 International Journal of Clinical Medicine, 2012, 3, 352-360 http://dx.doi.org/10.4236/ijcm.2012.35068 Published Online September 2012 (http://www.SciRP.org/journal/ijcm) 1 Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study* Kyung Won Park1#, Eun-Joo Kim2, Hwan Joo3, Sung-Man Jeon4, Seong-Ho Choi5, Jay C. Kwon6, Byoung Gwon Kim7, Jae Woo Kim1 1Department of Neurology, Dong-A University College of Medicine, Dong-A University Medical Center, Busan, South Korea; 2Department of Neurology, Pusan National University Hospital, Pusan National University School of Medicine and Medical Research Institute, Busan, South Korea; 3Department of Neurology, Busan Medical Center, Busan, South Korea; 4Department of Neurology, Bong Seng Memorial Hospital, Busan, South Korea; 5Department of Neurology, Wallace Memorial Baptist Hospital, Busan, South Korea; 6Department of Neurology, Changwon Fatima Hospital, Changwon, South Korea; 7Department of Preventive Medicine, Dong-A University College of Medicine, Busan, South Korea. Email: #neuropark@dau.ac.kr Received May 30th, 2012; revised June 30th, 2012; accepted July 17th, 2012 ABSTRACT Background: Mild cognitive impairment (MCI) is a heterogeneous condition with a variety of clinical outcomes, the presence of which correlates with risk of Alzheimer’s disease as well as pre-clinical stages of other dementia subtypes. The aims of this study were to assess the specific patterns of cognitive profiles an d to identify changes from baseline to 24 weeks in patients with MCI using detailed neuropsychological testing. Methods: We consecutively recruited 120 MCI patients at baseline according to the Petersen’s clinical diagno stic criteria, who were admitted to the Dementia and Memory Clinics. We analyzed patients who fulfilled both in clusion and exclusion criteria for MCI and classified them into four subtypes according to deficits in major cognitive domains; amnestic MCI single domain (aMCI-s), amnestic multiple domain MCI (aMCI-m), non-amnestic single domain MCI (naMCI-s) and non-amnestic multiple domain MCI (naMCI-m). Four groups of MCI were evaluated by a detailed neuropsychological battery test. Results: 83 patients with MCI at the 24-week follow-up were classified into four subtypes. The most frequent subtype was amnestic multi-do- main MCI, with the frequency of MCI subtypes as follows: aMCI-s (n = 21, 25.3%), aMCI-m (n = 53, 63.9%), naMCI-s (n = 5, 6.0%) and naMCI-m (n = 4, 4.8%). In the major cognitive items of the SNSB-D, there were significant changes between the initial and follow-up tests in the domains of language, memory and the frontal/executive function (p < 0.05), except for attention, in all MCI patient subtypes. At 24-weeks follow-up, the conversion rate to Alzheimer’s dis- ease was 2.4% (n = 2) from a subtype of amnestic multi-domain MCI. Conclusions: Our study revealed the most fre- quent subtype of MCI to be multiple domain amnestic MCI, with this subtype having a higher tendency of conversion to Alzheimer’s disease. Keywords: Mild Cognitive Impairment; Alzheimer’s Dementia; Neuropsycholog y; Conversion 1. Introduction The recent increase of an elderly population in developed countries like South Korea has led to a renewed focus on degenerative disorders such as dementia. MCI refers to a mild regression of cognitive functions, in particular memory impairment in patients compared to that of nor- mal people, although the condition is not severe enough to be classified as dementia due to retainment of active- ties of daily living, or ADL [1]. According to some epi- demiological studies, people with MCI are in a high risk group that may progress to Alzheimer’s disease [2-4]. Whereas 1 to 2 percent of normal control groups develop dementia annually, 10 to 15 percent of MCI patients de- velop dementia, in particular, Alzheimer’s disease [5]. This condition is clinically important because it is the earliest stage that Alzheimer’s disease can be detected and the effects of treatment could therefore be maxi- mized. MCI is a syndrome involving heterogeneous clinical manifestations and diverse causative diseases. The discovery that MCI patients were likely to develop dementia led to the recognition that early diagnosis of MCI patients was crucial. *The authors d eclare no conflicts of interest. #Corresponding author. Furthermore, the classification of MCI patients ac- Copyright © 2012 SciRes. IJCM  Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study 353 cording to manifestations of cognitive dysfunction re- sulted in a renewed focus to verify which groups experi- ence a high incidence of Alzheimer’s disease among dif- ferent types of MCI patients [6-8]. Structural or func- tional brain imaging techniques, such as Magnetic Reso- nance Imaging (MRI), Positron Emission Tomography (PET) and Single-Photon Emission Computed Tomo- graphy (SPECT), were heavily employed for this re- search, with efforts to verify differences in progression patterns in accordance with the prognoses or types of MCI [6]. A classification of MCI patient subtypes along with detailed neuropsychological tests, in addition to brain imaging techniques, while observing changes in cogni- tive patterns and prognoses can provide important clues in determining whether to apply pharmacotherapy in a practical clinic setting and make long-term follow-up observations. In a report presenting the international standards for, and classification of MCI [6] suggested that memory disorder was not the only symptom of MCI patients, and that diverse cognitive disabilities may be present, such as visuospatial and language impairment, as well as frontal lobe dysfunction even from an early state of the disease. Therefore, they noted that MCI may be classified into the subtypes of amnestic MCI and non- amnestic MCI, according to whether patients have mem- ory impairment or not. They may also be classified into single and multiple domain disorders, according to the presence of a failing single cognitive do main or of multi- ple domains. In order to classify patients according to the definitions of the four subtypes of MCI, a working crite- rion in consideration of age and educational back- ground were used, with neuropsychological test tools representing each cognitive area. Based on the neuro- psychological performances, MCI divided into the sub- types: amnestic single domain MCI (aMCI-s), when the patient lacked on the memory function; amnestic multi- ple domain MCI (aMCI-m), when there were impair- ments on several cognitive areas, including memory; non-amnestic single domain MCI (naMCI-s), presence of an impairment in another cognitive area, with normal memory; and non-amnestic multiple domain MCI (naMCI- m), with impairments in more than one cognitive domain, with normal mem ory. The frequency and pattern of progression of each sub- type of MCI were inconsistent due to the presence of diverse diagnostic criteria, as well as different sampling and assessment methods. The authors performed this study with the following objectives: First, to classify new patients, who visited hospitals from September 2008 to April 2009 that were participating in the study and who were diagnosed with MCI into subtypes (amnestic single domain, amnestic multiple domain, non-amnestic single domain, and non-amnestic multiple domain), and inves- tigate each subtype’s frequency and patterns. Second, after six months elapsed, we observed whether the MCI subtypes had changed and whether they had progressed into dementia. 2. Subjects and Methods This was a multi-center, observational study conducted for 24 weeks across 13 hospitals located in Busan Met- ropolitan City, Gyeongnam Province from September 2008 to February 2010. We performed this study with full approval from the respective Institutional Review Boards of each hospital, after inspection of the clinical trial plan, written explanation for subjects, and after ob- taining each subjects’ informed consent. 2.1. Subjects We enrolled patients according to working criteria based on the clinical diagnostic criteria for MCI [5,6]: 1) the presence of subjective memory complaint as reported by participants or informants; 2) intact ability to perform activities of normal daily living; 3) normal general cog- nitive function defined as cognitive performance above the range of 1.0 standard deviation (SD) of normative data in an extensive neuropsychological test; 4) abnor- mal cognitive func tion including memory domain for ag e and education documented by performance of at least 1.0 SD below mean normative data in cognitive tasks; 5) non-demented according to DSM-IV criteria and ex- cluded by fulfilling criteria (2) and (3). The participants included in the present study were 55 to 85 years of age, had not taken acetylcholinesterase inhibitors, memantine or ginkgo bilboa for at least 4 weeks prior to the study initiation, were ambulatory or ambulatory-aided (i.e., walker or cane), had brain MRI or CT scans revealing no clinical evidence of other diseases capable of producing a dementia syndrome, and had a reliable caregiver who met the patient at least once a week and provide the in- vestigator with accurate information. The following ex- clusion criteria were adopted: 1) major depressive dis- order, bipolar disorder, schizophrenia, substance use dis- order, or mental retardation according to criteria of the DSM-IV; 2) cerebrovascular disord ers, hydrocephalus or intracranial mass, documented by CT or MRI within the past 12 months; 3) abnormalities in serum folate and vi- tamin B12, syphilis serology, or thyroid hormone levels; 4) history of traumatic brain injury or other neurologic disease; and 5) significant medical problems (e.g. poorly controlled diabetes or hypertension; cancer within the past 5 years; clinically significant hepatic, renal, cardiac or pulmonary disorders). 2.2. Neuropsychological Tests The patients’ general cognitive functions were measured Copyright © 2012 SciRes. IJCM  Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study 354 with the Korean version of the mini-mental state exam (K-MMSE) [9]. The severity of dementia was evaluated with a clinical dementia rating (CDR) [10] and the scores in the six areas of CDR were combined to calculate the sum of boxes (SOB) in each item. Overall severity was expressed with global CDR. All patients underwent neu- ropsychological tests using a standardized neuropsy- chological battery called the Seoul Neuropsychological Screening Battery—Dementia Version (SNSB-D) [11 ,12 ]. This screening battery contains tests for attention, lan- guage, praxis, parietal function, visuoconstructive func- tion, verbal and visual memory, and frontal executive function. The neuropsychological tests were: digit span (forward and backward), the Korean version of the Bos- ton Naming Test (K-BNT) [13], ideomotor praxis, Rey- Osterrieth Complex Figure Test (RCFT; copying, imme- diate and 20-min delayed recall and recognition), the Seoul Verbal Learning Test (SVLT; three learning-free recall trials of 12 words, 20-min delayed recall trial for these 12 items and a recognition test), phonemic and se- mantic Controlled Oral Word Association Test (COWAT) and the Stroop test (word an d color reading of 112 items during a 2-min period). Age-, gender- and education- specific norms for each test based on 447 norma l subjects are available. The scores of these cognitive tests were classified as abnormal when they were below the 16th percentile of the norms for respective age-, gender- and education-matched normal sub jects. 2.3. Classification of MCI Patients According to Subtypes In order to classify patients according to the definitions of the four subtypes of MCI, a working criteria in con- sideration of age and educational background were used, with neuropsychological test tools representing each cognitive area that was specified by the standard estab- lished through data research. An experienced neuropsy- chologist performed the neuropsychological tests on all patients, and based on the results, divided them into the subtypes: 1) amnestic single domain MCI (aMCI-s), when the patient lacked disabilit y in other co gn itive areas, except for degraded memory; 2) amnestic multiple do- main MCI (aMCI-m), when there were disabilities in other cognitive areas, including memory; 3) non-amnes- tic single domain MCI (naMCI-s), presence of a disabil- ity in another cogn itive area, with normal memory; and 4) non-amnestic multiple domain MCI (naMCI-m), with disabilities in more than one cogn itive domain, with nor- mal memory. 2.4. Statistical Analysis STATA/SE 11.2 (Stata Corp. 2009, College Station, TX, USA) was used for all statistical analyses, and a two- tailed test was performed with the level of significance set at 0.05. A frequency analysis was done of the subtypes, and all data collected through the neuropsychological tests were analyzed using descriptive statistics. Mean values of con- tinuous variables of the data were compared with a paired t-test and non-continuous variables were com- pared with a chi-square test. When the P value was less than 0.05, a difference was considered to be statistically significant. Based on the findings from the neuropsy- chological tests performed again six months later and the clinicians’ own judgments, we calculated the frequency of patients whose MCI progressed to dementia and cal- culated the rate of conversion of MCI to dementia in each subtype. We ascertained the frequency of each sub- type of MCI and the number of MCI patients in each subtype who had changed since the initial diagnosis. In order to verify which cognitive domain underwent the most and least changes, the scores of each of the four cognitive domains (memory, visuospatial ability, linguis- tic ability and frontal lobe function) were measured, and the scores in the beginning and in the 24th week were compared. 3. Results 3.1. Frequency of Subtypes of MCI at Baseline Among the 120 subjects of this study, the follow-up tests of a total of 83 patients were completed. In total, 23 pa- tients dropped out (follow-up loss), 9 patients withdrew their consent to participate in the study, 2 patients were relocated to other hospitals, 1 patient died, 1 patient was excluded due to use of a banned medication and 1 patient was excluded due to the onset of cerebral infarction, all during the follow-up test period. The most common sub- type among MCI patients was found to be amnestic mul- tiple domain MCI (aMCI-m). Each subtype’s frequency was as follows: aMCI-s is 25.3% (n = 21), aMCI-m is 63.9% (n = 53), naMCI-s is 6.0% (n = 5), and naMCI-m is 4.8% (n = 4) (Table 1). The rate of male to female patients among the subjects, their average age, and their number of years of education were 34.2% to 65.8%, 68.5 ± 7.5 years, and 7.0 ± 4.3 years, respectively (Table 1). 3.2. Changes of Neuropsychological Test Results in Each Subtype at 24 Weeks Follow-Up The total score and follow-up sco re changes of the Seoul Neuropsychological Screening Battery-Dementia Ver- sion (SNSB-D) in each subtype are shown in detail in Tables 2-5. After the 24 weeks follow-up period, all MCI patients showed sign ificant improvements in cogni- tive function on the total score of SNSB-D compared with the baseline assessment (P < 0.05). Furthermore, Copyright © 2012 SciRes. IJCM 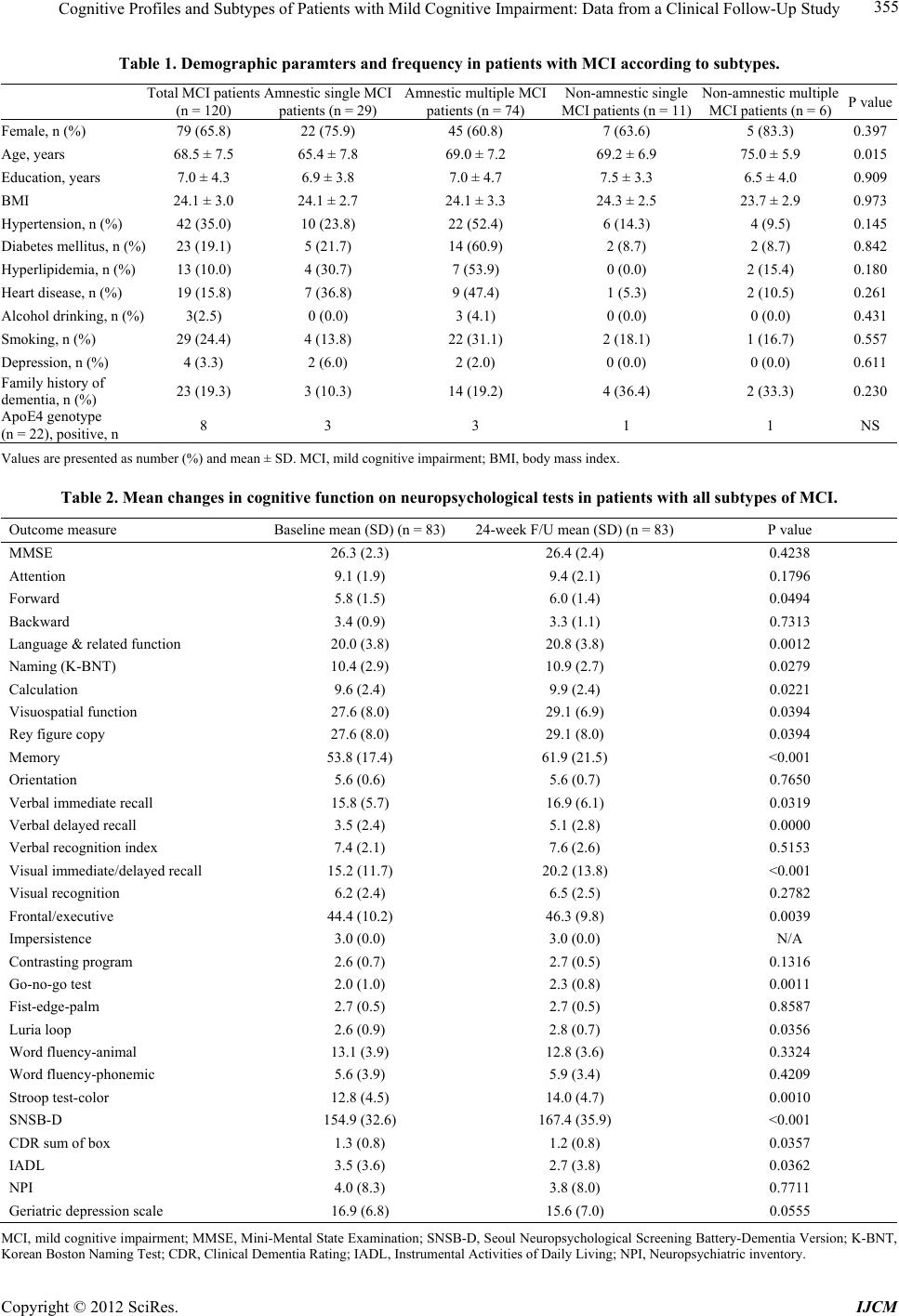 Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study Copyright © 2012 SciRes. IJCM 355 Table 1. Demographic paramters and frequency in patients with MCI according to subtypes. Total MCI patients (n = 120) Amnestic single MCI patients (n = 29) Amnestic multiple MCI patients (n = 74) Non-amnestic single MCI patients (n = 11) Non-amnestic multiple MCI patients (n = 6)P value Female, n (%) 79 (65.8) 22 (75.9) 45 (60.8) 7 (63.6) 5 (83.3) 0.397 Age, years 68.5 ± 7.5 65.4 ± 7.8 69.0 ± 7.2 69.2 ± 6.9 75.0 ± 5.9 0.015 Education, years 7.0 ± 4.3 6.9 ± 3.8 7.0 ± 4.7 7.5 ± 3.3 6.5 ± 4.0 0.909 BMI 24.1 ± 3.0 24.1 ± 2.7 24.1 ± 3.3 24.3 ± 2.5 23.7 ± 2.9 0.973 Hypertension, n (%) 42 (35.0) 10 (23.8) 22 (52.4) 6 (14.3) 4 (9.5) 0.145 Diabetes mellitus, n (%) 23 (19.1) 5 (21.7) 14 (60.9) 2 (8.7) 2 (8.7) 0.842 Hyperlipidemia, n (%) 13 (10.0) 4 (30. 7) 7 (53.9) 0 (0.0) 2 (15.4) 0.180 Heart disease, n (%) 19 (15.8) 7 (36. 8) 9 (47.4) 1 (5.3) 2 (10.5) 0.261 Alcohol drinking, n (%) 3(2.5) 0 (0.0) 3 (4.1) 0 (0.0) 0 (0.0) 0.431 Smoking, n (%) 29 (24.4) 4 (13.8) 22 (31.1) 2 (18.1) 1 (16.7) 0.557 Depression, n (%) 4 (3.3) 2 (6.0) 2 (2.0) 0 (0.0) 0 (0.0) 0.611 Family history of dementia, n (%) 23 (19.3) 3 (10.3) 14 (19.2) 4 (36.4) 2 (33.3) 0.230 ApoE4 genotype (n = 22), positive, n 8 3 3 1 1 NS Values a re presented as nu mber (%) and mean ± SD. MCI, mild cognitive impairment; BMI, body mass index. Table 2. Mean changes in cognitive function on neuropsychological tests in patients with all subtypes of MCI. Outcome measure Baseline mean (SD) (n = 83) 24-week F/U mean (SD) (n = 83)P value MMSE 26.3 (2.3) 26.4 (2.4) 0.4238 Attention 9.1 (1.9) 9.4 (2.1) 0.1796 Forward 5.8 (1.5) 6.0 (1.4) 0.0494 Backward 3.4 (0.9) 3.3 (1.1) 0.7313 Language & related func ti on 20.0 (3.8) 20.8 (3.8) 0.0012 Naming (K-BNT) 10.4 (2.9) 10.9 (2.7) 0.0279 Calculation 9.6 (2.4) 9.9 (2.4) 0.0221 Visuospatial function 27.6 (8.0) 29.1 (6.9) 0.0394 Rey figure copy 27.6 (8.0) 29.1 (8.0) 0.0394 Memory 53.8 (17.4) 61.9 (21.5) <0.001 Orientation 5.6 (0.6) 5.6 (0.7) 0.7650 Verbal immediate recall 15.8 (5.7) 16.9 (6. 1 ) 0.0319 Verbal delayed reca l l 3.5 (2.4) 5.1 (2.8) 0.0000 Verbal recognition index 7.4 (2.1) 7.6 (2.6) 0.5153 Visual immediate / d e l a yed recall 15.2 (11.7) 20.2 (13.8) <0.001 Visual recognition 6.2 (2.4) 6.5 (2.5) 0.2782 Frontal/executive 44.4 (10.2) 46.3 (9.8) 0.0039 Impersistence 3.0 (0.0) 3.0 (0.0) N/A Contrasting program 2.6 (0.7) 2.7 (0.5) 0.1316 Go-no-go test 2.0 (1.0) 2.3 (0.8) 0.0011 Fist-edge-palm 2.7 (0.5) 2.7 (0.5) 0.8587 Luria loop 2.6 (0.9) 2.8 (0.7) 0.0356 Word fluency-animal 13.1 (3.9) 12.8 (3.6) 0.3324 Word fluency- ph one mic 5.6 (3.9) 5.9 (3.4) 0.4209 Stroop test-color 12.8 (4.5) 14.0 (4.7) 0.0010 SNSB-D 154.9 (32.6) 167.4 (35.9) <0.001 CDR sum of box 1.3 (0.8) 1.2 (0.8) 0.0357 IADL 3.5 (3.6) 2.7 (3.8) 0.0362 NPI 4.0 (8.3) 3.8 (8.0) 0.7711 Geriatric dep ression scale 16.9 (6.8) 15.6 (7.0) 0.0555 MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; SNSB-D, Seoul Neuropsychological Screening Battery-Dementia Version; K-BNT, Korean Boston Naming Te st; CDR, Clinical Dementia Rating; IADL, Instrumental Activities of Daily L iving; NPI, Neuropsychiatric inventory. 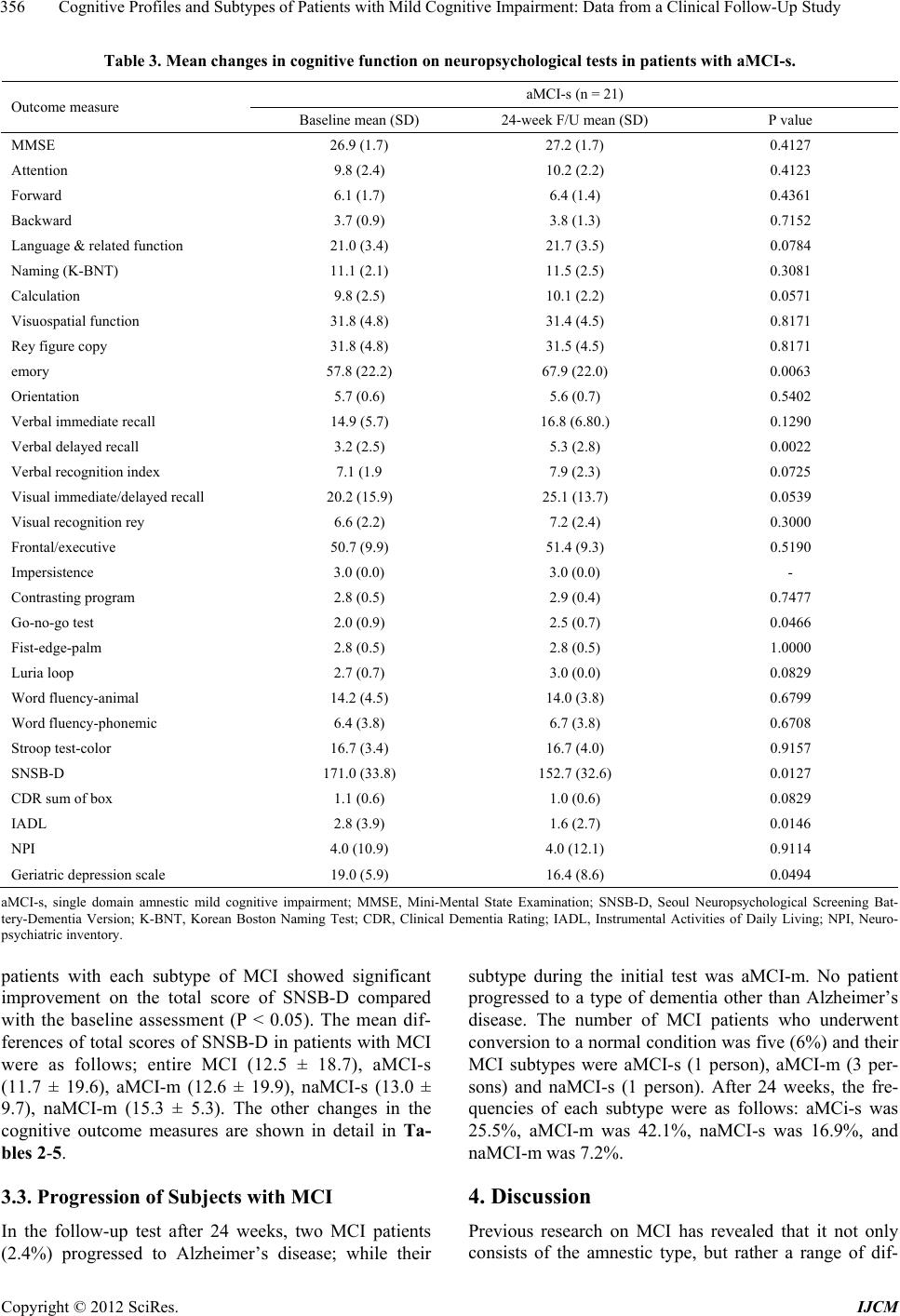 Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study 356 Table 3. Mean changes in cognitive function on neuropsychological tests in patients with aMCI-s. aMCI-s (n = 21) Outcome measure Baseline mean (SD) 24-week F/U mean (SD) P value MMSE 26.9 (1.7) 27.2 (1.7) 0.4127 Attention 9.8 (2.4) 10.2 (2.2) 0.4123 Forward 6.1 (1.7) 6.4 (1.4) 0.4361 Backward 3.7 (0.9) 3.8 (1.3) 0.7152 Language & related func ti on 21.0 (3.4) 21.7 (3.5) 0.0784 Naming (K-BNT) 11.1 (2.1) 11.5 (2.5) 0.3081 Calculation 9.8 (2.5) 10.1 (2.2) 0.0571 Visuospatial function 31.8 (4.8) 31.4 (4. 5) 0.8171 Rey figure copy 31.8 (4.8) 31.5 (4.5) 0.8171 emory 57.8 (22.2) 67.9 (22.0) 0.0063 Orientation 5.7 (0.6) 5.6 (0.7) 0.5402 Verbal immediate recall 14.9 (5.7) 16.8 (6.80.) 0.1290 Verbal delayed reca l l 3.2 (2.5) 5.3 (2.8) 0.0022 Verbal recognition index 7.1 (1.9 7.9 (2.3) 0.0725 Visual immediate/d el a yed recall 20.2 (15.9) 25.1 (13.7) 0.0539 Visual recognition rey 6.6 (2.2) 7.2 (2.4) 0.3000 Frontal/executive 5 0.7 (9.9) 51.4 (9.3) 0.5190 Impersistence 3.0 (0.0) 3.0 (0.0) - Contrasting program 2.8 (0.5) 2.9 (0.4) 0.7477 Go-no-go test 2.0 (0.9) 2.5 (0.7) 0.0466 Fist-edge-palm 2.8 (0.5) 2.8 (0.5) 1.0000 Luria loop 2.7 (0.7) 3.0 (0.0) 0.0829 Word fluency-animal 14.2 (4.5) 14.0 (3.8) 0.6799 Word fluency- ph one mic 6.4 (3.8) 6.7 (3.8) 0.6708 Stroop test-color 16.7 (3.4) 16.7 (4.0) 0.9157 SNSB-D 171.0 (33.8) 152.7 (32.6) 0.0127 CDR sum of box 1.1 ( 0.6) 1.0 (0.6) 0.0829 IADL 2.8 (3.9) 1.6 (2.7) 0.0146 NPI 4.0 (10.9) 4.0 (12.1) 0.9114 Geriatric dep ression scale 19.0 (5.9) 16.4 (8.6) 0.0494 aMCI-s, single domain amnestic mild cognitive impairment; MMSE, Mini-Mental State Examination; SNSB-D, Seoul Neuropsychological Screening Bat- tery-Dementia Version; K-BNT, Korean Boston Naming Test; CDR, Clinical Dementia Rating; IADL, Instrumental Activities of Daily Living; NPI, Neuro- psychiatric inventory. patients with each subtype of MCI showed significant improvement on the total score of SNSB-D compared with the baseline assessment (P < 0.05). The mean dif- ferences of total scores of SNSB-D in patients with MCI were as follows; entire MCI (12.5 ± 18.7), aMCI-s (11.7 ± 19.6), aMCI-m (12.6 ± 19.9), naMCI-s (13.0 ± 9.7), naMCI-m (15.3 ± 5.3). The other changes in the cognitive outcome measures are shown in detail in Ta- bles 2-5. 3.3. Progression of Subjects with MCI In the follow-up test after 24 weeks, two MCI patients (2.4%) progressed to Alzheimer’s disease; while their subtype during the initial test was aMCI-m. No patient progressed to a type of dementia other than Alzheimer’s disease. The number of MCI patients who underwent conversion to a normal condition was five (6%) and their MCI subtypes were aMCI-s (1 person), aMCI-m (3 per- sons) and naMCI-s (1 person). After 24 weeks, the fre- quencies of each subtype were as follows: aMCi-s was 25.5%, aMCI-m was 42.1%, naMCI-s was 16.9%, and naMCI-m was 7.2%. 4. Discussion Previous research on MCI has revealed that it not only consists of the amnestic type, but rather a range of dif- Copyright © 2012 SciRes. IJCM 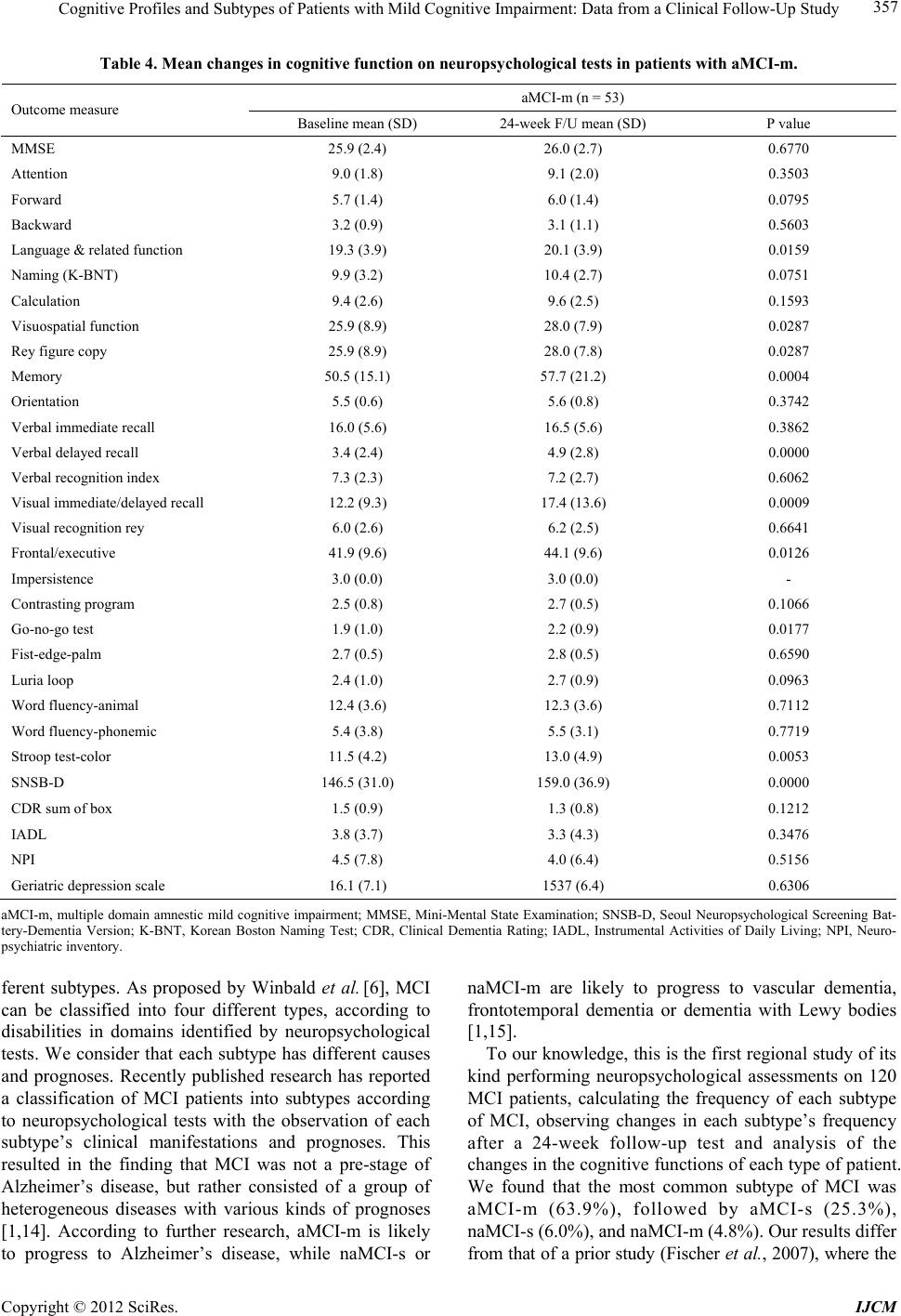 Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study 357 Table 4. Mean changes in cognitive function on neuropsychological tests in patients with aMCI-m. aMCI-m (n = 53) Outcome measure Baseline mean (SD) 24-week F/U mean (SD) P value MMSE 25.9 (2.4) 26.0 (2.7) 0.6770 Attention 9.0 (1.8) 9.1 (2.0) 0.3503 Forward 5.7 (1.4) 6.0 (1.4) 0.0795 Backward 3.2 (0.9) 3.1 (1.1) 0.5603 Language & related func ti on 19.3 (3.9) 20.1 (3.9) 0.0159 Naming (K-BNT) 9.9 (3.2) 10.4 (2.7) 0.0751 Calculation 9.4 (2.6) 9.6 (2.5) 0.1593 Visuospatial function 25.9 (8.9) 28.0 (7.9) 0.0287 Rey figure copy 25.9 (8.9) 28.0 (7.8) 0.0287 Memory 50.5 (15.1) 57.7 (21.2) 0.0004 Orientation 5.5 (0.6) 5.6 (0.8) 0.3742 Verbal immediate recall 16.0 (5.6) 16.5 (5.6) 0.3862 Verbal delayed reca l l 3.4 (2.4) 4.9 (2.8) 0.0000 Verbal recognition index 7.3 (2.3) 7.2 (2.7) 0.6062 Visual immediate / d e l a yed recall 12 .2 (9.3) 17.4 (13.6) 0.0009 Visual recognition rey 6.0 (2.6) 6.2 (2.5) 0.6641 Frontal/executive 41.9 (9.6) 44.1 (9.6) 0.0126 Impersistence 3.0 (0.0) 3.0 (0.0) - Contrasting program 2.5 (0.8) 2.7 (0.5) 0.1066 Go-no-go test 1.9 (1.0) 2.2 (0.9) 0.0177 Fist-edge-palm 2.7 (0.5) 2.8 (0.5) 0.6590 Luria loop 2.4 (1.0) 2.7 (0.9) 0.0963 Word fluency-animal 12.4 (3.6) 12.3 (3.6) 0.7112 Word fluency- ph one mic 5.4 (3.8) 5.5 (3.1) 0.7719 Stroop test-color 11.5 (4.2) 13.0 (4.9) 0.0053 SNSB-D 146.5 (31.0) 159.0 (36.9) 0.0000 CDR sum of box 1.5 (0.9) 1.3 (0.8) 0.1212 IADL 3.8 (3.7) 3.3 (4.3) 0.3476 NPI 4.5 (7.8) 4. 0 (6.4) 0.5156 Geriatric dep ression scale 16.1 (7.1) 1537 (6.4) 0.6306 aMCI-m, multiple domain amnestic mild cognitive impairment; MMSE, Mini-Mental State Examination; SNSB-D, Seoul Neuropsychological Screening Bat- tery-Dementia Version; K-BNT, Korean Boston Naming Test; CDR, Clinical Dementia Rating; IADL, Instrumental Activities of Daily Living; NPI, Neuro- psychiatric inventory. ferent subtypes. As proposed by Winbald et al. [6], MCI can be classified into four different types, according to disabilities in domains identified by neuropsychological tests. We consider that each subtype has different causes and prognoses. Recently published research has reported a classification of MCI patients into subtypes according to neuropsychological tests with the observation of each subtype’s clinical manifestations and prognoses. This resulted in the finding that MCI was not a pre-stage of Alzheimer’s disease, but rather consisted of a group of heterogeneous diseases with various kinds of prognoses [1,14]. According to further research, aMCI-m is likely to progress to Alzheimer’s disease, while naMCI-s or naMCI-m are likely to progress to vascular dementia, frontotemporal dementia or dementia with Lewy bodies [1,15]. To our knowledge, this is the first regional study of its kind performing neuropsychological assessments on 120 MCI patients, calculating the frequency of each subtype of MCI, observing changes in each subtype’s frequency after a 24-week follow-up test and analysis of the changes in the cognitive fun ctions of each typ e of patient. We found that the most common subtype of MCI was aMCI-m (63.9%), followed by aMCI-s (25.3%), naMCI-s ( 6.0%), and na MCI-m (4.8%). Our resul ts d if fer from that of a prior study (Fischer et al., 2007), where the Copyright © 2012 SciRes. IJCM 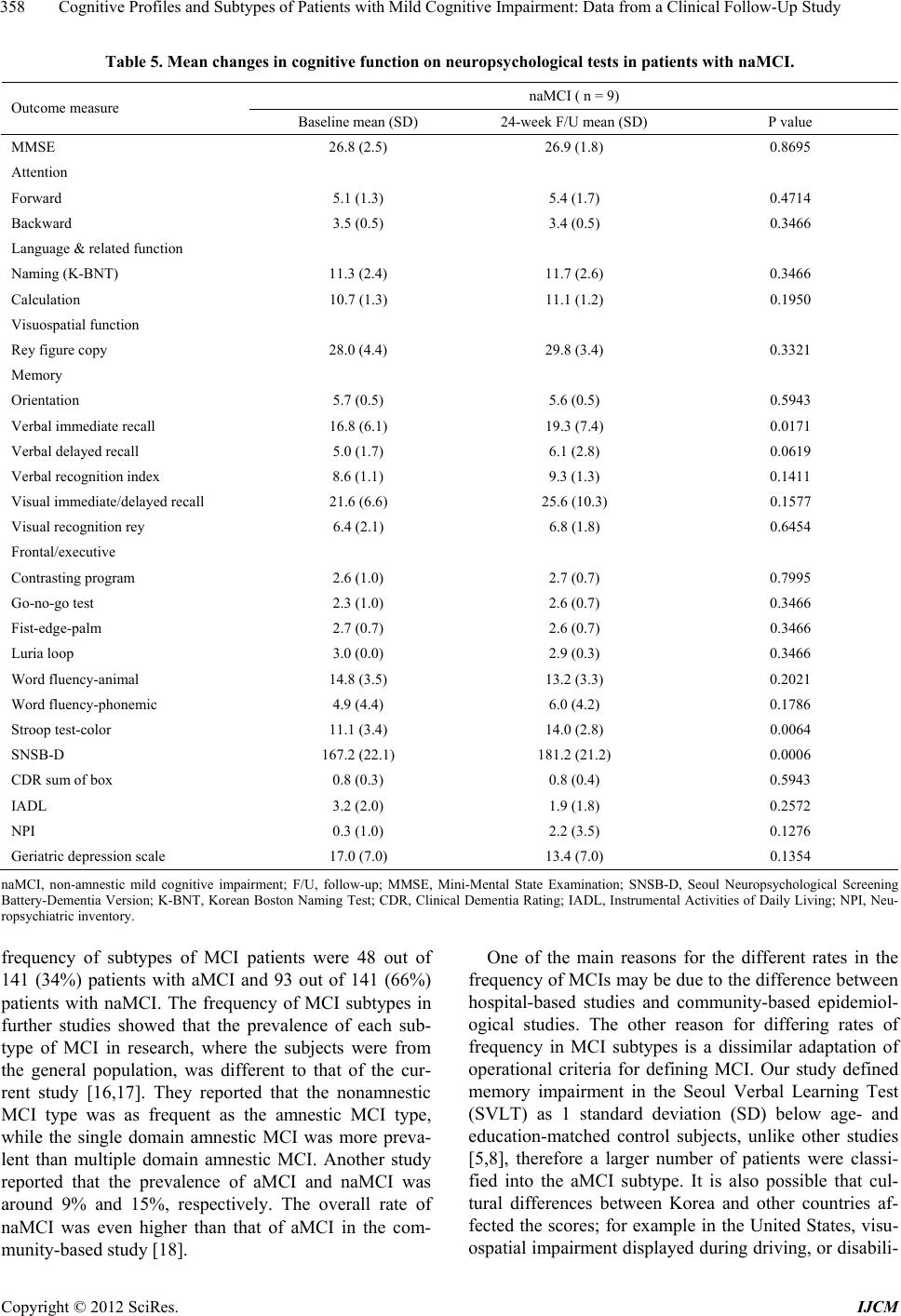 Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study 358 Table 5. Mean changes in cognitive function on neuropsychological tests in patients with naMCI. naMCI ( n = 9) Outcome measure Baseline mean (SD) 24-week F/U mean (SD) P value MMSE 26.8 (2.5) 26.9 (1.8) 0.8695 Attention Forward 5.1 (1.3) 5.4 (1.7) 0.4714 Backward 3.5 (0.5) 3.4 (0.5) 0.3466 Language & rela ted function Naming (K-BNT) 11.3 (2.4) 11.7 (2.6) 0.3466 Calculation 10.7 (1.3) 11.1 (1.2) 0.1950 Visuospatial function Rey figure copy 28.0 (4.4) 29.8 (3.4) 0.3321 Memory Orientation 5.7 (0.5) 5.6 (0.5) 0.5943 Verbal immediate recall 16.8 (6.1) 19.3 (7.4) 0.0171 Verbal delayed reca l l 5.0 (1.7) 6.1 (2.8) 0.0619 Verbal recognition index 8.6 (1.1) 9.3 (1.3) 0.1411 Visual immediate / d e l a yed recall 21 .6 (6.6) 25.6 (10.3) 0.1577 Visual recognition rey 6.4 (2.1) 6.8 (1.8) 0.6454 Frontal/executive Contrasting program 2.6 (1.0) 2.7 (0.7) 0.7995 Go-no-go test 2.3 (1.0) 2.6 (0.7) 0.3466 Fist-edge-palm 2.7 (0.7) 2.6 (0.7) 0.3466 Luria loop 3.0 (0.0) 2.9 (0.3) 0.3466 Word fluency-animal 14.8 (3.5) 13.2 (3.3) 0.2021 Word fluency- ph one mic 4.9 (4.4) 6.0 (4.2) 0.1786 Stroop test-color 11.1 (3.4) 14.0 (2.8) 0.0064 SNSB-D 167.2 (22.1) 181.2 (21.2) 0.0006 CDR sum of box 0.8 (0.3) 0.8 (0.4) 0.5943 IADL 3.2 (2.0) 1.9 (1.8) 0.2572 NPI 0.3 (1.0) 2. 2 (3.5) 0.1276 Geriatric dep ression scale 17.0 (7.0) 13.4 (7.0) 0.1354 naMCI, non-amnestic mild cognitive impairment; F/U, follow-up; MMSE, Mini-Mental State Examination; SNSB-D, Seoul Neuropsychological Screening Battery-Dementia Version; K-BNT, Korean Boston Naming Test; CDR, Clinical Dementia Rating; IADL, Instrumental Activities of Daily Living; NPI, Neu- ropsychiatric inventory. frequency of subtypes of MCI patients were 48 out of 141 (34%) patients with aMCI and 93 out of 141 (66%) patients with naMCI. The frequency of MCI subtypes in further studies showed that the prevalence of each sub- type of MCI in research, where the subjects were from the general population, was different to that of the cur- rent study [16,17]. They reported that the nonamnestic MCI type was as frequent as the amnestic MCI type, while the single domain amnestic MCI was more preva- lent than multiple domain amnestic MCI. Another study reported that the prevalence of aMCI and naMCI was around 9% and 15%, respectively. The overall rate of naMCI was even higher than that of aMCI in the com- munity-based study [18]. One of the main reasons for the different rates in the frequency of MCIs may be due to the difference between hospital-based studies and community-based epidemiol- ogical studies. The other reason for differing rates of frequency in MCI subtypes is a dissimilar adaptation of operational criteria for defining MCI. Our study defined memory impairment in the Seoul Verbal Learning Test (SVLT) as 1 standard deviation (SD) below age- and education-matched control subjects, unlike other studies [5,8], therefore a larger number of patients were classi- fied into the aMCI subtype. It is also possible that cul- tural differences between Korea and other countries af- fected the scores; for example in the United States, visu- ospatial impairment displayed during driving, or disabili- Copyright © 2012 SciRes. IJCM  Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study 359 ties in planning or decision making, may have been con- sidered important in addition to memory impairment. Furthermore, this study included cases where patients’ guardians or informants reported memory impairment even without subjective memory complaints from the patients, which resulted in a higher rate of MCI cases relative to those of other studies. During the 24 weeks follow-up period, all patients of MCI with each subtype of MCI showed significant im- provements in cognitive fun ction on the to tal score of the SNSB-D compared with the baseline assessment. In the major cognitive items of the SNSB-D, there was signifi- cant change between the initial and the follow-up as- sessments in the domains of language, memory and the frontal/executive function in all subtypes of MCI. This result is probably due to a relatively large number of pa- tients with high MMSE scores and mild stag e of patients being included, and learning effect may have resulted during the relatively short follow-up period. The condi- tion of depression may also have had an influence on the test scores, given that the patients with high depression scores in the initial tests sh owed improvement in the fol- low-up tests. Our study showed that two MCI patients (2.4%) pro- gressed to Alzheimer’s disease; their subtype during the initial test was aMCI-m. No patient progressed to other types of dementia other than Alzheimer’s disease. A 3-year follow-up research study reported that rates of conversion to Alzheimer’s disease for the MCI subtypes were 38% for amnestic MCI , 20% for non-amnestic MCI and 16% for amnestic multiple domain MCI [7]. The other long-term follow-up study revealed a conversion rate to AD at 49% for amnestic MCI and 27% for non- amnestic MCI [8]. Our study did not show in-depth con- version rates due to a shorter follow-up period. However, our results show a tendency for progression to AD from amnestic MCI rather than non-amnestic MCI. We identified some shortcomings in our study. First, although it was a prospective follow-up study, we did observe changes in the MCI patients’ subtypes and their cognitive functions during the short period of 24 weeks, therefore making it difficult to form a precise evaluation of the patients’ disease progression or an estimation of the annual rate of conversion from MCI to dementia. Second, the number of patients in each subtype was un- evenly distributed, making it difficult to determine true statistical significance. Also, differences in levels of apolipoprotein E4 were not obtained from all patients, nor the analysis of differences in MCI in accordance with the existence or non-existence of cerebrovascular lesions, such as white matter changes or lacun ar infarction. In conclusion, we were able to verify that the SNSB-D is a useful tool to classify MCI subtypes and follow their progression in detail, suggesting that the routine classifi- cation of MCI into subtypes and observation of progres- sion may be conducive to predicting a transition of MCI to Alzheimer’s disease or other types of dementia. In our study, aMCI-m was the most common subtype among the four subtypes of MCI, and its rate of conversion into Alzheimer’s disease was statistically significant. For a more comprehensive investigation, it will be necessary to perform further prospective multi-center research for a period of a few years, with many hundreds of patients as subjects, in region-based cohort studies as well as hospi- tal-based cohort studies. 5. Acknowledgements This study was supported by a grant from the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (A102065) and Eisai Korea Inc. REFERENCES [1] R. C. Petersen, R. Doody, A. Kurz, R. C. Mohs, J. C. Morris, P. V. Rabins, et al., “Current Concepts in Mild Cognitive Impairment,” Archives of Neurology, Vol. 58, No. 12, 2001, pp. 1985-1992. doi:10.1001/archneur.58.12.1985 [2] H. Amieva, L. Letenneur, J. F. Dartigues, I. Rouch- Leroyer, C. Sourgen, F. D’Alchee-Biree, et al., “Annual Rate and Predictors of Conversion to Dementia in Sub- jects Presenting Mild Cognitive Impairment Criteria De- fined According to a Population-Based Study,” Dementia and Geriatric Cognitive Disorders, Vol. 18, No. 1, 2004, pp. 87-93. doi:10.1159/000077815 [3] P. Alexopoulos, T. Grimmer, R. Perneczky, G. Domes and A. Kurz, “Progression to Dementia in Clinical Sub- types of Mild Cognitive Impairment,” Dementia and Geriatric Cognitive Disorders, Vol. 22, No. 1, 2006, pp. 27-34. doi:10.1159/000093101 [4] The Canadian Study of Health and Aging Working Group, “The Incidence of Dementia in Canada,” Neurology, Vol. 55, No. 1, 2000, pp. 66-73. doi:10.1212/WNL.55.1.66 [5] R. C. Petersen, G. E. Smith, S. C. Waring, R. J. Ivnik, E. G. Tangalos and E. Kokmen, “Mild Cognitive Impair- ment: Clinical Characterization and Outcome,” Archives of Neurology, Vol. 56, No. 3, 1999, pp. 303-308. doi:10.1001/archneur. 56.3.303 [6] B. Winblad, K. Palmer, M. Kivipelto, V. Jelic, L. Fratig- lioni, L. O. Wahlund, et al., “Mild Cognitive Impair- ment—Beyond Controversies, Towards a Consensus: Report of the International Working Group on Mild Cog- nitive Impairment,” Journal of Internal Medicine, Vol. 256, No. 3, 2004, pp. 240-246. doi:10.1111/j.1365-2796.2004.01380.x [7] F. Maioli, M. Coveri, P. Pagni, C. Chiandetti, C. Mar- chetti, R. Ciarrocchi, et al., “Conversion of Mild Cogni- tive Impairment to Dementia in Elderly Subjects: A Pre- liminary Study in a Memory and Cognitive Disorder Unit,” Archives of Gerontology and Geriatrics, Vol. 44, Copyright © 2012 SciRes. IJCM  Cognitive Profiles and Subtypes of Patients with Mild Cognitive Impairment: Data from a Clinical Follow-Up Study Copyright © 2012 SciRes. IJCM 360 No. 1, 2007, pp. 233-241. doi:10.1016/j.archger.2007.01.032 [8] P. Fischer, S. Jungwirth, S. Ze hetmay er, S. We issgram, S. Hoenigschnabl, E. Gelpi, et al., “Conversion from Sub- types of Mild Cognitive Impairment to Alzheimer De- mentia,” Neurology, Vol. 68, No. 4, 2007, pp. 288-291. doi:10.1212/01.wnl.0000252358.03285.9d [9] Y. Kang, D. L. Na and S. Hahn, “A Validity Study on the Korean Mini-Mental State Examination(K-MMSE) in Dementia Patients,” Journal of the Korean Neurological Association, Vol. 15, 1997, pp. 300-308. [10] J. C. Morris, “The Clinical Dementia Rating (CDR): Current Version and Scoring Rules,” Neurology, Vol. 43, No. 11, 1993, pp. 2412-2414. doi:10.1212/WNL.43.11.2412-a [11] Y. Kang and D. L. Na, “Seoul Neuropsychological Scr- eening Battery,” Human Brain Research & Consulting Co., Seoul, 2003. [12] H. J. Ahn, J. Chin, A. Park, B. H. Lee, M. K. Suh, S. W. Seo, et al., “Seoul Neuropsychological Screening Bat- tery-Dementia Version (SNSB-D): A Useful Tool for Assessing and Monitoring Cognitive Impairments in De- mentia Patients,” Journal of Korean Medical Science, Vol. 25, No. 7, 2010, pp. 1071-1076. doi:10.3346/jkms.2010.25.7.1071 [13] H. Kim and D. L. Na, “Normative Data on the Korean Version of the Boston Naming Test,” Journal of Clinical and Experimental Neuropsychology, Vol. 21, No. 1, 1999, pp. 127-133. doi:10.1076/jcen.21.1.127.942 [14] J. T. Tschanz, K. A. Welsh-Bohmer, C. G. Lyketsos, C. Corcoran, R. C. Green, K. Hayden, et al., “Conversion to Dementia from Mild Cognitive Disorder: The Cache County Study,” Neurology, Vol. 67, No. 2, 2006, pp. 229- 234. doi:10.1212/01.wnl.0000224748.48011.84 [15] M. Zanetti, C. Ballabio, C. Abbate, C. Cutaia, C. Vergani and L. Bergamaschini, “Mild Cognitive Impairment Sub- types and Vascular Dementia in Community-Dwelling Elderly People: A 3-Year Follow-Up Study,” Journal of the American Geriatrics Society, Vol. 54, No. 4, 2006, pp. 580-586. doi:10.1111/j.1532-5415.2006.00658.x [16] A. Busse, A. Hensel, U. Guhne, M. C. Angermeyer and S. G. Riedel-Heller, “Mild Cognitive Impairment: Long- Term Course of Four Clinical Subtypes,” Neurology, Vol. 67, No. 12, 2006, pp. 2176-2185. doi:10.1212/01.wnl.0000249117.23318.e1 [17] J. J. Manly, M. X. Tang, N. Schupf, Y. Stern, J. P. Von- sattel and R. Mayeux, “Frequency and Course of Mild Cognitive Impairment in a Multiethnic Community,” Annals of Neurology, Vol. 63, No. 4, 2008, pp. 494-506. doi:10.1002/ana.21326 [18] S. Jungwirth, S. Weissgram, S. Zehetmayer, K. H. Tragl and P. Fischer, “VITA: Subtypes of Mild Cognitive Im- pairment in a Community-Based Cohort at the Age of 75 Years,” International Journal of Geriatric Psychiatry, Vol. 20, No. 5, 2005, pp. 452-458. doi:10.1002/gps.1311
|