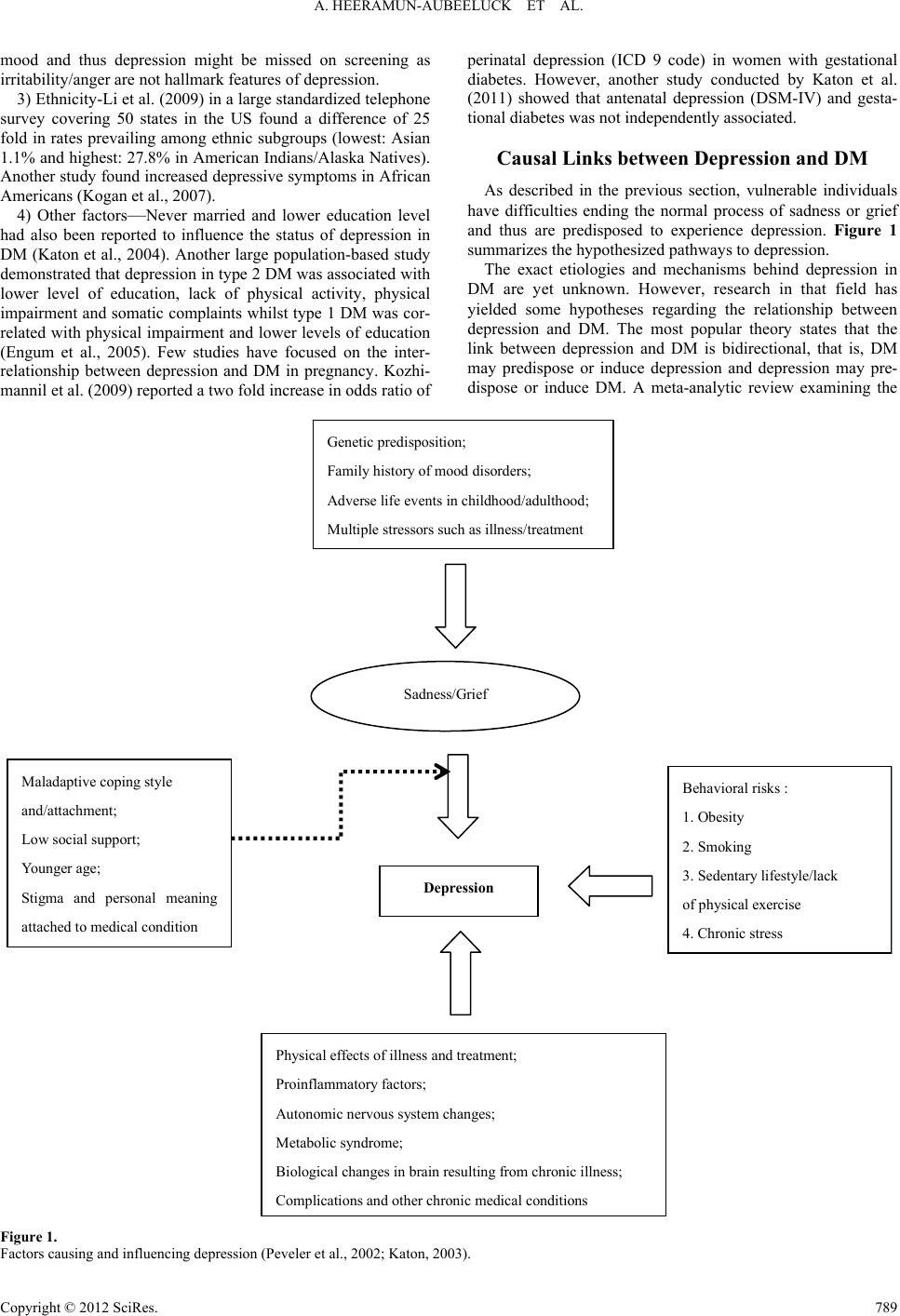 A. HEERAMUN-AUBEELUCK ET AL. Copyright © 2012 SciRes. 789 mood and thus depression might be missed on screening as irritability/anger are not hallmark features of depression. 3) Ethnicity-Li et al. (2009) in a large standardized telephone survey covering 50 states in the US found a difference of 25 fold in rates prevailing among ethnic subgroups (lowest: Asian 1.1% and highest: 27.8% in American Indians/Alaska Natives). Another study found increased depressive symptoms in African Americans (Kogan et al., 2007). 4) Other factors—Never married and lower education level had also been reported to influence the status of depression in DM (Katon et al., 2004). Another large population-based study demonstrated that depression in type 2 DM was associated with lower level of education, lack of physical activity, physical impairment and somatic complaints whilst type 1 DM was cor- related with physical impairment and lower levels of education (Engum et al., 2005). Few studies have focused on the inter- relationship between depression and DM in pregnancy. Kozhi- mannil et al. (2009) reported a two fold increase in odds ratio of perinatal depression (ICD 9 code) in women with gestational diabetes. However, another study conducted by Katon et al. (2011) showed that antenatal depression (DSM-IV) and gesta- tional diabetes was not independently associated. Causal Links between Depression and DM As described in the previous section, vulnerable individuals have difficulties ending the normal process of sadness or grief and thus are predisposed to experience depression. Figure 1 summarizes the hypothesized pathways to depression. The exact etiologies and mechanisms behind depression in DM are yet unknown. However, research in that field has yielded some hypotheses regarding the relationship between depression and DM. The most popular theory states that the link between depression and DM is bidirectional, that is, DM may predispose or induce depression and depression may pre- dispose or induce DM. A meta-analytic review examining the Sadness/Grief Behavioral risks : 1. Obesity 2. Smoking 3. Sedentary lifestyle/lack of physical exercise 4. Chronic stress Depression Maladaptive coping style and/attachment; Low social support; Younger age; Stigma and personal meaning attached to medical condition Physical effects of illness and treatment; Proinflammatory factors; Autonomic nervous system changes; Metabolic syndrome; Biological changes in brain resulting from chronic illness; Com lications and other chronic medical conditions Genetic predisposition; Family history of mood disorders; Adverse life events in childhood/adulthood; Multiple stressors such as illness/treatment Figure 1. Factors causing and influencing depression (Peveler et al., 2002; Katon, 2003). 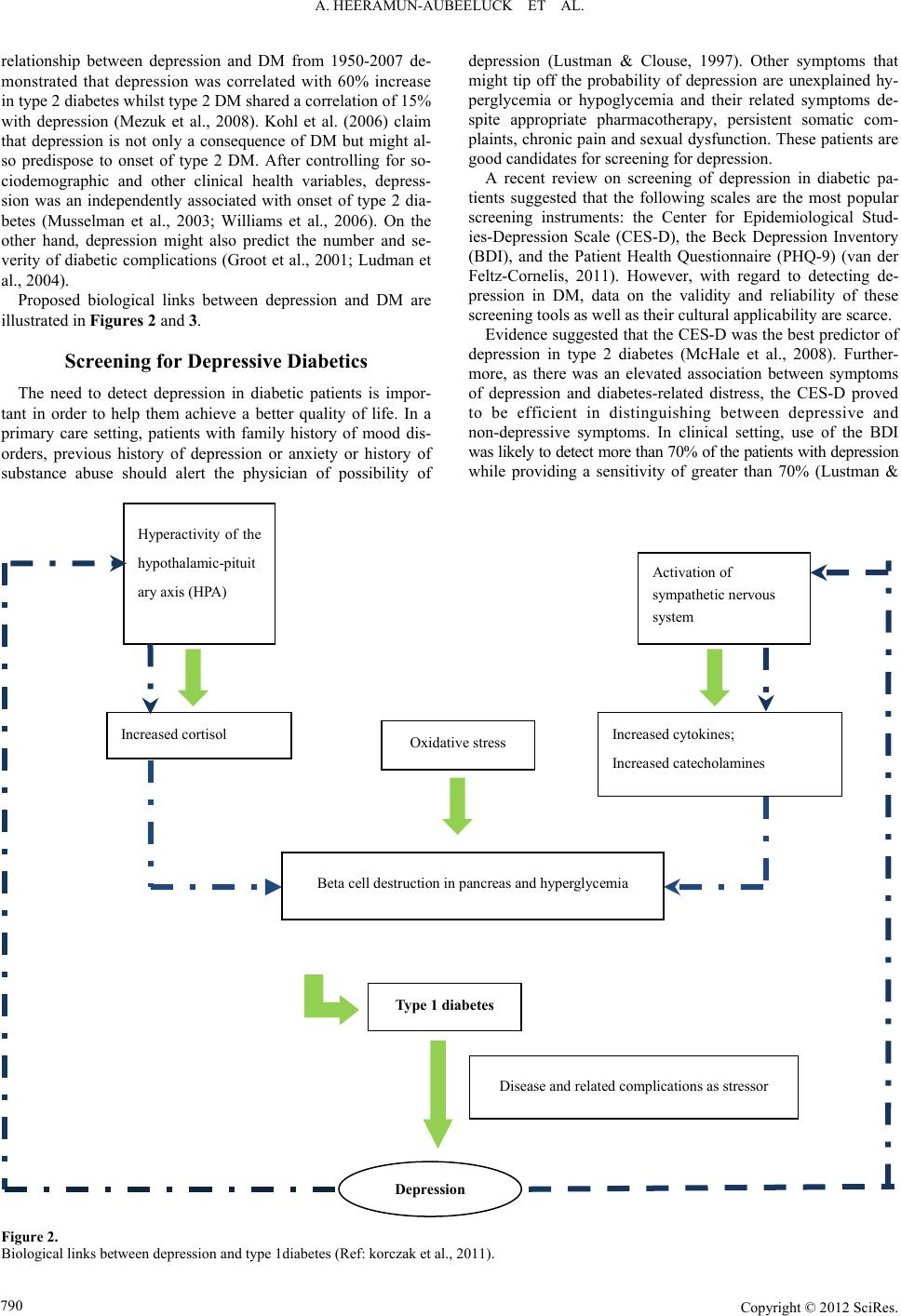 A. HEERAMUN-AUBEELUCK ET AL. relationship between depression and DM from 1950-2007 de- monstrated that depression was correlated with 60% increase in type 2 diabetes whilst type 2 DM shared a correlation of 15% with depression (Mezuk et al., 2008). Kohl et al. (2006) claim that depression is not only a consequence of DM but might al- so predispose to onset of type 2 DM. After controlling for so- ciodemographic and other clinical health variables, depress- sion was an independently associated with onset of type 2 dia- betes (Musselman et al., 2003; Williams et al., 2006). On the other hand, depression might also predict the number and se- verity of diabetic complications (Groot et al., 2001; Ludman et al., 2004). Proposed biological links between depression and DM are illustrated in Figures 2 and 3. Screening for Depressive Diabetics The need to detect depression in diabetic patients is impor- tant in order to help them achieve a better quality of life. In a primary care setting, patients with family history of mood dis- orders, previous history of depression or anxiety or history of substance abuse should alert the physician of possibility of depression (Lustman & Clouse, 1997). Other symptoms that might tip off the probability of depression are unexplained hy- perglycemia or hypoglycemia and their related symptoms de- spite appropriate pharmacotherapy, persistent somatic com- plaints, chronic pain and sexual dysfunction. These patients are good candidates for screening for depression. A recent review on screening of depression in diabetic pa- tients suggested that the following scales are the most popular screening instruments: the Center for Epidemiological Stud- ies-Depression Scale (CES-D), the Beck Depression Inventory (BDI), and the Patient Health Questionnaire (PHQ-9) (van der Feltz-Cornelis, 2011). However, with regard to detecting de- pression in DM, data on the validity and reliability of these screening tools as well as their cultural applicability are scarce. Evidence suggested that the CES-D was the best predictor of depression in type 2 diabetes (McHale et al., 2008). Further- more, as there was an elevated association between symptoms of depression and diabetes-related distress, the CES-D proved to be efficient in distinguishing between depressive and non-depressive symptoms. In clinical setting, use of the BDI was likely to detect more than 70% of the patients with depression while providing a sensitivity of greater than 70% (Lustman & Hyperactivity of the hypothalamic-pituit ary axis (HPA) Activation of sympathetic nervous system Oxidative stress Increased cortisol Increased cytokines; Increased catecholamines Beta cell destruction in pancreas and hyperglycemia Type 1 diabetes Depression Disease and related complications as stressor Figure 2. Biological links between depression and type 1diabetes (Ref: korczak et al., 2011). Copyright © 2012 SciRes. 790 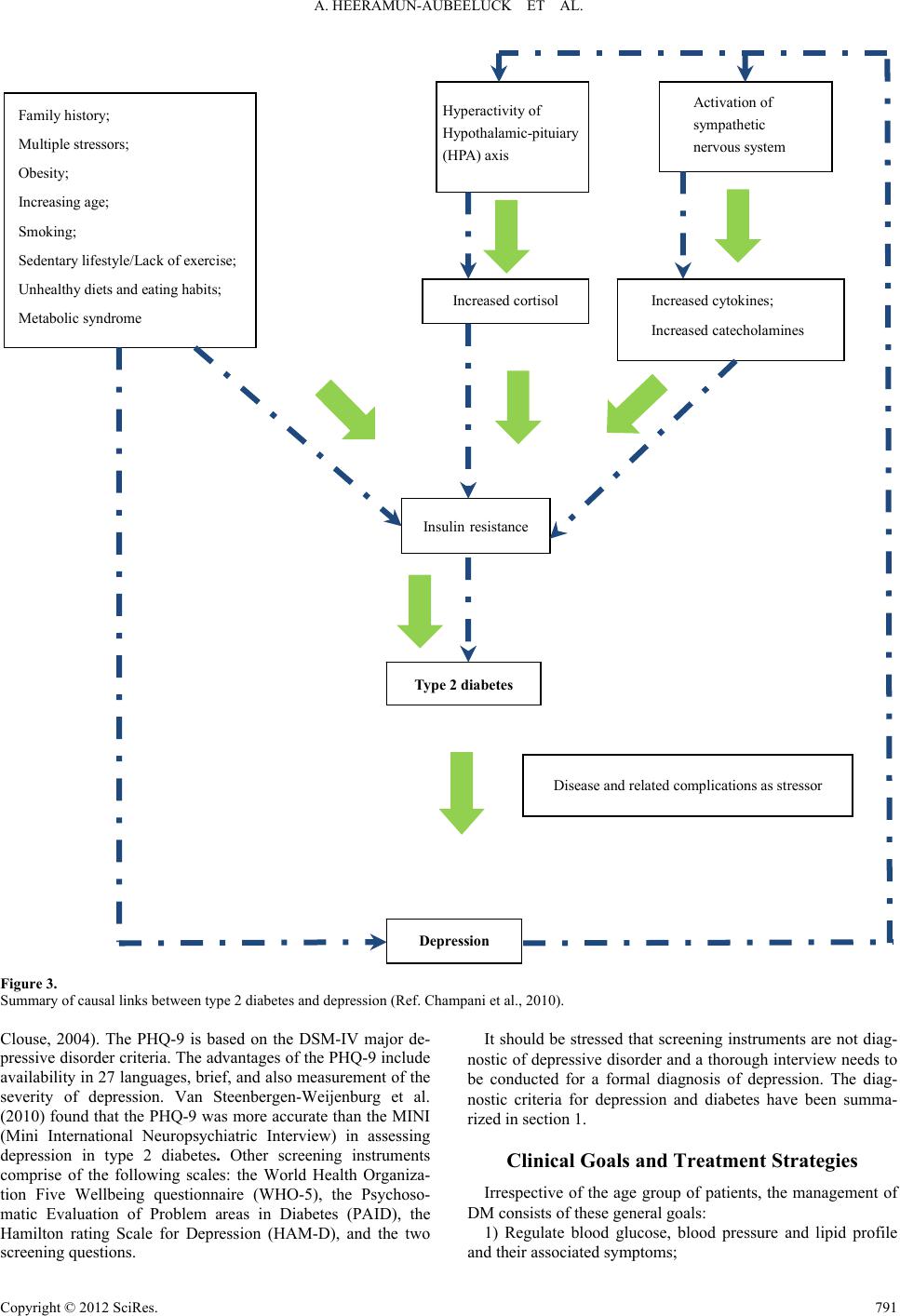 A. HEERAMUN-AUBEELUCK ET AL. Type 2 diabetes Increased cortisol Family history; Multiple stressors; Obesity; Increasing age; Smoking; Sedentary lifestyle/Lack of exercise; Unhealthy diets and eating habits; Metabolic syndrome Increased cytokines; Increased catecholamines Ins u li n resistance Disease and related complications as stressor Hyperactivity of Hypothalamic-pituiary (HPA) axis Activation of sympathetic nervous system Depression Figure 3. Summary of causal links between type 2 diabetes and depression (Ref. Champani et al., 2010). Clouse, 2004). The PHQ-9 is based on the DSM-IV major de- pressive disorder criteria. The advantages of the PHQ-9 include availability in 27 languages, brief, and also measurement of the severity of depression. Van Steenbergen-Weijenburg et al. (2010) found that the PHQ-9 was more accurate than the MINI (Mini International Neuropsychiatric Interview) in assessing depression in type 2 diabetes. Other screening instruments comprise of the following scales: the World Health Organiza- tion Five Wellbeing questionnaire (WHO-5), the Psychoso- matic Evaluation of Problem areas in Diabetes (PAID), the Hamilton rating Scale for Depression (HAM-D), and the two screening questions. It should be stressed that screening instruments are not diag- nostic of depressive disorder and a thorough interview needs to be conducted for a formal diagnosis of depression. The diag- nostic criteria for depression and diabetes have been summa- rized in section 1. Clinical Goals and Treatment Strategies Irrespective of the age group of patients, the management of DM consists of these general goals: 1) Regulate blood glucose, blood pressure and lipid profile and their associated symptoms; Copyright © 2012 SciRes. 791  A. HEERAMUN-AUBEELUCK ET AL. 2) Identify and treat macrovascular and microvascular com- plications; 3) Effective self-management by patients and 4) Improve or stabilize the general health status of patients. However, in practice only a small percentage of patients are able to reach the desired clinical goals. Various factors are thought to be implicated such as patient’s beliefs about disease, the severity of the disease, comorbid disorders, financial and economic status and availability of support. Qaseem et al. (2007) recommend that glycemic control should be based upon severity of disease and risk of complications, comorbidity, life expectancy, and patient’s preferences—thus treatment goals ought to be individualized. Diabetes coupled with depression tends to increase the dis- ease burden and functional impairment. As mentioned above primary care physicians need to have a high index of suspicion in detecting underlying depression in diabetic patients. In a longitudinal assessment of 998 adults with type 2 diabetes, Chui et al. (2010) found that general health behaviors (physical exercise, weight control, and smoking) explained 13% of the depression-hyperglycemic link. The association between de- pression and hyperglycemia has been replicated in other studies (Rush et al., 2008; Katon et al., 2004). Interestingly, Lustman et al., (2005) failed to establish diabetes self-care as a mediator between depression and hyperglycemia in type 1 diabetes. Nonetheless, lifestyle and health behaviors modification are essential in the management of depressive diabetic patients. Proposed strategies include: 1) Weight loss and exercise. Older patients are more likely to successfully meet these goals (Diabetes Prevention Program Research Group, 2004). Other beneficial effects of exercise include reduced abdominal adiposity, improved lipid profile, enhanced cardiac function and coronary blood flow and de- crease blood pressure. All these factors are directly and indi- rectly related to diabetes and its complications; 2) Reducing or quitting cigarette smoking and alcohol con- sumption; 3) Healthy diet: Increasing consumption of vegetables and fruits, reducing intake of fatty foods, monitoring caloric intake based on height and occupational requirement. Aggressive diets can lead to disastrous consequences in patient with low hypo- glycemic awareness. Furthermore, the adverse effects of tight glycemic control is said to increase exponentially with age. Treatment can be pharmacological, psychotherapeutic or combined interventions. A recent meta-analysis has deemed it effective to treat depression in diabetic patients (van der Feltz- Cornelis et al., 2010). The role of antidepressant and whether the class of antidepressant used had an influence on the glyce- mic control was not clarified in the meta-analysis. Echeverry et al. (2009) found significant association between treatment of depression with sertraline and decrease in A1C levels as well as systolic pressure in a low income Hispanic and African Ameri- can sample. The Pathways study, on the other hand, in its one year study did not find significant differences in A1C levels in between treatment group for depression and placebo group (Katon et al., 2004). Concern has also been raised regarding the role of antidepressant in causing DM. A large well-conducted trial found significant association between antidepressant use for depression and diabetes was nullified by lifestyle/risk fac- tors (Wilkins & Sambamoorthi, 2011). Another large trial in middle-aged patients also supported the theory of no causal relationship between antidepressant and DM (Kivimäki et al., 2011). Interestingly, in a large sample of multi-ethnic post- menopausal women, the use of antidepressants in women with longstanding or elevated depressive symptoms was signifi- cantly associated with a higher risk of DM (Ma et al., 2011). A review on antidepressant use in DM showed that selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine, par- oxetine, citalopram and sertraline not only improved depression but also helped in reducing glucose levels while nortriptyline (norepinephrine reuptake inhibitor, NRI) worsened the glucose control (Goodnick, 2001). Studies on conventional antidepres- sants have shown that they are liable to increase the risk of metabolic syndrome and hence DM (van Reedt Dortland et al., 2010; Mcintyre et al., 2010). Another antidepressant that has proved to be beneficial in comorbid depression and DM is mil- nacipran which is a serotonin and norepinephrine reuptake in- hibitor (SNRI) (Hoffman, 2010). Depressive diabetic patients with sexual dysfunction might benefit from the use of bu- propion which is a norepinephrine-dopamine reuptake inhibitor (Sayuk et al., 2011). Inadequate response to antidepressants in depressive type 2 diabetics might benefit from treating co-exist- ing symptoms such as pain and impairment (Anderson et al., 2010). Regarding psychotherapeutic interventions, as evidenced by findings of a systematic review, they helped improve the sever- ity of depression and had limited effects on the reduction of A1C levels (Wang et al., 2008). Nevertheless, studies which had focused on behavioral modifications or collaborative care in depressive diabetics had improved outcomes and adherence to medications. A combination of both pharmacotherapy and psychotherapeutic interventions might lead to better outcome measures and quality of life. Unfortunately, in real life, patients with new-onset depression and medical comorbidities might not be receiving adequate treatment (Gill et al., 2010). Conclusion Functional impairment as well as adverse effects caused by comorbidity of DM and depression is a fact. Due to the in- creasing number of both DM and depression and their hypothe- sized associations, identification and treatment is a must. How- ever, since DM has its own related diabetes-distress syndrome, diagnosis is tricky. A high index of suspicion is required as at times patients are unaware of their latent depression. Another difficulty likely to be encountered is that many diabetic patients have depressive symptoms which do not meet the criteria for a diagnosis of depression as per DSM-IV-TR or ICD-10. Fur- thermore, there is growing evidence that many patients given the diagnosis of depression are in fact having Bipolar II disor- der. Unfortunately, research on comorbidity of Bipolar II and diabetes is scarce. Since antidepressants are not the first choice for managing mild depression, patients with either subsyndro- mal depression or mild depression are more likely to benefit from added non-pharmacological approaches such as psy- choeducation, coping skills strategies and behavioral interven- tions to their regular treatment. These strategies could also be added to the treatment of diabetic patients with a formal diag- nosis of depression. Whatever strategies employed, they should be individualized to the person. From a different angle, in the long run, treated depressive diabetics might reduce the eco- nomic burden of these 2 diseases by reducing complications and functional impairment. Copyright © 2012 SciRes. 792  A. HEERAMUN-AUBEELUCK ET AL. REFERENCES Ali, S., Stone, M. A., Peters, J. L., Davies, M. J., & Khunti, K. (2006). The prevalence of co-morbid depression in adults with Type 2 dia- betes: A systematic review and meta-analysis. Diabetic Medicine, 23, 1165-1173. doi:10.1111/j.1464-5491.2012.03721.x Alonso, J. et al. (ESEMeD/MHEDEA 2000 Investigators) (2004). Pro- ject prevalence of mental disorders in Europe: Results from the Euro- pean Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatrica Scandinavica Suppletum, 420, 21-27. Anderson, R. J., Freedland, K. E., Clouse, R. E., & Lustman, P. J. (2001). The prevalence of comorbid depression in adults with diabetes: A meta-analysis. Diabetes Care, 24, 1069-1078. doi:10.2337/diacare.24.6.1069 Anderson, R. J., Gott, B. M., Sayuk, G. S., Freedland, K. E., & Lust- man, P. J. (2010). Antidepressant pharmacotherapy in adults with type 2 diabetes. Diabetes Care, 33, 485-489. doi:10.2337/dc09-1466 Champaneri, S., Wand, G. S., Malhotra, S. S., Casagrande, S. S., & Golden, S. H. (2010). Biological basis of depression in adults with diabetes. Current Diabetes Reports, 10, 396-405. Chiu, C. J., Wray, L. A., Beverly, E. A., & Dominic, O. G. (2010). The role of health behaviors in mediating the relationship between de- pressive symptoms and glycemic control in type 2 diabetes: A struc- tural equation modeling approach. Social Psychiatry and Psychiatric Epidemiology, 45, 67-76. doi:10.1007/s00127-009-0043-3 Chou, K. L, & Chi, I. (2005) Prevalence of depression among elderly Chinese with diabetes. International Journal of Geriatric Psychiatry, 20, 570-575. doi:10.1002/gps.1328 Chui, E. (2004). Epidemiology of depression in the Asia Pacific region. Australasian Psychiatry, 12, S4-S10. De Jonge, P., Roy, J. F., Saz, P., Marcos, G., & Lobo, A. (ZARADEMP Investigators) (2006). Prevalent and incident depression in commu- nity-dwelling elderly persons with diabetes mellitus: Results from the ZARADEMP project. Diabetologia, 49, 2627-2633. doi:10.1007/s00125-006-0442-x Echeverry, D., Duran, P., Bonds, C., Lee, M., & Davidson, M. B. (2009). Effect of pharmacological treatment of depression on A1C and qual- ity of life in low-income Hispanics and African Americans with dia- betes: A randomized, double-blind, placebo-controlled trial. Diabetes Care, 32, 2156-2160. doi:10.2337/dc09-0785 Egede, L. E., & Ellis, C. (2010). Diabetes and depression: Global per- spectives. Diabetes Research and Clinical P r a ctice, 87, 302-312. doi:10.1016/j.diabres.2010.01.024 Engum, A., Mykletun, A., Midthjell, K., Holen, A., & Dahl, A. (2005). Depression and diabetes: A large population-based study of socio- demographic, lifestyle, and clinical factors associated with depress- sion in type 1 and type 2 diabetes. Diabetes Care, 28, 1904-1909. doi:10.2337/diacare.28.8.1904 Gill, J. M., Klinkman, M. S., & Chen, Y. X. (2010). Antidepressant medication use for primary care patients with and without medical comorbidities: A national Electronic Health Record (EHR) network study. Journal of the American Board of Family Medicine, 23, 499- 508. doi:10.3122/jabfm.2010.04.090299 Goodnick, P. J. (2001). Use of antidepressants in treatment of comorbid diabetes mellitus and depression as well as in diabetic neuropathy. Annals of Clinical Psychia tr y , 13, 31-41. doi:10.3109/10401230109147127 Greden, J. F. (2003). Physical symptoms of depression: Unmet needs. Journal of Clinical Psychia t ry , 64, 5-11. Groot, M. D., Anderson, R., Freedland, K. E., Clouse, R. E., & Lust- man, P. J. (2001). Association of depression and diabetes complica- tions: A meta-analysis. Psychosomatic Medicine, 63, 619-630. Hoffman, P. (2010). Treatment of patients with comorbid depression and diabetes with metformin and milnacipran. Neuropsychiatric Di- sease and Treatment, 6, 9-15. International Diabetes Federation (2009). Diabetes Atlas (4th ed.). Brus- sels: International Diabetes Federation. Johnson, B., Eiser C., Young, V., Brierley, S., & Heller, S. (2012). Pre- valence of depression among young people with Type 1 diabetes: A systematic review. Diabetic Medici n e, Epub ahead of print. doi:10.1111/j.1464-5491.2012.03721.x Katon, W. J. (2003). Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biological Psychiatry, 54, 216-226. doi:10.1016/S0006-3223(03)00273-7 Katon, W., Von kroff, M., Ciechanowski, P., Russo, J., Lin, E., Simon, G., Ludman, E., Walker, E., Bush, T., & Young, B. (2004). Behav- ioural and clinical factors associated with depression among indi- viduals with diabetes. Diabetes Care, 27, 914-920. doi:10.2337/diacare.27.4.914 Katon, W. J., Von Korff, M., Lin, E. H. B., Simon, G., Ludman, E., Russo, J., Ciechanowski, P., Walker, E., & Bush, T. (2004). The pathways study. A randomized trial of collaborative care in Patients with diabetes and depression. Archives of General Psychiatry, 61, 1042-1049. doi:10.1001/archpsyc.61.10.1042 Katon, J. G., Russo, J., Gavin, A. R., Melville, J. L., & Katon, W. J. (2011). Diabetes and depression in pregnancy: Is there an association? Jour- nal of Women’s Health, 20, 983-989. doi:10.1089/jwh.2010.2662 Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005) Lifetime prevalence and age-of-onset distribu- tions of DSM-IV disorders in the national comorbidity survey repli- cation. Archives of g e ne r a l p s yc h ia t ry, 62, 593-602. doi:10.1001/archpsyc.62.6.593 Kivimäki, M., Batty, G. D., Jokela, M., Ebmeier, K. P., Vahtera, J., Vir- tanen, M., Brunner, E. J., Tabak, A. G., Witte, D. R., Kumari, M., Singh-Manoux, A., & Hamer, M. (2011). Antidepressant medication use and risk of hyperglycemia and diabetes mellitus—A noncausal association? Biologic a l Psychiatry, 70, 978-984. Knol, M. J., Twisk, J. W., Beekman, A. T., Heine, R. J., Snoek, F. J., & Pouwer, F. (2006). Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia, 49, 837-845. doi:10.1007/s00125-006-0159-x Kogan, S. M., Brody, G. H., Crawley, C., Logan, P., & Murry, V. M. (2007). Correlates of elevated depressive symptoms among rural Af- rican American adults with type 2 diabetes. Ethnicity & Disease, 17, 106-112. Korczak, D. J., Pereira, S., Koulajian, K., Matejcek, A., & Giacca, A. (2011). Type 1 diabetes mellitus and major depressive disorder: evi- dence for a biological link. Diabetologia, 54, 2483-2493. Kozhimannil, K. B., Pereira, M. A., & Harlow, B. L. (2009). Associa- tion between diabetes and perinatal depression among low-income mothers. Journal of the American Medical Association, 301, 842- 847. doi:10.1001/jama.2009.201 Levenson, J. L. (2001). Textbook of psychosomatic medicine. Arlington, VA: American Psychiatric Publishing, 193. Li, C., Ford, E. S., Strine, T. W., & Mokdad, A. H. (2008). Prevalence of depression among US adults with diabetes: findings from the 2006 behavioral risk factor surveillance system. Diabetes Care, 31, 105- 107. doi:10.2337/dc07-1154 Li, C., Ford, E. S., Zhao, G., Ahluwalia, I. B., Pearson, W. S., & Mok- dad, A. H. (2009). Prevalence and correlates of undiagnosed depres- sion among US adults with diabetes: The Behavioral Risk Factor Surveillance System. Diabetes Research and Clinical Practice, 83, 268-279. doi:10.1016/j.diabres.2008.11.006 Lustman, P. J., & Clouse, R. E (1997). Identifying depression in adults with diabetes. Clinical Diabetes, 15, 78-81. Ludman, E. J., Katon, W., Russo, J., Von Korff, M., Simon, G., Ciech- anowski, P., Lin, E., Bush, T., Walker, E., & Young, B. (2004). De- pression and diabetes symptom burden. General Hospital Psychiatry, 26, 430-436. doi:10.1016/j.genhosppsych.2004.08.010 Lustman, P. J., & Clouse, R. E. (2004). Section III: Practical Consid- erations in the management of depression in diabetes. Diabetes Spec- trum, 17, 160-166. doi:10.2337/diaspect.17.3.160 Lustman, P. J., Clouse, R. E., Ciechanowski, P. S., Hirsch, I. B., & Freedland, K. E. (2005). Depression-related hyperglycemia in type 1 diabetes: A mediational approach. Psychosomatic Medicine, 67, 195- 199. doi:10.1097/01.psy.0000155670.88919.ad Ma, Y., Balasubramanian, R., Pagoto, S. L., Schneider, K. L., Culver, A. L., Olendzki, B., Tinker, L., Liu, S., Safford, M., Sepavich, D. M., Rosal, M.C., Ockene, J. K., Carnethon, M., Zorn, M., & Hébert, J. R. (2011). Elevated depressive symptoms, antidepressant use, and dia- betes in a large multiethnic national sample of postmenopausal wo- Copyright © 2012 SciRes. 793  A. HEERAMUN-AUBEELUCK ET AL. Copyright © 2012 SciRes. 794 men. Diabetes Care, 34, 2390-2392. doi:10.2337/dc11-1223 McHale, M., Hendrikz, J., Dann, F., & Kenardy, J. (2008). Screening for depression in patients with diabetes mellitus. Psychosomatic Medi- cine, 70, 869-874. Mclntyre, R. S., Park, K. Y., Law, C. W. Y., Sultan, P., Adams, A., Lourenco, M. T., Lo, A. K. S., Soczynska, J. K., Woldeyohannes, H., Alsuwaidan, M., Yoor, J., & Kennedy, S. H. (2010). The association between conventional antidepressants and the metabolic syndrome. A Review of the evidence and clinical implications. CNS Drugs, 24, 741-763. doi:10.2165/11533280-000000000-00000 Mezuk, B., Eaton, W. W., Albrecht, S., & Golden, S. H. (2008). De- pression and type 2 diabetes over the lifespan: A meta-analysis. Dia- betes Care, 31, 2383-2390. doi:10.2337/dc08-0985 Moussavi, S., Chatterji, S., Verdes, E., Tandon, A., Patel, V., & Ustun, B. (2007). Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet, 370, 851-858. doi:10.1016/S0140-6736(07)61415-9 Murphy, S. L., Xu, J., & Kochanek, K. D. (2012). Deaths preliminary data for 2010. National Vital Statistics Reports, 60, 1-68. Musselman, D. L., Betan, E., Larsen, H., Phillips, L. S. (2003). Rela- tionship of depression to diabetes types 1 and 2: Epidemiology, bi- ology, and treatment. Biological Psychiatry, 54, 317-329. doi:10.1016/S0006-3223(03)00569-9 Pan, A., Lucas, M., Sun, Q., van Dam, R. M., Franco, O. H., Willett, W. C., Manson, J. E., Rexrode, K. M., Ascherio, A., & Hu, F. B. (2011). Increased mortality risk in women with depression and diabetes mel- litus. Archives of General Psychiatry, 68, 42-50. doi:10.1001/archgenpsychiatry.2010.176 Peveler, R., Carson, A., & Rodin, G. (2002). ABC of psychological medicine: Depression in medical patients. British Medical Journal, 325, 149-152. doi:10.1136/bmj.325.7356.149 Qaseem, A., Vijan, S., Snow, V., Cross, J. T., Weiss, K. B., & Owens, D. K. (Clinical Efficacy Assessment Subcommittee of the American College of Physicians) (2007). Glycemic control and type 2 diabetes mellitus: the optimal hemoglobin A1C targets. A guidance statement from the American College of Physicians. Annals of Internal Medi- cine, 147, 417-422. Rush, W. A., Whitebird, R. R., Rush, M. R., Solberg, L. I., & O’Conner, P. J. (2008). Depression in patients with diabetes: Does it impact clinical goals? Journal of the American Board Family Medicine, 21, 392-397. doi:10.3122/jabfm.2008.05.070101 Sayuk, G. S., Gott, B. M., Nix, B. D., & Lustman, P. J. (2011). Im- provement in sexual functioning in patients with type 2 diabetes and depression treated with bupropion. Diabetes Care, 34, 332-334. doi:10.2337/dc10-1714 The Diabetes Prevention Program Research Group (2004). Achieving weight and activity goals among Diabetes Prevention Program Life- style participants. Obesity Research, 12, 1426-1434. doi:10.1038/oby.2004.179 Tomlinson, M., Grimsrud, A. T., Stein, D. J., Williams, D. R., & Myer, L. (2009). The epidemiology of major depression in South Africa: Results from the South African stress and health study. South African Medical Journal, 99, 367-373. Ustun, T. B., Ayuso-Mateos, J. L., Chatterji, S., Mathers, C., & Murray, C. J. (2004). Global burden of depressive disorders in the year 2000. British Journal of P sychiatry, 184, 386-392. doi:10.1192/bjp.184.5.386 van der Feltz-Cornelis, C. M., Nuyen, J., Stoop, C., Chan, J., Jacobson, A. M., Katon, W., Snoek, F., & Sartorius, N. (2010). Effect of inter- ventions for major depressive disorder and significant depressive symptoms in patients with diabetes mellitus: A systematic review and meta-analysis. General Hospital Psychiatry, 32, 380-395. doi:10.1016/j.genhosppsych.2010.03.011 van der Feltz-Cornelis, C. M. (2011). Depression in diabetes mellitus: To screen or not to screen? A patient-centred approach. British Jour- nal of Diabetes & Vascular Disea s e , 11, 276-281. van Reedt Dortland, A. K. B., Giltay, E. J., van Veen, T., Zitman, F. G., & Penninx, B. W. J. H. (2010). Metabolic syndrome abnormalities are associated with severity of anxiety and depression and with tri- cyclic antidepressant use. Acta Psychiatrica Scandinavica, 122, 30-39. doi:10.1111/j.1600-0447.2010.01565.x Van Steenbergen-Weijenburg, K. M., de Vroege, L., Ploeger, R. R., Brals, J. W., Vloedbeld, M. G., Veneman, T. F., Hakkaart-van Roijen, L., Rut- ten, F. F., Beekman, A. T., & van der Feltz-Cornelis, C. M. (2010). Validation of the PHQ-9 as a screening instrument for depression in diabetes patients in specialized outpatient clinics. BMC Health Ser- vices Research, 12, 235. doi:10.1186/1472-6963-10-235 Wang, M. Y., Tsai, P. S., Chou, K. R., & Chen, C. M. (2008). A sys- tematic review of the efficacy of non-pharmacological treatments for depression on glycaemic control in type 2 diabetics. Journal of Clini- cal Nursing, 17, 2524-2530. doi:10.1111/j.1365-2702.2008.02301.x Wilkins T. L., & Sambamoorthi, U. (2011). Antidepressant use, depres- sion, lifestyle factors and new-onset diabetes. International Clinical Psychopharmacology, 26, 159-168. doi:10.1097/YIC.0b013e328342ce31 Williams, M. M., Clouse, R. E., & Lustman, P. J. (2006). Treating depression to prevent diabetes: Understanding depression as a medi- cal complication. Clinical Diabetes, 24, 79-86. doi:10.2337/diaclin.24.2.79 Willis, T. (1675). Pharmaceutice rationalis sive diabtriba demedica- mentorum operantionibus in humano corpore. Oxford: MDCLXXV. World Health Organization (2012). URL (last checked 22 July 2012). http://www.who.int/mental_health/management/depression/definitio n/en/ Zhao, W., Chen, Y., Lin, M., & Sigal, R. J. (2006). Association between diabetes and depression: Sex and age differences. Public Hea lt h, 120, 696-704. doi:10.1016/j.puhe.2006.04.012
|