Open Journal of Nephrology, 2012, 2, 35-37
http://dx.doi.org/10.4236/ojneph.2012.23006 Published Online September 2012 (http://www.SciRP.org/journal/ojneph)
Patient with Churg Strauss Syndrome and Myocarditis
Treated with Cyclophosphamide
Liam Mullen, Janice Harper, Sukumaran Binukrishnan
Royal Liverpool University Hospital, Liverpool Heart an d Chest Hospital, Liverpool, UK
Email: Liam.Mullen@nhs.net
Received April 5, 2012; revised May 25, 2012; accepted June 10, 2012
ABSTRACT
Cardiac involvement in Churg Strauss Syndrome is common and a poor prognostic indicator. Myocarditis in Churg
Strauss Syndrome can present in different ways. It has been shown that basic cardiac investigations including echocar-
diography can be normal even in symptomatic patients. More recently cardiac magnetic resonance imaging (MRI) has
been shown to be more sensitive in its diagno sis. Our case report describes a 45 year old male who presented with pal-
pitations and breathlessness. Echocardiography was normal but cardiac MRI demonstrated abnormalities consistent
with Myocarditis. He was treated with Cyclophosphamide and follow up MRI imaging demonstrated complete resolu-
tion of these abnormalities which was accompanied by resolution of symptoms. This case therefore supports the use of
cardiac MRI in Churg Strauss Synd rome as a sensitiv e diag nostic too l and as a means of monito ring respon se to therapy.
It also supports the therapeutic effectiveness of Cyclophosphamide therapy in Churg Strauss related Myocarditis,
something that has yet to be assessed on a large scale.
Keywords: Cardiac MRI; Cyclophosphamide; Myocarditis; Churg Strauss Syndrome
1. Introduction
Cardiac involvement in Churg Strauss Syndrome is
common, with a prevalence of up to 62% [1]. It is the
leading cause of mortality in this disease [2]. The necro-
tising granulomatous Myocarditis associated with Churg
Strauss can manifest in different ways. Clear diagnosis is
difficult without myocardial biopsy. Unlik e patients with
renal disease, patients with cardiac involvement are usu-
ally ANCA (perinuclear type) negative [3,4]. Further-
more traditional cardiac investigations including echo-
cardiography can be normal even in symptomatic pa-
tients. More recently cardiac MRI has been proposed as a
useful diagnostic and monitoring tool in this condition.
Here we present a case of Churg Strauss Myocarditis in
which cardiac MRI was utilised to good effect.
2. Case Report and Methods
A 45 year old man, recently diagnosed with Churg Strauss
Syndrome, presented with a two week history of palpita-
tions, presyn cope and breathlessness on exertio n. He had
been taking Prednisolone since 1999 when he had been
initially diagnosed with chronic eosinophilic pneumonia,
and was currently prescribed 30mg daily.
He was admitted in January 2010 for investigation of
his symptoms. Electrocardiography and serum Troponin
T were normal. A 24 hour tape showed sinus rhythm with
22 isolated ventricular ectopics and 962 episodes of ven-
tricular bigeminy. An echocardiogram demonstrated
normal biventricular size and function, and no significant
abnormalities.
He was incidentally prescribed Myfortic (Mycopheno-
lic Acid) 720 mg twice a day in February 2010, in addi-
tion to Prednisolone, on the basis of persistent sinus
symptoms.
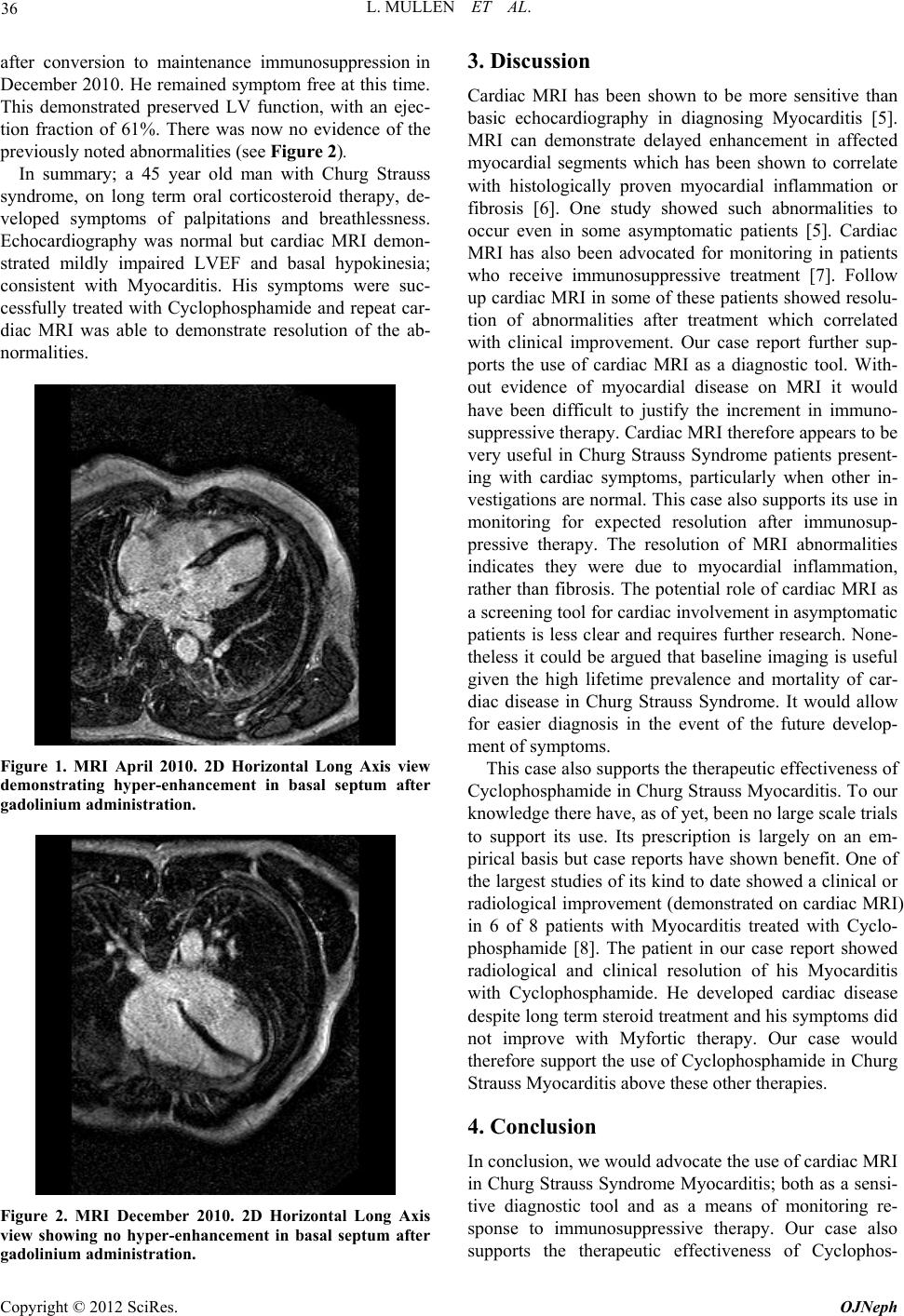
Based on his ongoing cardiac symptoms he subse-
quently underwent cardiac MRI in April. This demon-
strated a mildly reduced left ventricular ejection fraction
(LVEF) of 46%. There was mild hypo kinesia of the basal
septum with late contrast hyper-enhancement; consistent
with Myocarditis (see Figure 1). There was no evidence
of endocardial disease or myocardial hypert r op hy .
Based on the MRI findings he was commenced on
Cyclophosphamide in May and Myfortic therapy was
withdrawn. He received 12 doses (at 15 mg/Kg body
weight) as an intravenous infusion every 2 weeks.
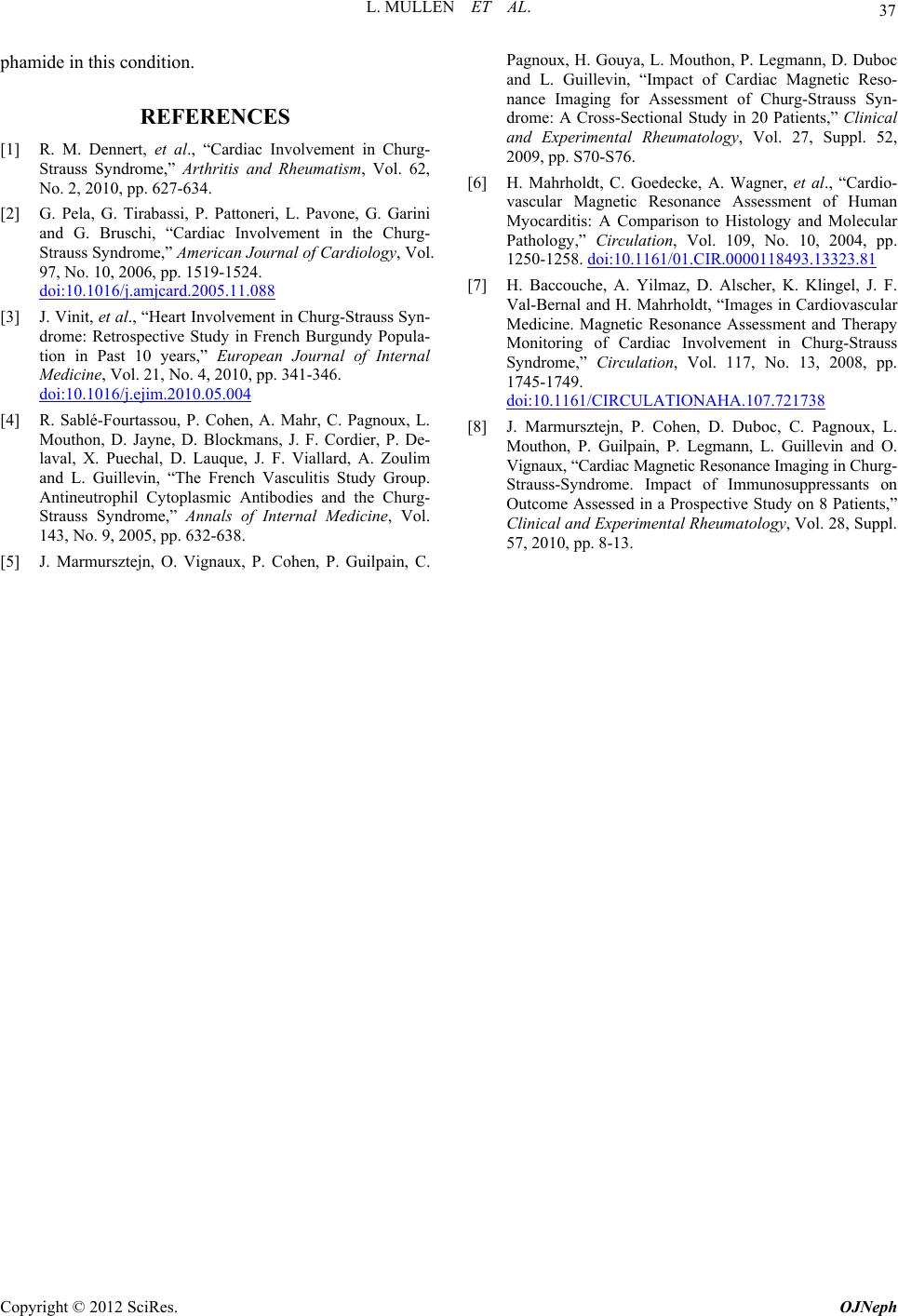
A cardiac MRI was repeated in August after 6 doses of
Cyclophosphamide. This demonstrated clear improve-
ment with a LVEF of 62%. There was very subtle hyper-
enhancement in the basal septum but significantly less
than previ o us ly. He was al so now asymptomati c .
He received his last Cyclophsophamide dose in October
2010 and was then commenced on Azathioprine therapy
at 150 mg a day. A third MRI was pe rfor med two mon th s
C
opyright © 2012 SciRes. OJNeph