R. Sariri et al. / HEALTH 2 (2010) 769-772
Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
771
771
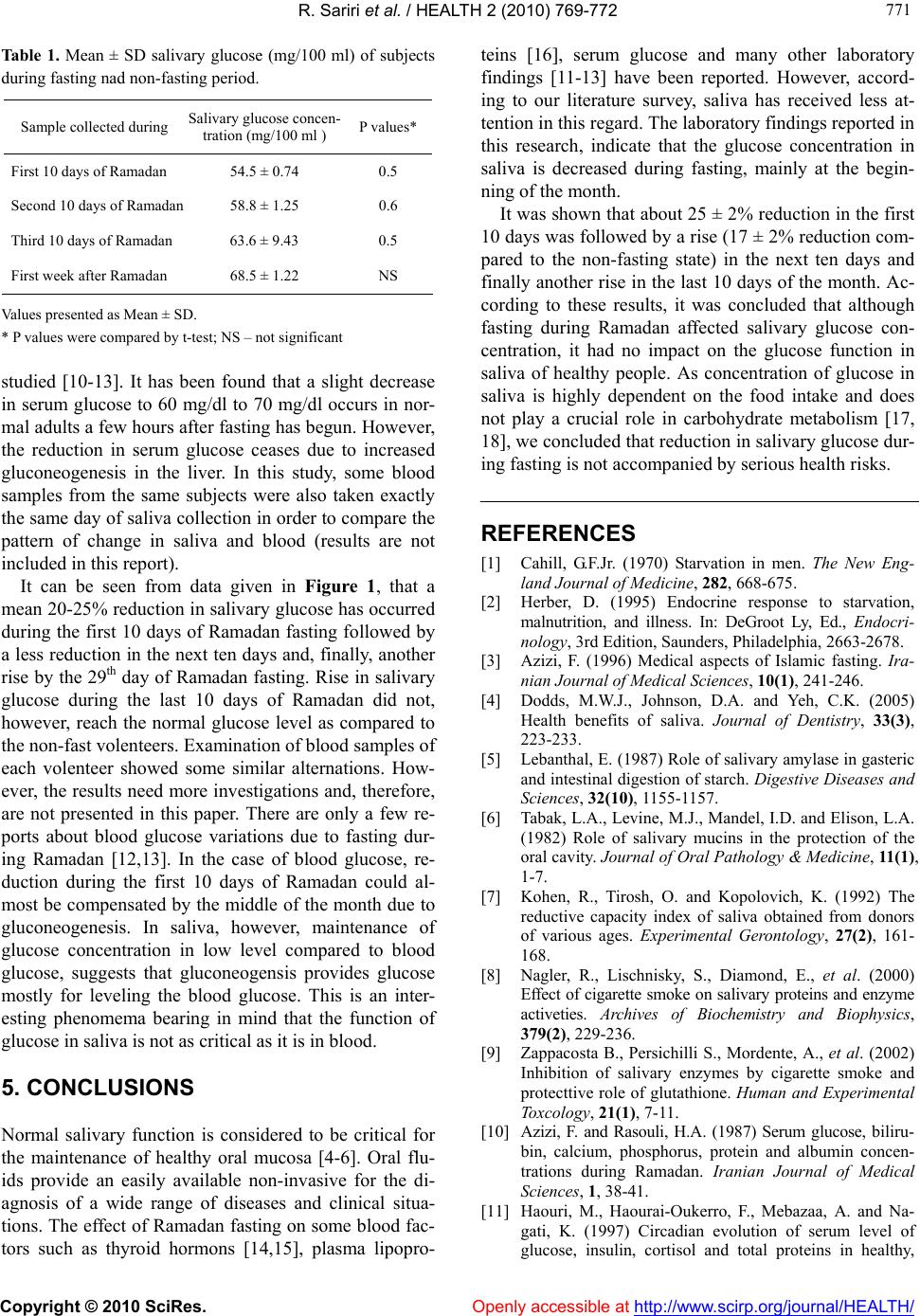
Ta bl e 1 . Mean ± SD salivary glucose (mg/100 ml) of subjects
during fasting nad non-fasting period.
Sample collected during Salivary glucose concen-
tration (mg/100 ml ) P values*
First 10 days of Ramadan 54.5 ± 0.74 0.5
Second 10 days of Ramad an 58.8 ± 1.25 0.6
Third 10 days of Ramadan 63.6 ± 9.43 0.5
First week after Ramadan 68.5 ± 1.22 NS
Values presented as Mean ± SD.
* P values were compared by t-test; NS – not significant
studied [10-13]. It has been found that a slight decrease
in serum glucose to 60 mg/dl to 70 mg/dl occurs in nor-
mal adults a few hours after fasting has begun. However,
the reduction in serum glucose ceases due to increased
gluconeogenesis in the liver. In this study, some blood
samples from the same subjects were also taken exactly
the same day of saliva collection in order to compare the
pattern of change in saliva and blood (results are not
included in this report).
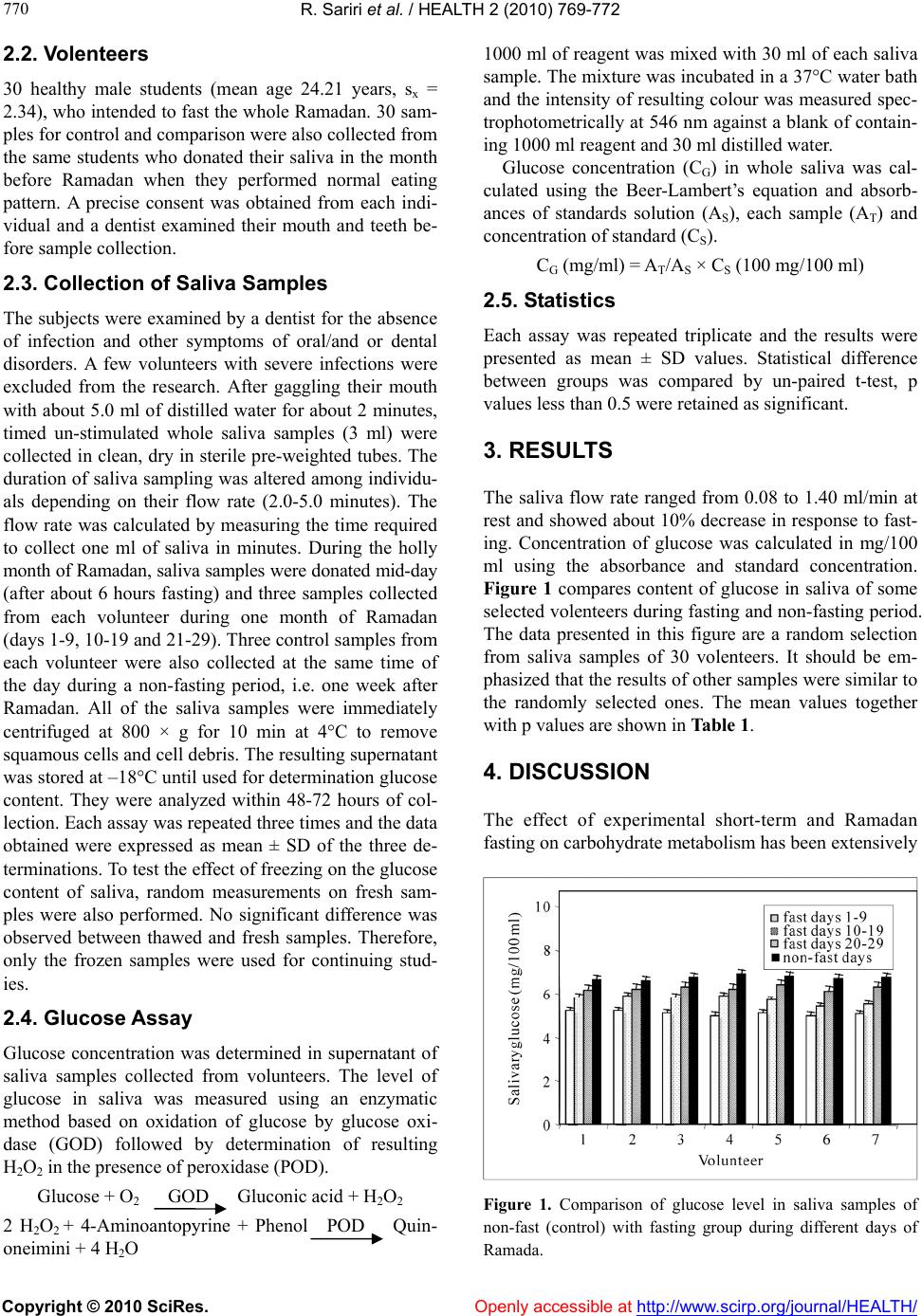
It can be seen from data given in Figure 1, that a
mean 20-25% reduction in salivary glucose has occurred
during the first 10 days of Ramadan fasting followed by
a less reduction in the next ten days and, finally, another
rise by the 29th day of Ramadan fasting. Rise in salivary
glucose during the last 10 days of Ramadan did not,
however, reach the normal glucose level as compared to
the non-fast volenteers. Examination of blood samples of
each volenteer showed some similar alternations. How-
ever, the results need more investig ations and, therefore,
are not presented in this paper. There are only a few re-
ports about blood glucose variations due to fasting dur-
ing Ramadan [12,13]. In the case of blood glucose, re-
duction during the first 10 days of Ramadan could al-
most be compensated by the middle of the month due to
gluconeogenesis. In saliva, however, maintenance of
glucose concentration in low level compared to blood
glucose, suggests that gluconeogensis provides glucose
mostly for leveling the blood glucose. This is an inter-
esting phenomema bearing in mind that the function of
glucose in saliva is not as critical as it is in blood.
5. CONCLUSIONS
Normal salivary function is considered to be critical for
the maintenance of healthy oral mucosa [4-6]. Oral flu-
ids provide an easily available non-invasive for the di-
agnosis of a wide range of diseases and clinical situa-
tions. The effect of Ramadan fasting on some b lood fac-
tors such as thyroid hormons [14,15], plasma lipopro-
teins [16], serum glucose and many other laboratory
findings [11-13] have been reported. However, accord-
ing to our literature survey, saliva has received less at-
tention in this regard . The labo ratory findings repo rted in
this research, indicate that the glucose concentration in
saliva is decreased during fasting, mainly at the begin-
ning of the month.
It was shown that about 25 ± 2% reduction in the fir st
10 days was follo wed by a r ise (17 ± 2% reduction co m-
pared to the non-fasting state) in the next ten days and
finally another rise in the last 10 days of the month. Ac-
cording to these results, it was concluded that although
fasting during Ramadan affected salivary glucose con-
centration, it had no impact on the glucose function in
saliva of healthy people. As concentration of glucose in
saliva is highly dependent on the food intake and does
not play a crucial role in carbohydrate metabolism [17,
18], we concluded that reduction in salivary glucose dur-
ing fasting is not accompanied by serious health risks.
REFERENCES
[1] Cahill, G.F.Jr. (1970) Starvation in men. The New Eng-
land Journal of Medicine, 282, 668-675.
[2] Herber, D. (1995) Endocrine response to starvation,
malnutrition, and illness. In: DeGroot Ly, Ed., Endocri-
nology, 3rd Edition, Saunders, Philadelphia, 2663-2678.
[3] Azizi, F. (1996) Medical aspects of Islamic fasting. Ira-
nian Journal of Medical Sciences, 10(1), 241-246.
[4] Dodds, M.W.J., Johnson, D.A. and Yeh, C.K. (2005)
Health benefits of saliva. Journal of Dentistry, 33(3),
223-233.
[5] Lebanthal, E. (1987) Role of salivary amylase in gasteric
and intestinal digestion of starch. Digestive Diseases and
Sciences, 32(10), 1155-1157.
[6] Tabak, L.A., Levine, M.J., Mandel, I.D. and Elison, L.A.
(1982) Role of salivary mucins in the protection of the
oral cavity. Journal of Oral Pathology & Medicine, 11(1),
1-7.
[7] Kohen, R., Tirosh, O. and Kopolovich, K. (1992) The
reductive capacity index of saliva obtained from donors
of various ages. Experimental Gerontology, 27(2), 161-
168.
[8] Nagler, R., Lischnisky, S., Diamond, E., et al. (2000)
Effect of cigarette smoke on salivary proteins and enzy me
activeties. Archives of Biochemistry and Biophysics,
379(2), 229-236.
[9] Zappacosta B., Persichilli S., Mordente, A., et al. (2002)
Inhibition of salivary enzymes by cigarette smoke and
protecttive role of glutathione. Human and Experimental
Toxcology, 21(1), 7-11.
[10] Azizi, F. and Rasouli, H.A. (1987) Serum glucose, biliru-
bin, calcium, phosphorus, protein and albumin concen-
trations during Ramadan. Iranian Journal of Medical
Sciences, 1, 38-41.
[11] Haouri, M., Haourai-Oukerro, F., Mebazaa, A. and Na-
gati, K. (1997) Circadian evolution of serum level of
glucose, insulin, cortisol and total proteins in healthy,