 International Journal of Clinical Medicine, 2012, 3, 419-425 http://dx.doi.org/10.4236/ijcm.2012.35078 Published Online September 2012 (http://www.SciRP.org/journal/ijcm) 1 The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display Morton E. Tavel St. Vincent Hospital, Indiana University School of Medicine, Indianapolis, USA. Email: mtavel@thecaregroup.com Received June 14th, 2012; revised July 15th, 2012; accepted August 4th, 2012 ABSTRACT Background: Dynamic subaortic stenosis occurs in differing situations, commonly with hypertrophic cardiomyopathy. Regardless of the underlying cause, the resulting murmurs usually possess a characteristic sound spectral pattern, mani- festing a sharp and high frequency peak occurring late in systole, often bearing a striking resemblance to the subaortic Doppler flow pattern. Methods: Murmurs found in thirty one subjects with dynamic subaortic stenosis were analyzed after having been recorded with a novel portable device capable of spectral and waveform sound displays. Results: All subjects manifested characteristic frequency patterns, consisting of high and sharp peaks occurring in late systole. With significant subaortic stenosis (resting subaortic flow velocity > 2 m/sec) this pattern was evident at rest. In the pr esence of little or no resting subaortic obstruction (<2 m/sec) this pattern was produced regularly by the Valsalva maneuver. Conclusions: Dynamic subaortic stenosis produces a specific sound spectral pattern that may provide a basis fo r clini- cal evaluation, especially in early detection of this disorder and in screening situations . Keywords: Hypertrophic Cardiomyopathy; Cardiac Physical Diagnosis; Subaortic Stenosis; Heart Murmurs; Computer Analysis of Heart Sounds 1. Background Increased subaortic blood flow velocity, (dynamic steno- sis), is commonly associated with hypertrophic cardio- myopathy, usually resulting from increased interven- tricular septal thickness in close proximity to anteriorly displaced mitral leaflets in systole [1]. This subaortic narrowing produces murmurs that may be concentrated in mid to late systole when displayed in standard wave- form phonocardiograms [2]. Other conditions producing increased intraventricular velocities, however, may rep- resent a heterogeneous group, are relatively common, and have been identified in adults of all ages with or without systolic anterior motion of the mitral valve (SAM). In the absence of SAM, increased velocity is presumed to be a result of narrowing of the midventricle, often associated with hypertrophy, a small chamber di- ameter and vigorous contraction [3-5], and has been identified in as many as 9.4% of those thought to mani- fest hypertrophic cardiomyopathy [6]. In all cases of dy- namic subaortic stenosis, however, the resulting murmurs have been described by auditory assessment as “cres- cendo-decrescendo, ejection-type, beginning after the first heart sound, peaking during mid to late systole and ending just before the second heart sound” [3]. Standard waveform phonocardiograms may demonstrate a late systolic peak intensity th at correlates with the peak Dop- pler flow signal representing maximum intracardiac ve- locity [7]. Regardless of what produces increased subaor- tic velocity, however, the resulting Doppler flow pattern usually demonstrates a sloped acceleration which ends with an abrupt peak during the latter half of systole, re- sulting in a “dagger like” appearance [8] (Figure 1(c)). The associated murmurs, when displayed by spectral techniques, often bear a close resemblance to the Doppler flow signals and thus are highly specific for this abnor- mality. In order to test the utility of sound recording with spectral display, the author has analyzed the murmurs produced in a group of subjects with dynamic subaortic stenosis. 2. Methods Subjects: The author personally reviewed the findings from a total of 31 patients referred for echocardio- graphic/Doppler study for evaluation of a systolic mur- mur or in follow-up in cases of known hypertrophic car- diomyopathy associated with subaortic stenosis. Subjects were included after the detection of increased subaortic velocities by Doppler examination in the absence of fixed obstruction at the valvular or subvalvular level. In Copyright © 2012 SciRes. IJCM  The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display 420 SM S1 S2 (a) (b) (c) Figure 1. Sound spectral patterns in a patient with subaor- tic stenosis (Resting subaortic flow velocity, 3.4 m/s). (a) Color shaded format shows a systolic murmur (SM) with peak frequency (vertical line), occurring in the latter half of systole. S1, first heart sound; S2, second heart sound. Fre- quency is displayed on the vertical axis. Waveform phono- cardiogram is displayed below in green; (b) The same murmur as shown in A, displayed in color-coded format. The white line depicts the envelope of peak frequency as shown in the right complex in this panel; (c) Doppler flow pattern at the subaortic location in the same individual. Note the similarity between this pattern and that of the sound spectral displays at the left. some instances increased velocities were absent at rest but produced through the use of the Valsalva maneuver. The overall group included 14 males and 17 females with an average age of 58.1 years (range, 16 - 88). The underlying diagnosis in many of these individuals was uncertain, for although 24 (77%) had asymmetric septal hypertrophy (septal/posterior wall ratio of >1.3), only 19 of the total 31 patien ts were thought clinically to have a form of hypertrophic cardiomyopathy. Of the total 31 patients, 21 (68%) had a history of hypertension, and 20 (65%) were older than 50 years of age. After careful auscultation at all standard locations, re- cordings were obtained from each subject at the location of maximum auditory transmission, usually from the lower left sternal border. The recording procedure gener- ally required approximately three minutes. All patients voluntarily gave informed consent according to the guidelines approved by the Institutional Review Board of St Vincent’s Hospital, Indianap olis, Indiana. Sound Recording: This was accomplished with a spe- cially designed electronic component inserted into a standard acoustic stethoscope that allowed for both lis- tening and wireless transmission to a hand held computer (Hewlett Packard, model 5500). The sounds were ob- tained digitally and transferred to a laptop computer (Dell Corp, Inspiron, Model 8600) and subsequently analyzed with the use of specially designed software. The sounds were first displayed in both a spectral and waveform format (Figures 1(a) and (b)). Waveform dis- play was produced by digital filtration (band pass) be- tween 125 and 500 Hz to facilitate recognition of indi- vidual components of the cardiac cycle, i.e., sounds and murmurs. Spectral display was performed in both color shaded and color coded formats (Figures 1-3). In the color shaded format, sound frequency is displayed on the vertical axis, and time is displayed on the horizontal axis. Color shading represents relative sound intensities at the various frequency levels; numerical quantitation of these relative values in this format is not possible. In the color coded format, however, the spectral amplitudes are plot- ted for frequencies up to 2 KHz; those amplitudes above 80% of the minimum amplitude are coded red, while those below are coded black. The border between those two regions is called the “envelope of peak frequencies” (Figure 1). We have found that optimal assessment of the murmurs’ peak frequencies was achieved when the sound spectrograph was coded in this fashion [9]. This method is also useful in producing a pattern capable of distinguishing dynamic subaortic stenosis from other causes of systolic murmurs (Figure 3). The timing of peak frequencies was measured from an average of at least three cardiac cycles and the delay of this peak ex- pressed as a percentage of systole, i.e., that interval ex- tending from the onset of the first to the second heart sound. Copyright © 2012 SciRes. IJCM  The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display 421 Hz 600 200 (a) 100m/sec (b) Figure 2. Effect of valsalva maneuver. Spectral displays in color coded (a) and color shaded (b) format, taken from a 71-year-old woman with resting subaortic peak Doppler flow velocity of 1.8 m/sec, increasing to 5.8 m/sec during the Valsalva maneuver. Recording was done at rest (at left) and with Valsalva maneuver (at right). Note that with this ma- neuver, peak frequency (vertical height) increases and the spectral patterns display the characteristic late and sharp peaks. Each spectral display is accompanied (below) by a simultaneous waveform display. Echocardiographic Examination: Complete M-mode, two-dimensional and Doppler echocardiographic exami- nations were performed on all patients using commer- cially available cardiac ultrasound equipment (Hewlett- Packard Recorder model #5500). An S3 multifocal p robe transducer was used for imaging and recorded in digi- tized form into a ProSolvR network. All measurements were performed by experienced cardiac ultrasonogra- phers. Measurement of left ventricular intracavitary velocities, chamber dimensions, septal and posterior wall thickness have been described elsewhere [10]. The Doppler veloc- ity (V) measurements were made in meters per second (m/s). Only peak intraventricular velocities were reported. A peak velocity of >1.2 m/s was considered abnormally high [3]. Systolic anterior motion of the mitral valve was de- termined with M-mode and two-dimensional display when a displacement of the anterior or posterior leaflets or both toward the septum in systole was observed. SM (a) (b ) SM (c) (d) Figure 3. Murmur patterns without subaortic stenosis. Spectral patterns in tw o other conditions unassociated with subaortic stenosis: (a) Innocent systolic murmur (Color shaded); (b) Innocent murmur (Color coded); (c) Valvular aortic stenosis (Color shaded); (d) Valvular aortic stenosis (color coded). In these examples, murmur contours (SM) are rounded and do not peak late in systole. Statistical methods: Numerical results within and be- tween groups were analyzed through the use of paired and non-paired t tests. 3. Results Twenty four subjects (77%) had asymmetric septal hy- pertrophy of the left ventricle (septum to posterior wall ratio of >1.2). Twenty one (88%) of this latter group demonstrated systolic anterior motion (SAM) of the mi- tral leaflets, and the three subjects lacking this finding had no evidence of increased subaortic velocities at rest. Seven subjects (13%) had increased midventricular ve- locities in the absence of identifiable SAM, and of this latter group, only 3 had asymmetric septal hypertrophy. Of the entire group of 31 cases, 4 subjects had peak rest- ing subaortic velocities that did not exceed 1.2 m/s. Resting values in the remaining cases exceeded this value, ranging to a high of 5.7 m/sec. Mitral regurgitation was found in 28 (90 %) of the total 31 cases. Of this latter 28, however, none was considered severe in degree: 7 were graded as minimal, 16 as mild, and 5 as mild to moderate. Table 1 and Figure 4 compare the data taken from the cases with mild resting subaortic stenosis (velocity < 2 Copyright © 2012 SciRes. IJCM 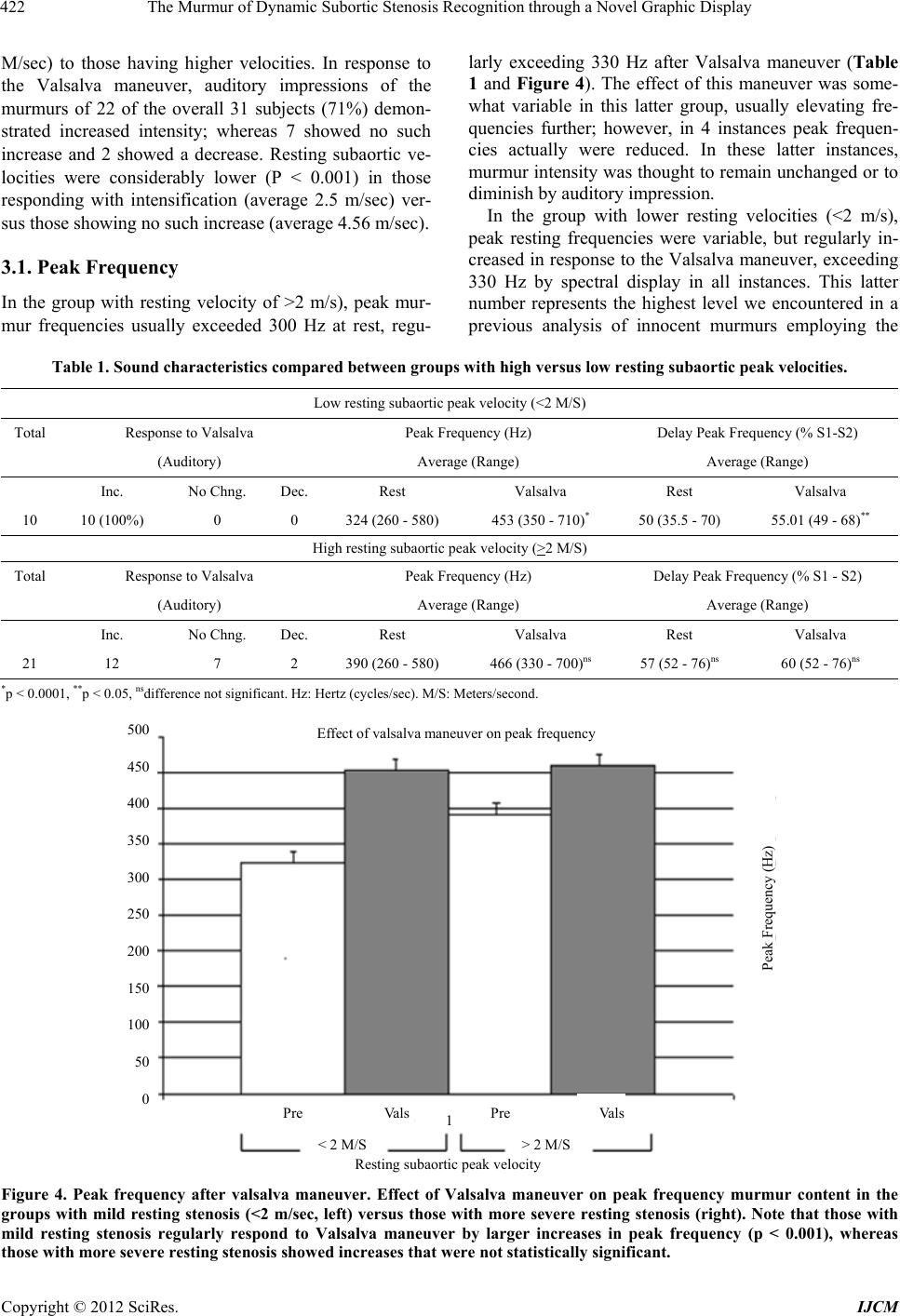 The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display Copyright © 2012 SciRes. IJCM 422 larly exceeding 330 Hz after Valsalva maneuver (Table 1 and Figure 4). The effect of this maneuver was some- what variable in this latter group, usually elevating fre- quencies further; however, in 4 instances peak frequen- cies actually were reduced. In these latter instances, murmur intensity was thoug ht to remain unchanged or to diminish by auditory impression. M/sec) to those having higher velocities. In response to the Valsalva maneuver, auditory impressions of the murmurs of 22 of the overall 31 subjects (71%) demon- strated increased intensity; whereas 7 showed no such increase and 2 showed a decrease. Resting subaortic ve- locities were considerably lower (P < 0.001) in those responding with intensification (average 2.5 m/sec) ver- sus those showing no such increase (average 4.56 m/sec). In the group with lower resting velocities (<2 m/s), peak resting frequencies were variable, but regularly in- creased in response to the Valsalva maneuver, exceeding 330 Hz by spectral display in all instances. This latter number represents the highest level we encountered in a previous analysis of innocent murmurs employing the 3.1. Peak Frequency In the group with resting velocity of >2 m/s), peak mur- mur frequencies usually exceeded 300 Hz at rest, regu- Table 1. Sound characteristics compar e d be tween groups with high versus low resting subaor tic pe ak veloc ities. Low resting subaortic peak velocity (<2 M/S) Total Response to Valsalva Peak Frequency (Hz) Delay Peak Frequency (% S1-S2) (Auditory) Average (Range) Average (Range) Inc. No Chng. Dec. Rest Valsalva Rest Valsalva 10 10 (100%) 0 0 324 (260 - 580) 453 (350 - 710)* 50 (35.5 - 70) 55.01 (49 - 68)** High resting subaortic peak velocity (>2 M/S) Total Response to Valsalva Peak Frequency (Hz) Delay Peak Frequency (% S1 - S2) (Auditory) Average (Range) Average (Range) Inc. No Chng. Dec. Rest Valsalva Rest Valsalva 21 12 7 2 390 (260 - 580) 466 (330 - 700)ns 57 (52 - 76)ns 60 (52 - 76)ns *p < 0.0001, **p < 0.05, nsdifference not significant. Hz: Hertz (cycles/sec). M/S: Meters/second. 500 450 400 350 300 250 200 150 100 50 0 Peak Frequency (Hz) 1 < 2 M/S > 2 M/S Resting subaortic peak velocity Effect of valsalva maneuver on peak frequency Pre Vals Pre Vals Figure 4. Peak frequency after valsalva maneuver. Effect of Valsalva maneuver on peak frequency murmur content in the groups with mild resting stenosis (<2 m/sec, left) versus those with more severe resting stenosis (right). Note that those with mild resting stenosis regularly respond to Valsalva maneuver by larger increases in peak frequency (p < 0.001), whereas those with more severe resting stenosis showed increases that were not statistically significant.  The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display 423 same techniques [9]. As noted above, all murmurs in this group responded to this maneuver with auditory intensi- fication. Of the 2 cases responding to the Valsalva maneuver with decreased auditory intensity, both demonstrated a fall in peak murmur frequency but a significant increase in subaortic velocity in response to this maneuver (aver- age = 2.3 m/s). In the remainng 7 showing no change in auditory murmur intensity, the murmurs demonstrated little or no change in peak frequency with only minor increases of subaortic velocities in response to this ma- neuver (average = 0.33 m/s). 3.2. Delay of Peak Frequency Overall, spectral patterns show resting peak murmur fre- quencies that are delayed past the halfway point between the first and second heart sounds (average 55.9%). Their contours are usually sharply peaked and often display a concavity on the upward limb of the spectrum, resem- bling that of the classic Doppler v e loc ity co nto u r ( Figure 1(c)). Those cases in whom resting velocities equaled or exceeded 2 m/s regularly displayed delayed peak fre- quencies at rest, averaging 57%. In the 10 cases with lower resting velocities (<2 m/sec), p eak resting murmur frequencies were variable and often occurred relatively early (average 50% between S1 and S2), differing sig- nificantly from the former group (p < 0.003). In this group with lower resting velocities, the characteristic pattern of subaortic stenosis was revealed during the Valsalva maneuver (Figure 2), with peak frequencies being increased and delayed to the later half of systole, a change that was highly significant (Table 1). Although assessing the exact time of the peak fre- quency is challenging, we minimized this potential source of error by averaging the measurements in multi- ple cardiac cycles. Nevertheless, simple visual inspection in most instances allows one to clearly identify a spectral pattern displaying a characteristic contour with its late peak frequency. 4. Discussion We have studied the murmur characteristics in a group of 31 subjects with dynamic subaortic stenosis of varying severity. Although most had asymmetric septal hyper- trophy, not all were thought clinically to have a form of hypertrophic cardiomyopathy. Since the majority had a history of hypertension and were older than 50 years of age, one could suggest that the underlying cause of in- creased subaortic velocity in many such cases was actu- ally unknown but may have been considered to be “hy- pertensive hypertrophic cardiomyopathy” [3], or possibly “hypertrophic cardiomyopathy in the elderly” [4]. Re- gardless of the underlying diagnosis, however, we have found that the spectral pattern of these murmurs is char- acteristic and usually is easily recognizable. If this pat- tern was absent at rest, it was readily produced almost immediately during the Valsalva maneuver, usually re- sembling the Doppler pattern (Figures 1 and 2). Al- though a close resemblance between spectral Doppler and acoustic displays might be intuitively expected, this study is the first to demonstrate objectively such a rela- tionship. This murmur of dynamic subaortic stenosis is easily distinguished from innocent murmurs, which regularly display rounded contours that peak in the first half of systole [9] (Figures 3(a) and (b)). Murmurs found in valvular aortic stenosis (Figures 3(c) and (d)) also pos- sess rounded contours, often reaching higher and later peak frequencies [11,12], but they are usually identifiable through recognition of this latter contour. The coexis- tence of mitral regurgitation secondary to SAM did not appear to alter the pattern produced by dynamic subaortic stenosis. Although most of the subjects had mitral regur- gitation (usu ally mild to moderate), none of the recorded murmurs gave any indication that they were caused pri- marily by this flow disturbance. This is implied by the characteristic murmur frequency patterns, cessation of murmurs before the second heart sound, and typical re- sponses to the Valsalva maneuver. As a practical matter, therefore, recognition of the underlying dynamic subaor- tic stenosis was not impaired by abnormal mitral flow. By contrast, the independent presence of mitral regurgi- tation generally produces a murmur that contains no sharp peak frequencies and extends to or beyond the second heart sound [12]. Although 7 of our subjects demonstrated mid-ven- tricular obstruction without systolic anterior motion of the mitral valve (SAM), we were unable to detect any difference in the spectral systolic murmur characteristics between this group and those with SAM. Unfortunately, in this regard, our numbers were too few to allow for definitive conclusions. Most subjects in this study displayed auditory intensi- fication and the appearance of characteristic murmur spectral envelope in response to the Valsalva maneuver. This effect appeared to be most dramatic in subjects possessing low resting subaortic velocities, and this ob- servation might prove useful in detection of cases har- boring more subtle variations of these conditions which may be more common than heretofore recognized [3,13]. Although auditory perception of intensification is easiest in the presence of a soft or absent murmur, this study provides objective support to the concept that, in the presence of resting high-grade stenosis, murmurs often show no change—or even reduction—of intensity in re- sponse to this maneuver. These findings suggest that murmur intensity and frequency reflect a complex inter- Copyright © 2012 SciRes. IJCM  The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display 424 play between velocity and volume of flow across the stenotic area, i.e. , very high velocity may be accompa- nied by reduced flow volume, yielding lowered auditory intensity and frequency. Spectral display of sounds possesses distinct advan- tages over the classic waveform displays (phonocardio- graphy) that have been used for many years [12], for they require no wave filtration and allow for a large range of intensities to be plotted on the same graph. This also provides a far better means of identification and meas- urement of peak frequencies. Nevertheless, waveform display is easily obtained simultaneously with the spec- tral format and can play a useful role in overall murmur characterization and in demonstrating murmur placement relative to the heart sounds. We have also shown spectral displays to be potentially useful in other clinical situa- tions, such as in assessing severity of valvular aortic stenosis [11], the distinction of innocent murmurs from those of aortic stenosis [9], and in the evaluation of cer- vical bruits in order to predict the likelihood of severe carotid arterial obstruction [14]. The technique used in this study is portable, inexpen- sive, easily applied, and requires little time for an indi- vidual examination. It is readily adaptable to a handheld computer or cellular telephone that possesses visual dis- plays and also provides immediate playback for auditory review. These attributes make it potentially applicable to screening and diagnosis in any situation associated with dynamic subaortic stenosis, especially hypertrophic car- diomyopathy [13]. Since this condition is often the un- derlying cause of sudden death in young athletes, more inexpensive and efficacious screening tools appear to be urgently needed [15]. The present technique may allow for the detection of cases harboring such obstruction, especially if one employs the Valsalva maneuver with the subject in the upright position, a maneuver that can provoke obstruction when there is none at rest. Spectral display of sounds also offers the opportunity to detect pathological fourth heart sounds [17], often encountered in hypertrophic cardiomyopathy with or without subaor- tic stenosis [18]. Another potential clinical application of spectral sound recording would be in determination of the underlying mechanism of a systolic murmur found together with other situations associated with murmurs, such as in normals (innocent murmur) and valvular aortic stenosis (Figure 3). In the present study, recognition of the mur- mur of dynamic subaortic stenosis was not impaired by the presence of coexistent secondary mitral regurgitation. By contrast, the author has found that mitral regurgitation arising from independent causes such as mitral prolapse is easily distinguished from this pattern [12]. Finally, the present system provides a novel means to teach cardiac auscultation, for it allows for graphic dis- play and immediate playback to single and multiple si- multaneous listeners [19]. Moreover, the recordings can be transmitted wirelessly to distant sites and stored per- manently for later retrieval. This method requires little training and expertise, is portable and rapidly imple- mented, and can be applied at the point of care for a frac- tion of the cost of cardiac ultrasound. Recently dev eloped hand-held echocardiography has been advocated as a substitute for cardiac au scultation [20], but it is relatively expensive, has limited Doppler flow interrogation, and requires significant operator experience. Study Limit a tions The current study contained a selected and limited number of examples of individuals found to have dy- namic subaortic stenosis. Additional studies would be required to confirm and extend these applications to lar- ger groups, especially in screening for this disorder and establishing its effect on ultimate outcomes. Mid-ventricular obstruction in the absence of SAM of the mitral apparatus might potentially produce a subaor- tic velocity pattern that peaks earlier in systole [21] and possibly may produce a deviant murmur that does not conform to the pattern described in this study. Although we noted no such tendency in the few cases falling into this category, our study population contained an insuffi- cient number to allow for any conclusions regarding this possibility. 5. Acknowledgements The author is indebted to Hart Katz, MD, PhD for provi- sion of materials used in this study and for valuable sup- port in the preparation of this manuscript. REFERENCES [1] B. J. Maron, M. S. Maron, D. Wigle, et al., “The 50-Year History, Controversy, and Clinical Implications of Left Ventricular Outflow Tract Obstruction in Hypertrophic Cardiomyopathy,” Journal of the American College of Cardiology, Vol. 54, No. 3, 2009, pp. 191-200. [2] M. E. Tavel, “Clinical Phonocardiography and External Pulse Recording,” 4th Edition, Year Book Medical Pub- lishers, Chicago, 1985, p. 147. [3] P. H. Spooner, P. Perry, R. O. Brandenburg and G. D. Pennock, “Increased Intraventricular Velocities: An Un- recognized Cause of Systolic Murmur in Adults,” Journal of the American College of Cardiology, Vol. 32, No. 6, 1998, pp. 1589-1595. [4] H. M. Lever, R. F. Karam, P. J. Currie, et al., “Hypertro- phic Cardiomyopathy in the Elderly,” Circulation, Vol. 79, No. 3, 1989, pp. 580-589. [5] M. R. Harrison, C. G. Grigsby, S. K. Southern, M. D. Smith, et al., “Midventricular Obstruction Associated with Chronic Systemic Hypertension and Severe Left Ventricular Hypertrophy,” American Journal of Cardiol- Copyright © 2012 SciRes. IJCM  The Murmur of Dynamic Subortic Stenosis Recognition through a Novel Graphic Display Copyright © 2012 SciRes. IJCM 425 ogy, Vol. 68, 1991, pp. 761-765. doi:10.1016/0002-9149(91)90650-A [6] Y. Minami, K. Kajimoto, Y. Terajima, B. Yashiro, D. Okayama, S. Haruki, T. Nakajima, N. Kawashiro, M. Kawana and N. Hagiwara, “Clinical Implications of Mid- ventricular Obstruction in Patients with Hypertrophic Cardiomyopathy,” Journal of the American College of Cardiology, Vol. 57, No. 23, 2011, pp. 2346-2355. [7] N. Fukuda, T. Oki, A. Iuchi, T. Tabata, K. Manabe, et al., “Clinical Significance of the Apical Late Systolic Ejec- tion Murmur: A New Phonocardiographic Sign Indicating Dynamic Mid-Left Vent ricular Obstruction,” Clinical C ar- diology, Vol. 19, 1996, pp. 121-127. doi:10.1002/clc.4960190210 [8] W. F. Armstrong and T. Ryan, “Feigenbaum’s Echocar- diography,” 6th Edition, Lippincott Williams and Wilkins, Philadelphia, 2005, p. 549 [9] W. F. Armstrong and T. Ryan, “Feigenbaum’s Echocar- diography,” 6th Edition, Lippincott Williams and Wilkins, Philadelphia, 2005, p. 545. [10] M. E. Tavel and H. Katz, “Usefulness of a New Sound Spectral Averaging Technique to Distinguish an Innocent Systolic Murmur from That of Aortic Stenosis,” Ameri- can Journal of Cardiology, Vol. 95, No. 7, 2005, pp. 902-904 [11] D. Kim and M. E. Tavel, “Assessment of Severity of Aortic Stenosis through Time-Frequency Analysis of Murmur,” Chest, Vol. 124, No. 5, 2003, pp. 1638-1644. [12] M. E. Tavel, “Cardiac Auscultation: A Glorious Past— And It Does Have a Future!” Circulation, Vol. 113, No. 9, 2006, pp. 1255-1259. [13] M. S. Maron, I. Olivotto, A. G. Zenovich, et al., “Hyper- trophic Cardiomyopathy Is Predominantly a Disease of Left Ventricular Outflow Tract Obstruction,” Circulation, Vol. 114, No. 21, 2006, pp. 2323-2239. [14] M. E. Tavel and Bates, “The Cervical Bruit: Sound Spec- tral Analysis Related to Severity of Carotid Arterial Dis- ease,” Clinical Cardiology, Vol. 29, No. 10, 2006, pp. 462-465. [15] D. Montellese, “Preventing Sudden Cardiac Death in Young Athletes: Are Current Preparticipation Screening Guidelines Appropriate?” Cardiology Review, Vol. 23, 2006, pp. 34-38. [16] M. S. Maron, I. Olivotto, S. Betocchi, et al., “Effect of Left Ventricular Outflow Tract Obstruction on Clinical Outcome in Hypertrophic Cardiomyopathy,” New Eng- land Journal of Medicine, Vol. 348, No. 4, 2003, pp. 295-303. doi:10.1056/NEJMoa021332 [17] E. Baracca, M. C. Brunazzi, M. Pasqualine, et al., “An Estimation of the Left Ventricular Diastolic Function from the Spectral Analysis of the Fourth Heart Sound. A Doppler Validated Study in Hypertrophic Cardiomyopa- thy,” Acta Cardiologica, Vol. 50, 1995, pp. 17-21. [18] E. D. Wigle, H. Rakowski, B. P. Kimball, et al., “Hyper- trophic Cardiomyopathy; Clinical Spectrum and Treat- ment,” Circulation, Vol. 92, No. 7, 1995, pp. 1680-1692. [19] M. E. Tavel, “Cardiac Auscultation: A New Method for Instruction,” Medical Education, Vol. 44, No. 11, 2010, p. 1132. doi:10.1111/j.1365-2923.2010.03831.x [20] M. J .Liebo, R. L. Israel, E. O. Lillie, M. R. Smith, D. S. Rubenson and E. J. Topol, “Is Pocket Mobile Echocardi- ography the Next-Generation Stethoscope? A Cross-Sec- tional Comparison of Rapidly Acquired Images with Standard Transthoracic Echocardiography,” Annals of In- ternal Medicine, Vol. 155, No. 1, 2011, pp. 33-38. [21] M. V. Sherrid, O. Wever-Pinzon, A. Shah, et al., “Reflec- tions of Inflections in Hypertrophic Cardiomyopathy,” Journal of the American College of Cardiology, Vol. 54, No. 3, 2009, pp. 212-219.
|