 Psychology 2012. Vol.3, Special Issue, 775-781 Published Online September 2012 in SciRes (http://www.SciRP.org/journal/psych) http://dx.doi.org/10.4236/psych.2012.329117 Copyright © 2012 SciRes. 775 Acceptance of Disability among Chinese Individuals with Spinal Cord Injuries: The Effects of Social Support and Depression Jie Jiao, Mark M. Heyne, Chow S. Lam Department of Psychology, Illinois Institute of Technology, Chicago, USA Email: jjiao@iit.edu Received June 16th, 2012; revised July 17th, 2012; accepted August 10th, 2012 This study explored the roles of perceived social support and depression in acceptance of disability among Chinese individuals with spinal cord injuries (SCI). Design: An exploratory and cross-sectional study was conducted in an outpatient rehabilitation center in Guangzhou, China. One hundred Chinese individuals with SCI completed the Multidimensional Scale of Perceived Social Support, Center for Epidemiological Studies Short Depression Scale, and Acceptance of Disability Scale. Results: In general, there was low acceptance of disability and a high prevalence of depression among Chinese individuals with SCI. Higher acceptance of disability was associated with less depressive symptoms and higher level of perceived so- cial support. Furthermore, depression was shown to mediate the relationship between perceived social support and acceptance of disability. Conclusion: Depression is an essential factor in the process of ac- ceptance of disability. Cross-cultural studies are needed to facilitate a better understanding of the adjust- ment process following disabilities and apply culturally sensitive interventions to promote acceptance of disability. Keywords: Acceptance of Disability; Depression; Social Support; Spinal Cord Injuries; Chinese Introduction Among the myriad ways that adjustment to disability has been conceptualized and studied, the concept of acceptance of disability (AD) has received significant attention in the reha- bilitation literature. At its core, AD is considered to be a proc- ess of perceiving one’s disability as non-devaluing (Wright, 1983). To achieve this end, one must adjust his or her value system such that “actual or perceived losses from disability do not negatively affect the value of existing abilities” (Keaney & Glueckauf, 1993: p. 200). As a psychosocial variable, AD is one of the best indicators of positive adjustment following an acquired disability (Elliott, Uswatte, Lewis, & Palmatier, 2000) and has significant implications in vocational rehabilitation. Research has shown that AD facilitates employment and inde- pendent living (Green, Pratt, & Grigsby, 1984) and is signify- cantly associated with work status (Melamed, Groswasser, & Stern, 1992), social integration, and overall community integra- tion (Snead & Davis, 2002). There appear to be four specific value changes that charac- terize successful AD: enlargement of scope of values—the abil- ity to perceive value in abilities that have not been lost as a result of the disability; subordination of physique—the ability to evaluate self-worth based on nonphysical as well as physical attributes; containment of disability effects—the ability to view the disability itself as a single characteristic of oneself, but not the only characteristic; and transformation from comparative to asset values—the ability to recognize the value of one’s own unique combination of characteristics and abilities rather than making comparisons to an outside and often unattainable stan- dard (Wright, 1983). Assessment of these four core values has been shown to be a valid method of evaluating psychosocial adjustment following acquired physical disability (Elliott, Kurylo, & Rivera, 2002). The psychosocial variable that has perhaps the most consis- tent association with adjustment to disability in people with spinal cord injuries (SCI) is depression. Higher reported de- pressive symptomology has been related to lower adjustment in studies of varying sample sizes (Attawong & Kovindha, 2005; Elliott, 1999; Krause, Brotherton, Morrisette, Newman, & Karakostas, 2007; Martz, Livneh, Preibe, Wuermser, & Otto- manelli, 2005). The salient relationship between depression and AD in those years removed from the occurrence of SCI sup- ports the idea that AD encompasses more than one’s immediate emotional reaction to a physical disability. AD comprises cog- nitive and affective elements which interact to determine one’s adjustment to a chronic and disabling health condition. It may be that those with high AD are able to de-emphasize the impor- tance of physical attributes and place more value on their char- acterological attributes, leading to a sense of empowerment and a more positive outlook on their current situation; conversely, those with low AD may be preoccupied with the negative im- pact of their disability, leading to a sense of helplessness and leaving them more susceptible to prolonged and/or recurrent episodes of negative mood and experience. Social support has also been shown to be positively associ- ated with health, well-being, and coping with a stressful event such as SCI (Chronister, Johnson, & Berven, 2006). Some findings indicate that social support serves to buffer depression and suicidal intent, as well as enhance quality of life and life satisfaction (Beedie & Kennedy, 2002; Kemp & Krause, 1999). One of the characteristics of a collective culture such as China is the strong social support from family members and friends for those with disabilities (Morris & Peng, 1994; Yang, 1981). Having a strong social network and supportive relationships is particularly desirable for Chinese people (Triandis et al., 1986),  J. JIAO ET AL. and should serve to alleviate depression and facilitate adjust- ment to disability. A study by Belgrave (1991) found that social support was a significant predictor of AD among 170 African Americans with disabilities. Furthermore, Post and colleagues (1999) reported that there was a moderate to strong negative correlation be- tween social support and depression, and a positive correlation between social support and well-being, self-esteem, adjustment, and life satisfaction among people with SCI. Beedie and Ken- nedy (2002) followed a group of individuals with SCI longitu- dinally and found that high quality of social support was asso- ciated with lower hopelessness and depression scores, with this association becoming more pronounced as rehabilitation pro- gressed. Sherman, Devinney, and Sperling (2004) compared the impact of two types of social support, past peer-mentoring ex- perience (PME) and current live-in partner (LIP), on adjustment after SCI. They found that PME was associated with higher occupational activity and life satisfaction, while LIP was asso- ciated with greater mobility and economic self-sufficiency. These results attest the differential impacts of social support sources. The significance of social support on subjective well- being and quality of life has also been reported in other studies (Hampton, 2004; Hampton & Qin-Hilliard, 2004). In summary, people who report greater social support experience less emo- tional distress and better adjustment to their disabilities. Being the most populous country in the world, China also has the largest number of people with disabilities. Unlike the US, there is no official record of the incidence of SCI in China, though the number of individuals with SCI is expected to be high and on the rise given the increase in automobile and con- struction accidents (Hampton, 2001). To better understand how Chinese with SCI might differ from Westerners in their adjust- ment to disability, it is first necessary to know whether the Chinese differ from Westerners in their manifestation of de- pressive symptoms, as depression is the most consistent psy- chosocial correlate of SCI. Previous epidemiological studies have found the lifetime prevalence of depression to be between 3% and 17% in the United States (Kessler et al., 1994), but as low as .19% in China (Hwu, Chang, Yeh, Chang, & Yeh, 1996). One of the proposed reasons for this large discrepancy in de- pression prevalence is the more somatic presentation of psy- chological distress in the Chinese (Draguns, 1996), leading to medical diagnoses other than depression. The overall results of studies investigating symptom reporting in Chinese with de- pression suggest that the tendency of the Chinese to interpret putative symptoms of depression with a somatic explanation is stronger if they are less acculturated to a Western-style culture (Parker, Chan, Tully, & Eisenbruch, 2005; Yen, Robins, & Lin, 2000). Despite their significant relationship with each other, as well as with other psychosocial and disability-related factors, the effects of depression and social support on AD within the con- text of physical disability have not received much attention in non-Western samples. The correlates of AD in the Chinese may be somewhat different from those in U.S. samples, stemming from differing psychological reactions, differing social and physical environments, or differing cultural conceptualizations of disability. The more collectivist self-concept apparent in Eastern cultures suggests that long-term AD may be different in Chinese individuals with SCI, especially given the traumatic, chronic, and life-changing nature of this disability, and the more somatic orientation of symptom reporting among native Chinese. For this reason, the study of the association between AD, depression, and social support, which often being viewed as buffer to anxiety and depression, is necessary given the pau- city of research done with Chinese SCI population. The purpose of the current study was to explore the relationship between perceived social support, depression, and AD among Chinese individuals with SCI. It was hypothesized that both depression and social support would significantly predict AD. It was also hypothesized that high perceived social support would attenuate, or even nullify, the impact of depression on AD. In other words, we hypothesized that social support would serve as a mediator of the relationship between depression and AD. Method Participants The current study is part of a major collaborative project between the Guangdong Provincial Vocational Rehabilitation Center and the Illinois Institute of Technology’s (IIT) Reha- bilitation Psychology Program. Participants were patients re- ferred by their treating rehabilitation professionals at the reha- bilitation center, located in Guangzhou, China. To be included in the study, participants had to be at least 18 months post-SCI, as indicated by medical record or self-report. The justification for this inclusion criterion was to avoid the transient impact of the traumatic event related to the SCI and assess more stable and enduring cognitive and psychological constructs. Partici- pants had to be able to complete all instruments through face- to-face interview or phone interview. Exclusion criteria: Exclusion criteria included concomitant traumatic brain injury (TBI), developmental disabilities, or a history of hospitalization for a psychiatric disorder, as indicated by medical record. Those with TBI or a developmental disabil- ity were excluded to ensure that all participants could under- stand and complete study measures. Those with a history of psychiatric hospitalization were excluded to avoid the potential influence of a previous psychiatric condition on the psychoso- cial variables of interest in this study. Procedure: Two hundred twenty-five individuals were ini- tially identified from the rehabilitation center as possible par- ticipants for the study. Based on inclusion and exclusion criteria and willingness to participate, the final sample consisted of 100 in and outpatients. The age range of the participants was from 19 to 77 (Mean = 37.68, SD = 11.77) and 37 percent of the participants had some college education. At the time of the study, more than 70 percent of the participants were married and less than half of the participants were working (full time = 31%; part time = 7%; home maker = 3%; student = 2%). Each participant was paid 30 RMB ($4.50) for their interview. Inter- views took place either in person or by phone; in-person inter- views lasted approximately 40 minutes and phone interviews lasted 60 - 80 minutes. All interviews were conducted by a physician or graduate research assistant trained in the admini- stration of all measures. Prior to study participation, all partici- pants provided written or verbal informed consent. Data were collected from January 2007 through December 2008. Measures Demographics and injury-related characteristics: Demo- graphic information was collected on gender, age, marital status, education level, and work status. Work status was classified Copyright © 2012 SciRes. 776  J. JIAO ET AL. into one of six categories: full-time; part-time; student; retired; homemaker; unemployed. Type of injury was determined by neurologic level and the extent of lesion; injuries were classi- fied as either tetraplegia or paraplegia based on diagnosis indi- cated in the medical record or self-report. Acceptance of disability: Acceptance of Disability Scale (ADS; Linkowski, 1971) is a 50-item measure examining psy- chosocial adjustment among people with disabilities. The scale evaluates the degree to which people find meaning in their cir- cumstances and maintain positive beliefs about themselves. Participants rate each item on a 6-point scale ranging from 1 (disagree very much) to 6 (agree very much), with 15 of the items reverse scored. Higher scores indicate greater acceptance of disability. The scale demonstrates high reliability, with an internal consistency coefficient of .93, and significant construct and concurrent validity (Linkowski, 1971). The Chinese ver- sion of the ADS (Wu & Lu, 1999) has been translated and back-translated, and it has been found to be appropriate for use with a Taiwanese sample. Depression: Center for Epidemiologic Studies Short De- pression Scale (CES-D 10; Andresen, Malmgren, Carter, & Patrick, 1994) is a 10-item self-report measure designed to as- sess symptoms of depression in the general population. The full-length 20-item version of the CES-D (Radloff, 1977) was designed to de-emphasize somatic complaints relative to other depression scales, and the CES-D 10 is a shorter version of this instrument. Considering the substantial medical complications related to SCI, the CES-D 10 helps to avoid the problem of over-diagnosing depression based on somatic symptoms. Par- ticipants are instructed to rate items on a 4-point scale ranging from 0 (rarely or none of the time) to 3 (all of the time), with 2 items reverse scored; a higher score indicates higher depressive symptoms. When compared to the 20-item version of the CES- D, the CES-D 10 has demonstrated strong predictive accuracy (kappa = .97), and test-retest reliability is comparable to that of other measures of depression (r = .71) (Andresen et al., 1994). Internal consistency reliability in a sample of patients with chronic disease was .84 (Lorig, Sobel, Ritter, Laurent, & Hobbs, 2001.) The CES-D has been widely used in various cultures, and it has specifically demonstrated construct validity within a sample of Chinese married couples (Cheung & Bagley, 1998). Social support: Multidimensional Scale of Perceived Social Support (MSPSS; Zimet, Dahlem, Zimet, & Farley, 1988) is a 12-item self-report measure of the perceived level of support from three sources: family, friends, and significant other. Par- ticipants rate items on a 7-point scale ranging from 1 (very strongly disagree) to 7 (very strongly agree), with higher scores indicating a higher level of perceived social support. The MSPSS has demonstrated very good internal reliability, with Cronbach’s alpha ranging from .85 - .91 (Dahlem, Zimet, & Walker, 1991; Zimet et al., 1988). The measure has also shown construct validity, as evidenced by its negative association with measures of anxiety and depression (Zimet et al., 1988), and factorial validity, as factor analysis confirms that individuals do make distinctions between sources of social support (Dahlem et al., 1991). The Chinese version of the MSPSS has shown good internal consistency as well, ranging from .82 to .94 (Chou, 2000; Short & Johnston, 1997; Zhang & Norvilitis, 2002). Statistical Analysis To examine the relationship among perceived social support, depression, and AD, bivariate correlation was utilized. Given that little research has been done among the Chinese population, associations of demographic variables (i.e., age, gender, educa- tion) with these psychosocial variables were also examined through correlational analysis. Hierarchical regression analysis was used to evaluate the independent contributions of depress- sion and perceived social support to AD. Because this was a pilot study concerning AD within the Chinese population, demographic variables were entered in the first block of the regression model. Total score on the perceived social support scale (MSPSS) was entered in the second block given its crucial impact in Chinese culture. Total score on the depression scale (CES-D 10) was entered in the model last to reveal its unique contribution to AD with all other variables controlled. The po- tential mediating role of social support in the relationship be- tween depression and AD was tested following the procedure recommended by Judd and Kenny (1981, as cited in Baron & Kenny, 1986). Results Preliminary and Correlational Analyses Means and standard deviations of the sample’s scores on the MSPSS, CES-D 10, and ADS are provided in Table 1. Of note, approximately 67 percent of participants met the criterion for depression using the CES-D 10 cut-off score of 10 suggested by Andresen et al. (1994). After dichotomizing the sample using the above criterion (depressed vs. non-depressed), it was found that the individuals in the depressed group re- ported a significantly lower level of perceived social support (t = 4.44, p < .01) and acceptance of disability (t = 4.59, p < .01) than those in the non-depressed group. The average total score on the MSPSS was 60 and 71, respectively; the average total score on the ADS was 172 and 198, respectively. Bivariate correlation analyses showed that there were no sig- nificant correlations between the demographic variables and the MSPSS score. Similarly, only education was significantly re- lated to CES-D 10 score (r = –.20, p < .05), with people with higher education reporting less depressive symptoms. For the ADS, all three demographic variables showed a significant bivariate correlation with the ADS score. Female gender was associated with higher AD (r = .24, p < .05). Age was nega- tively related to their ADS score (r = –.22, p < .05), and educa- tion level was positively associated with the ADS score (r = .34, p < .01). Of interest, for the sample as a whole, age was nega- tively associated with education level (r = –.33, p < .01). After controlling for education, the relationship between age and the ADS score became non-significant. There were significant correlations among the ADS score, CES-D 10 score, and MSPSS score. The ADS score was nega- tively correlated with the CES-D 10 score (r = –.57, p < .01) and positively correlated with the MSPSS score (r = .28, p < .01). The MSPSS score was also negatively correlated with the Table 1. Means ans standard deviations of scores on perceived social support, depression and acceptance of disability measures for the entire sample. Measure M SD n MSPSS 63.81 12.86 99 CES-D 1011.44 5.44 99 ADS 182.18 29.80 94 Copyright © 2012 SciRes. 777 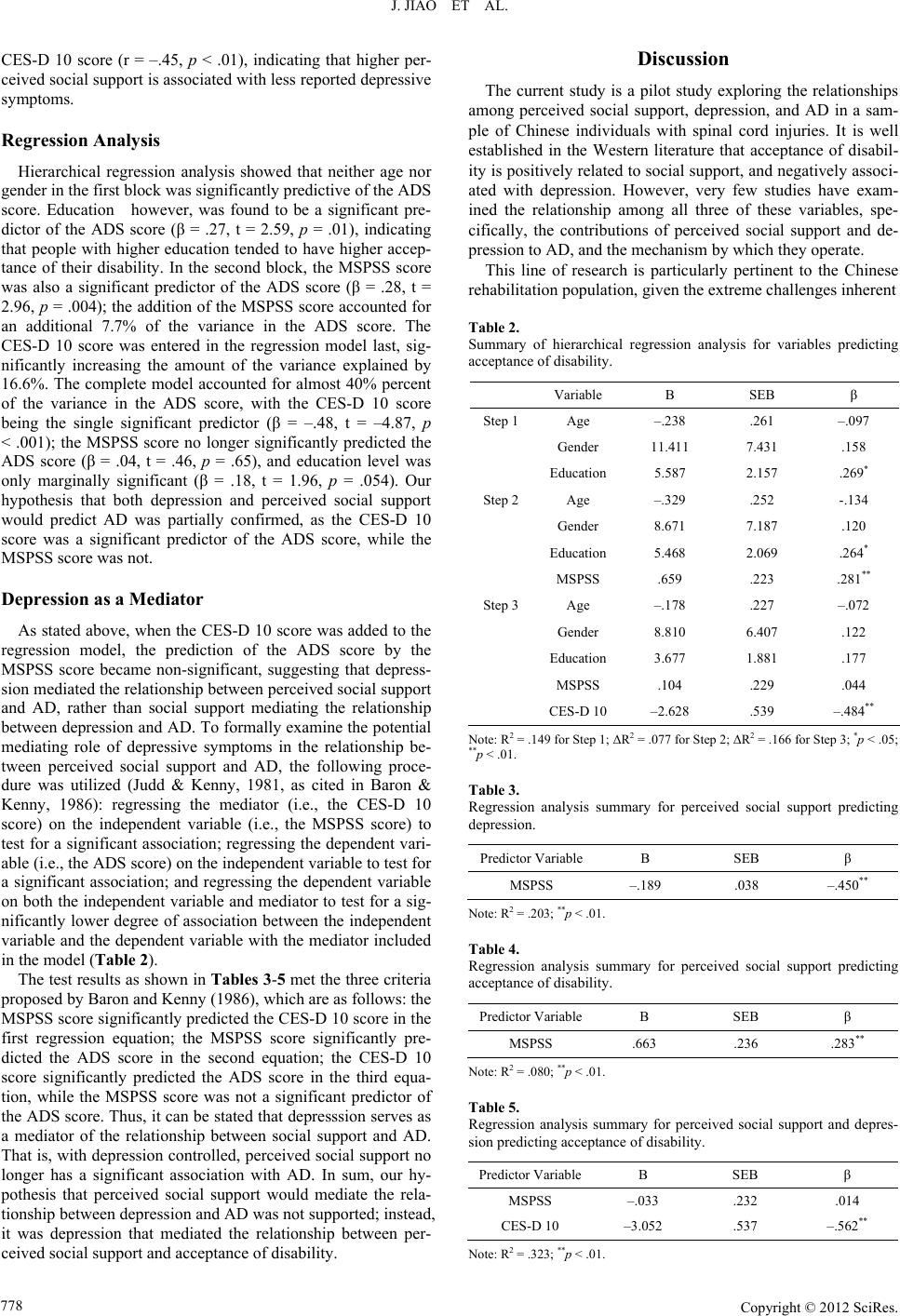 J. JIAO ET AL. CES-D 10 score (r = –.45, p < .01), indicating that higher per- ceived social support is associated with less reported depressive symptoms. Regression Analysis Hierarchical regression analysis showed that neither age nor gender in the first block was significantly predictive of the ADS score. Education however, was found to be a significant pre- dictor of the ADS score (β = .27, t = 2.59, p = .01), indicating that people with higher education tended to have higher accep- tance of their disability. In the second block, the MSPSS score was also a significant predictor of the ADS score (β = .28, t = 2.96, p = .004); the addition of the MSPSS score accounted for an additional 7.7% of the variance in the ADS score. The CES-D 10 score was entered in the regression model last, sig- nificantly increasing the amount of the variance explained by 16.6%. The complete model accounted for almost 40% percent of the variance in the ADS score, with the CES-D 10 score being the single significant predictor (β = –.48, t = –4.87, p < .001); the MSPSS score no longer significantly predicted the ADS score (β = .04, t = .46, p = .65), and education level was only marginally significant (β = .18, t = 1.96, p = .054). Our hypothesis that both depression and perceived social support would predict AD was partially confirmed, as the CES-D 10 score was a significant predictor of the ADS score, while the MSPSS score was not. Depression as a M ediator As stated above, when the CES-D 10 score was added to the regression model, the prediction of the ADS score by the MSPSS score became non-significant, suggesting that depress- sion mediated the relationship between perceived social support and AD, rather than social support mediating the relationship between depression and AD. To formally examine the potential mediating role of depressive symptoms in the relationship be- tween perceived social support and AD, the following proce- dure was utilized (Judd & Kenny, 1981, as cited in Baron & Kenny, 1986): regressing the mediator (i.e., the CES-D 10 score) on the independent variable (i.e., the MSPSS score) to test for a significant association; regressing the dependent vari- able (i.e., the ADS score) on the independent variable to test for a significant association; and regressing the dependent variable on both the independent variable and mediator to test for a sig- nificantly lower degree of association between the independent variable and the dependent variable with the mediator included in the model (Table 2). The test results as shown in Tables 3-5 met the three criteria proposed by Baron and Kenny (1986), which are as follows: the MSPSS score significantly predicted the CES-D 10 score in the first regression equation; the MSPSS score significantly pre- dicted the ADS score in the second equation; the CES-D 10 score significantly predicted the ADS score in the third equa- tion, while the MSPSS score was not a significant predictor of the ADS score. Thus, it can be stated that depresssion serves as a mediator of the relationship between social support and AD. That is, with depression controlled, perceived social support no longer has a significant association with AD. In sum, our hy- pothesis that perceived social support would mediate the rela- tionship between depression and AD was not supported; instead, it was depression that mediated the relationship between per- ceived social support and acceptance of disability. Discussion The current study is a pilot study exploring the relationships among perceived social support, depression, and AD in a sam- ple of Chinese individuals with spinal cord injuries. It is well established in the Western literature that acceptance of disabil- ity is positively related to social support, and negatively associ- ated with depression. However, very few studies have exam- ined the relationship among all three of these variables, spe- cifically, the contributions of perceived social support and de- pression to AD, and the mechanism by which they operate. This line of research is particularly pertinent to the Chinese rehabilitation population, given the extreme challenges inherent Table 2. Summary of hierarchical regression analysis for variables predicting acceptance of disability. Variable B SEB β Step 1Age –.238 .261 –.097 Gender 11.411 7.431 .158 Education 5.587 2.157 .269* Step 2Age –.329 .252 -.134 Gender 8.671 7.187 .120 Education 5.468 2.069 .264* MSPSS .659 .223 .281** Step 3Age –.178 .227 –.072 Gender 8.810 6.407 .122 Education 3.677 1.881 .177 MSPSS .104 .229 .044 CES-D 10 –2.628 .539 –.484** Note: R2 = .149 for Step 1; ΔR2 = .077 for Step 2; ΔR2 = .166 for Step 3; *p < .05; **p < .01. Table 3. Regression analysis summary for perceived social support predicting depression. Predictor VariableB SEB β MSPSS –.189 .038 –.450** Note: R2 = .203; **p < .01. Table 4. Regression analysis summary for perceived social support predicting acceptance of disability. Predictor VariableB SEB β MSPSS .663 .236 .283** Note: R2 = .080; **p < .01. Table 5. Regression analysis summary for perceived social support and depres- sion predicting acceptance of disability. Predictor VariableB SEB β MSPSS –.033 .232 .014 CES-D 10 –3.052 .537 –.562** Note: R2 = .323; **p < .01. Copyright © 2012 SciRes. 778  J. JIAO ET AL. in AD and the increased cultural emphasis on social support. This study focused on the population of Chinese individuals with SCI because of the increased rate of injury and the trau- matic impact on the individuals and their families. SCI has been studied extensively in the Western literature because of its tre- mendous impact on rehabilitation resources. In developing China, rehabilitation services are still limited in scope, and optimizing rehabilitation outcome using available resources is the main focus of Chinese rehabilitation professionals. Addi- tionally, a better understanding of the adjustment process of Chinese individuals with SCI will fill an existing gap in the rehabilitation literature and help develop cultural competency among Western rehabilitation professionals. Results showed that, as a whole, participants reported a low level of acceptance of disability; the mean ADS score in this sample was 182, whereas in a Western sample of rehabilitation clients a mean ADS score of 217 has been reported, with scores of 180 and below being considered indicative of low AD (Jointer, Lovett, & Goodwin, 1989). Compared with their West- ern counterparts, this Chinese sample demonstrated a lower level of AD. In terms of depressive symptoms, the mean CES-D 10 score was 11, with more than 60 percent of partici- pants meeting the criterion for depression using the suggested cut-off score of 10 reported by Andresen et al. (1994). This level of depressive symptomology is much higher than that re- ported in the Western rehabilitation literature (Richards, Kew- man, & Pierce, 2000). Due to the physical complaints com- monly reported by individuals with SCI, this study used the CES-D 10 to prevent over-diagnosing depression in this popu- lation based on somatic symptoms. Thus, we believe that this result accurately reflects the depression prevalence among Chinese individuals with SCI, as somatic symptoms have been controlled by the depression measure chosen. It should be noted that the participants in this study were at least a year-and-a-half post-injury. Based on our findings and methodology, we are confident that those met the criterion for depression were not experiencing inflated symptomology due to very recent onset of injury or a preponderance of somatic symptoms. We believe that our findings are an accurate reflection of the significantly lower level of perceived social support and acceptance of dis- ability in those with higher depressive symptomatology. The present study confirmed the findings reported in the Western literature that female individuals are more accepting of their disability. In addition, education was positively associated with AD. Consistent with previous research, age did not dem- onstrate a significant association with AD. As for the relation- ship between perceived social support, depression, and AD, our results replicated existing findings in the literature (Attawang & Kovindha, 2005; Belgrave, 1991; Perry, Nicholas, & Middleton, 2009; Post et al., 1991): perceived social support was shown to be positively associated with AD and negatively associated with depression; depression and AD were negatively associ- ated. By way of hierarchical regression analysis, the prediction of AD by perceived social support and depression was examined. In the regression model, education was the single significant demographic predictor of AD, with higher education contribut- ing to higher AD. Perceived social support was added in the second block of the model, and depression was added in the third and final block. For the overall regression equation, de- pression was the single significant predictor of AD. Surpris- ingly, perceived social support was no longer a significant pre- dictor after depression was added into the regression model. The non-significant role of perceived social support in the final model was unexpected, given the seeming importance of social support to well-being cited in the Chinese literature (Chan, Lee, & Lieh-Mak, 2000). Results indicated that per- ceived social support did not have a direct effect on AD, nor did it impact the relationship between depression and AD. In- stead, depression mediated the relationship between perceived social support and AD. In other words, depression appears to be the generative mechanism through which perceived social sup- port influences AD. That is, depression seems to be the essen- tial factor in the process of acceptance of disability. Due to the drastic life changes resulting from their disability, Chinese individuals with SCI are likely to be sensitive to the negative impact on their social network, which can induce substantial guilt and self-blame. Furthermore, their collectivist cultural up- bringing dictates that Chinese individuals seek out and require feedback from their family and friends to establish their self- concept. So low perceived social support can be especially detrimental. This low level of perceived social support may exacerbate already existing adjustment difficulties and make these individuals more vulnerable to developing psychological problems such as depression. The results of the present study indicate that depression is prevalent among Chinese individuals with SCI, and it has a marked impact on the process of accep- tance of disability. The most significant finding of this study is the essential role of depression in the relationship between perceived social sup- port and acceptance of disability. Rather than being mediated by social support, depression mediates the relationship between social support and acceptance of disability, having a pervasive and direct impact throughout the adjustment process. For social support to facilitate acceptance of disability, it must operate by mitigating individuals’ depressive symptoms. One explanation for this finding is that Chinese individuals with SCI are par- ticularly vulnerable to depression as the result of their disabling condition. More than 60 percent of the participants in this study met the CES-D 10 criterion for depression (Andresen et al., 1994), and this prevalence is higher than that documented in the Western literature (Richards et al., 2000). Another possible explanation for only the indirect impact of social support may be that those with SCI need social support aside from family, friends, and significant others, as measured by the social sup- port scale used in this study. Subsequent studies should invest- tigate whether support from rehabilitation professionals or peo- ple with similar conditions plays a more direct role in the ad- justment process. The current study holds important implications. Given its pervasive and direct impact on the rehabilitation process, de- pression should be carefully assessed and closely monitored in Chinese individuals with SCI. When working with these indi- viduals, rehabilitation professionals should pay close attention to both presenting somatic symptoms and emotional function- ing, as this population appears to be at significant risk for de- pression. Additionally, though social support is likely an im- portant factor in adjustment to disability, it is not a panacea. It is often assumed that as long as individuals with SCI have support from their family and friends, they will make a smooth adjustment to their disability. This is especially believed to be true for those from a collectivist cultural background such as the Chinese. Rehabilitation professionals need to guard against the tendency to oversimplify and generalize the rehabilitation Copyright © 2012 SciRes. 779  J. JIAO ET AL. process of people from different cultural backgrounds. Finally, the results of the present study do not undermine the impor- tance of social support. Instead, it suggests that the conceptu- alization of social support and its measurement be broadened (e.g., interaction with rehabilitation professional, interaction with people with similar condition), both in research and prac- tice, to further examine and utilize its contribution to adjust- ment to disability. Limitation The present study has several limitations. First, we used a convenient sample, and participants had been receiving outpa- tient rehabilitation services which are not commonly accessible for the majority of Chinese individuals with disabilities. Also, approximately 37 percent of the participants had some college education, which is higher than the level of education reported in the general population. These factors may limit the gener- alizability of the current findings to the larger population of Chinese individuals with SCI. Second, ours was the first study to use the ADS scale with Chinese individuals from mainland China. Studies examining the reliability and validity of this scale for this particular population are needed. Third, as dis- cussed previously, the social support scale used in this study focuses mainly on support from family, friends, and significant others. The scale does not include social support from other resources. For example, it does not include perceived support from professionals or people with similar conditions, which might partially account for the non-significant prediction of acceptance of disability by perceived social support. Future studies on acceptance of disability, social support, and depress- sion would benefit from the inclusion of a broader range of de- mographic, disability-related, and psychosocial variables, such as employment status, marital status, functional limitations, and self-efficacy. The interaction among these variables could shed further light on this important rehabilitation topic. Conclusion In summary, the results of the present study indicate that the prevalence of depression is alarmingly high among Chinese individuals with SCI. Depression is negatively associated with perceived social support, and is predictive of lower acceptance of disability. Depression is an essential factor in the adjustment process, and it mediates the relationship between social support and acceptance of disability. Further research is needed to con- tinue investigating the effects of depression and perceived so- cial support on acceptance of disability in populations from different cultures. Cross-cultural studies will help rehabilitation professionals develop a better understanding of the adjustment process and apply effective and culturally sensitive intervene- tions to promote acceptance of disability. REFERENCES Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). American Journal of Preventive Medicine, 10, 77-84. Attawong, T., & Kovindha, A. (2005). The influencing factors of ac- ceptance of disability in spinal cord injured patients. Nepal Journal of Neuroscience, 2, 67-70. Baron, R. M, & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psy- chology, 51, 1173-1182. doi:10.1037/0022-3514.51.6.1173 Beedie, A., & Kennedy, P. (2002). Quality of social support predicts hopelessness and depression post spinal cord injury. Journal of Clinical Psychology in M edical Settings, 9, 227-234. doi:10.1023/A:1016003428370 Belgrave, F. Z. (1991). Psychosocial predictors of adjustment to dis- ability in African Americans. Journal of Rehabilitation, 57, 37-40. Chan, R. C. K., Lee, P. W. H, & Lieh-Mark, F. (2000). The pattern of coping in persons with spinal cord injuries. Disability and Rehabil- itation, 22, 501-507. doi:10.1023/A:1016003428370 Cheung, C. K., & Bagley, C. (1998). Validating an American scale in Hong Kong: The Center for Epidemiological Studies Depression Scale (CES-D). The Journal of Psychology, 132, 169-186. doi:10.1080/00223989809599157 Chou, K. L. (2000). Assessing Chinese adolescents’ social support: The multidimensional scale of perceived social support. Personality and Individual Differences, 28, 299-307. doi:10.1016/S0191-8869(99)00098-7 Chronister, J. A., Johnson, E. K., & Berven, N. (2006). Measuring social support in rehabilitation. Disability and Rehabilitation, 28, 75- 84. doi:10.1016/S0191-8869(99)00098-7 Dahlem, N. W., Zimet, G. D., & Walker, R. (1991). The multimensional scale of perceived social support: A conformation study. Journal of Clinical Psychology, 4 7, 756-761. doi:10.1002/1097-4679(199111)47:6<756::AID-JCLP2270470605>3 .0.CO;2-L Draguns, J. G. (1996). Abnormal behaviour in Chinese societies: Clini- cal, epidemiological, and comparative studies. In M. H. Bond (Ed.), Handbook of Chinese psychology (pp. 412-428). Hong Kong: Oxford University Press. Elliott, T. R. (1999). Social problem-solving abilities and adjustment to recent-onset spinal cord injury. Rehabilitation Psychology, 44, 315- 332. doi:10.1037/0090-5550.44.4.315 Elliott, T. R., Kurylo, M., & Rivera, P. (2002). Positive growth follow- ing acquired physical disability. In C. R. Snyder & S. J. Lopez (Eds.), Handbook of positive psychology (pp. 687-699). New York: Oxford University Press. Elliott, T. R., Uswatte, G., Lewis, L., & Palmatier, A. (2000). Goal in- stability and adjustment to physical disability. Journal of Counseling Psychology, 47, 251-265. doi:10.1037/0022-0167.47.2.251 Green, B., Pratt, C., & Grigsby, T. (1984). Self-concept among persons with long-term spinal cord injury. Archives of Physical Medicine and Rehabilitation, 65, 751-754. Hampton, N. Z. (2001). Disability status, perceived health, social sup- port, self-efficacy, and quality of life among people with spinal cord injury in the People’s Republic of China. International Journal of Rehabilitation Research, 24, 69-71. doi:10.1097/00004356-200103000-00010 Hampton, N. Z. (2004). Subjective well-being among people with spi- nal cord injuries: The role of self-efficacy, perceived social support, and perceived health. Rehabilitation Counseling B u l l e t i n , 4 8 , 31-37. doi:10.1177/00343552040480010401 Hampton, N. Z., & Qin-Hilliard, D. B. (2004). Dimensions of quality of life for Chinese Adults with spinal cord injury: A qualitative study. Disability and Rehabilitation, 26, 203-212. doi:10.1080/09638280310001639704 Hwu, H. G., Chang, I. H., Yeh, E. K., Chang, C. J., & Yeh, L. L. (1996). Major depressive disorder in Taiwan defined by the Chinese Diag- nostic Interview Schedule. Journal of Nervous and Mental Disease, 184, 497-502. doi:10.1080/09638280310001639704 Joiner, J. G., Lovett, P. S., & Goodwin, L. K. (1989). Positive assertion and acceptance among persons with disabilities. Journal of Reha- bilitation, 2, 22-29. Keaney, K. C. M. H., & Glueckauf, R. L. (1993). Disability and value change: An overview and reanalysis of acceptance of loss theory. Rehabilitation Psychology, 38, 199-210. doi:10.1037/h0080297 Kemp, B. J, & Krause, J. S. (1999). Depression and life satisfaction among people ageing with post-polio and spinal cord injury. Disabil- ity and Rehabilitation, 2 1 , 241-249. Copyright © 2012 SciRes. 780  J. JIAO ET AL. Copyright © 2012 SciRes. 781 doi:10.1080/096382899297666 Kendall, E., & Buys, N. (1998). An integrated model of psychosocial adjustment following acquired disability. Journal of Rehabilitation, 64, 16-20. Kessler, R. C., McGonagle, K. A., Zhao, S., Nelson, C. B., Hughes, M., Eshleman, S., Wittchen, H., Kendler, K. S. (1994). Lifetime and 12- month prevalence of DSM-III-R psychiatric disorders in the United States. Archives of General Psychiatry, 51, 8-19. doi:10.1001/archpsyc.1994.03950010008002 Krause, J. S., Brotherton, S. S., Morrisette, D. C., Newman, S. D., & Karakostas, T. E. (2007). Does pain interference mediate the rela- tionship of independence in ambulation with depressive symptoms after spinal cord injury? Rehabilitation Psychology, 52, 162-169. doi:10.1037/0090-5550.52.2.162 Linkowski, D. (1971). A scale to measure acceptance of disability. Re- habilitation Counseling Bulletin, 14, 236-244. Lorig K. R., Sobel, D. S., Ritter P. L., Laurent, D., & Hobbs, M. (2001). Effects of a self- management program for patients with chronic dis- ease. Effective Clinical Practice, 4, 256-262. Martz, E., Livneh, H., Preibe, M., Wuermser, L. A., & Ottomanelli, L. (2005). Predictors of psychosocial adaptation among people with spinal cord injury or disorder. Archives of Physical Medicine and Rehabilitation, 86, 1182-1192. doi:10.1016/j.apmr.2004.11.036 Melamed, S., Groswasser, Z., & Stern, M. J. (1992). Acceptance of disability, work involvement and subjective rehabilitation status of traumatic brain-injured (TBI) patients. Brain Injury, 6, 233-243. doi:10.3109/02699059209029665 Morris, M. W., & Peng, K. (1994). Culture and cause: American and Chinese attributions for social and physical events. Journal of Per- sonality and Social P sychology, 67, 949-971. doi:10.1037/0022-3514.67.6.949 Parker, G., Chan, B., Tully, L., & Eisenbruch, M. (2005). Depression in the Chinese: The impact of acculturation. Psychological Medicine, 35, 1475-1483. doi:10.1017/S0033291705005623 Perry, K. N., Nicholas, M. K., & Middleton, J. (2009). Spinal cord injury-related pain in rehabilitation: A cross-sectional study of rela- tionship with cognition, mood and physical function. European Jour- nal of Pain, 13, 511-517. doi:10.1016/j.ejpain.2008.06.003 Post, M. W. M., Ros, W. J. G, & Schrijvers, A. J. P. (1999). Impact of social support of health status and life satisfaction in people with spinal cord injury. Psychology and Health, 14, 679-695. doi:10.1080/08870449908410757 Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Meas- urement, 1, 385-401. doi:10.1177/014662167700100306 Richards, J. S., Kewman, D. G., & Pierce, C. A. (2000). Spinal cord in- jury. In F. G. Frank & T. R. Elliott (Eds.), Handbook of Rehabilita- tion Psychology (pp. 11-27). Washington, DC: American Psycho- logical Association. doi:10.1037/10361-001 Sherman, J. E., DeVinney, D. J., & Sperling, K. B. (2004). Social sup- port and adjustment after spinal cord injury: Influence of past peer- mentoring experiences and current live-in partner. Rehabilitation Psychology, 49, 140-149. doi:10.1037/0090-5550.49.2.140 Short, K. H., & Johnston, C. (1997). Stress, maternal distress, and chil- dren’s adjustment following immigration: The buffering role of so- cial support. Journal of Consulting and Clinical Psychology, 65, 494-503. doi:10.1037/0022-006X.65.3.494 Snead, S. L., & Davis, J. R. (2002). Attitudes of individuals with ac- quired brain injury towards disability. B rain Injury, 16, 947-953. doi:10.1080/02699050210147211 Triandis, H. C., Bontempo, R., Betancourt, H., Bond, M., Leung, K., Brenes, A., Georgas, J., Hui, C. H., Martin, G., Setiadi, B., Sinha, J., Verma, J., Spangenberg, J., Touzard, H. & Montmollin, G. (1986). The measurement of the etic aspects of individualism and collectiv- ism across cultures. Australian Journal of Psychology, 38 , 257-267. doi:10.1080/00049538608259013 Wright, B. A. (1983). Physical disability: A psychosocial approach (2nd ed.). New York: Harper & Row. doi:10.1037/10589-000 Wu, W. D., & Lu, T. H. (1999). The Chinese translated version of ac- ceptance of disability scale. Taipei: National Taiwan Normal Uni- versity. Yang, K. S. (1981). Social orientation and individual modernity among Chinese students in Taiwan. Journal of Social Psychology, 113, 159- 170. doi:10.1080/00224545.1981.9924368 Yen, S., Robins, C. J., & Lin, N. (2000). A cross-cultural comparison of depressive symptom manifestation: China and the United States. Journal of Consulting and Clin ic al Psychology, 68, 993-999. doi:10.1037/0022-006X.68.6.993 Zhang, J., & Norvilitis J. M. (2002). Measuring Chinese psychological well-being with western developed instruments. Journal of Personal- ity Assessment, 79, 492-511. doi:10.1207/S15327752JPA7903_06 Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The Multidimensional Scale of Perceived Social Support. Journal of Per- sonality Assessment, 52, 30-41. doi:10.1207/s15327752jpa5201_2
|