Levels of Immunoglobulin Classes Are Not Associated with Severity of HIV Infection in Nigerian Patients 235
vious studies [4,6,8]. IgA is the most important immu-
noglobulin involved in mucosal defenses [4,13]. The
same trend on the IgG levels was observed with systemic
total IgA levels increasing during progression to AIDS
[4]. Polyclonal immune activation and production of
specific cytokines (IL 5 and IL 6) appear to be some of
the mechanism responsible. However slight elevations of
IgA may simply be a reflection of genetic and environ-
mental factors within an African population. Common
viral infections are initiated by local invasion of epithet-
lial surfaces, which initially induces local production of
interferon and secretory IgA from these surfaces [10].
Serum IgA antibodies have also been shown to have neu-
tralizing activity on HIV [10] but this effect diminishes
with disease progression allowing passage of IgA into
the blood and resulting in increased serum levels of IgA.
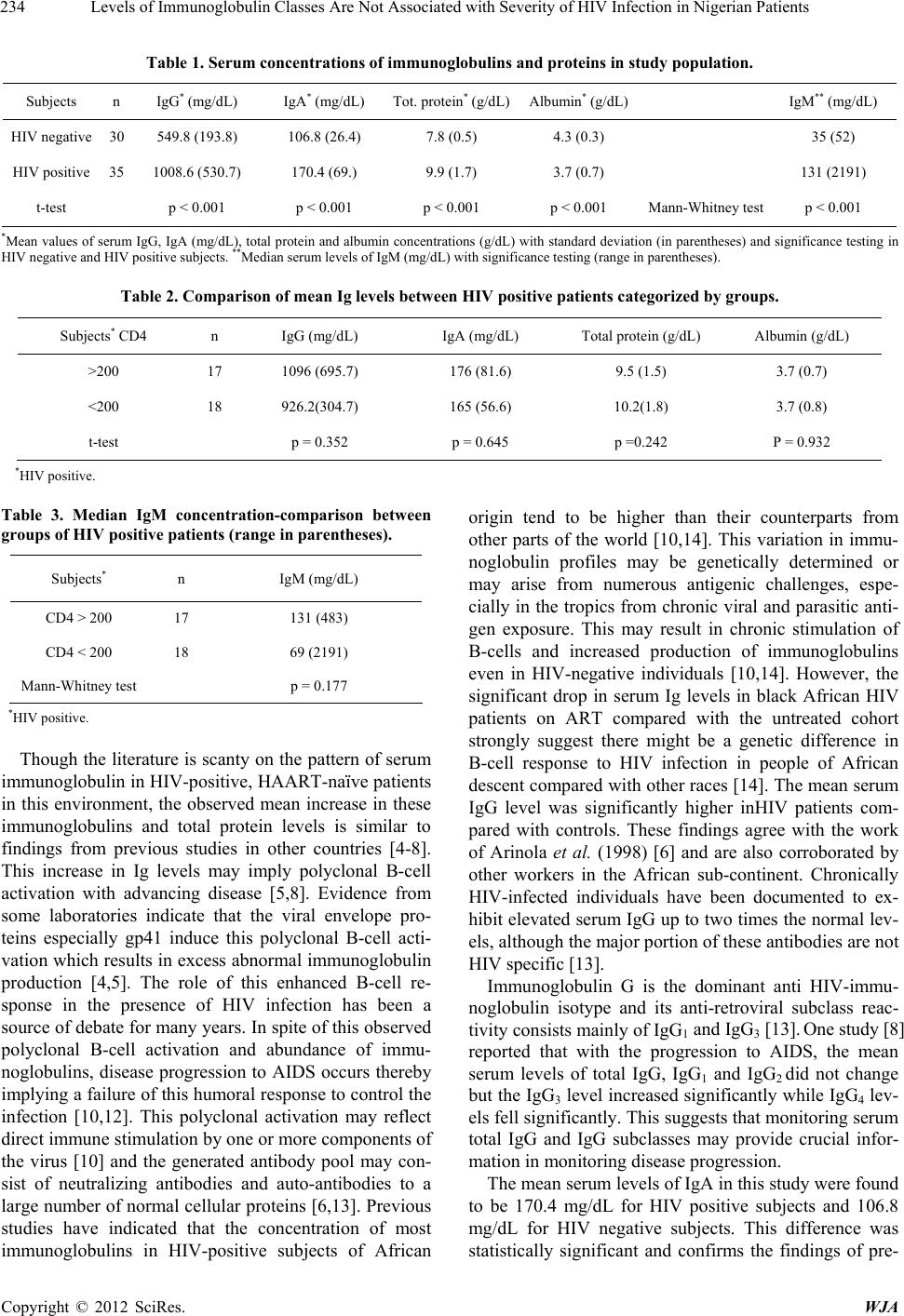
The median serum levels of IgM were also signifi-
cantly higher in HIV-positive than HIV negative subjects
(p < 0.001). This also confirms findings of previous
studies [6,8]..
In this study, the HIV positive subjects were further
stratified into two groups based on their CD4+ T cell
count into those with CD4+ cell count < 200 cells/µL and
those with >200 cells/µL. This was done to compare
CD4 cell count with serum immunoglobulin levels among
the HIV sero-positive subjects and to determine any as-
sociation between CD4 cell counts and observed serum
Ig levels. There were no statistically significant differ-
ences in these values (p > 0.05). These findings are simi-
lar to those in a study in Tanzania [7] which reported an
insignificant correlation between high serum immu-
noglobulin levels and CD4 count.
Low albumin levels have also been associated with
HIV disease progression and one study [15] reported that
among 453 HIV infected individuals, albumin < 35 g/l
(3.5 g/dl) was associated with faster progression to AIDS.
Other studies have associated low albumin levels with
all-cause mortality in AIDS; however it could not be de-
termined whether low albumin levels among these indi-
viduals were caused by HIV infection or were reflective
of the inherent state of health of the individual. Different
hypotheses have been proposed to explain the low levels
of albumin seen in HIV infection [15]. Some studies
have demonstrated that HIV co-infection with HCV ac-
celerates the progression of liver disease while other
studies have found albumin to be a significant predictor
of HIV disease progression even among those not in-
fected with HCV [16]. It is also possible that low that
low albumin levels may reflect the effects of anorexia,
poor nutritional status or chronic inflammation (albumin
is a negative acute phase reactive protein whose levels
can possibly be depressed by elevated levels of TNF and
IL-1 during chronic inflammation) [15]. In this study,
mean serum albumin was 4.3 g/dL among HIV negative
subjects and 3.7 g/dL among HIV positive subjects. This
difference was statistically significant. However no sig-
nificant difference was observed among HIV positive
subjects with CD4 cell count ≥ 200 cells/µL versus those
with CD4 counts < 200 cells/µL.
In this study serum IgA, IgG and IgM concentration
were non-significantly correlated to viral loads in all HIV
positive subjects (r = –0.206, –0.032 and –0.316 respec-
tively).
5. Conclusions
This study confirms that serum levels of total protein,
IgG, IgA and IgM are elevated in the course of HIV in-
fection while serum albumin levels are lower.
Although the value of immunoglobulin concentration
in predicting CD4+ cell count may appear limited on its
own, measuring levels in conjunction with other bio-
chemical parameters (such as the serum albumin levels)
may potentially be used to monitor both disease pro-
gression and response to HAART. This might be used to
advantage in low resource settings as the cost for anti-
body measurements is much lower than that for HIV
RNA determination.
REFERENCES
[1] B. Taiwo, “General HIV Medicine,” The Floating Gallery
Press, 2004, pp. 3-30.
[2] A. Abayomi, N. Adomakoh and S. Adomakoh, “Res-
pondïng to the HIV Epidemic in the Developing World.
Capacity Building and Technology Transfer for Monitor-
ing with HAART: A Caribbean Experience,” African
Journal of Medicine & Medical Sciences, Vol. 34, 2005,
pp. 19-24.
[3] D. O. Olaleye, T. O. Harry and G. N. Odaibo, “The Vi-
rology and Dynamics of the Epidemic in Nigeria,” In: O.
Adeyi, P. J. Kanki, O. Odutolu and J. A. Idoko, Eds., Aids
in Nigeria: A Nation on the Threshold, Harvard Centre
for Population and Development Studies, Cambridge,
2006, pp. 37-66.
[4] J. M. Pascale, M. D. Isaacs, P. Contreras, B. Gomez, L.
Lozano, E. Austin, M. C. De Martin, R. L. Gregory,
McLaughlin and A. Amador, “Immunological Markers of
Disease Progression in Patients Infected with the Human
Imunodeficiency Virus,” Clinical and Vaccine Immunol-
ogy, Vol. 4, No.4, 1997, pp. 474-477.
[5] O. G. Arinola, L. S. Salimonu, O. H. Okiwelu and C. P.
Muller, “Levels of Immunoglobulin Classes, Acute Phase
Proteins and Serum Electrophoresis in Nigerians Infected
with Human Immmunodeficiency Virus,” European Jour-
nal of Scientific Research, Vol. 7, No. 3, 2005, pp. 34-44.
[6] O. G. Arinola and J. Igbi, “Serum Immunoglobulins and
Circulating Immune Complexes in Nigerians with Human
Immmunodeficiency Virus and Pulmonary Tuberculosis
Infection,” Tropical Journal of Medical Research, Vol. 2,
No. 2, 1998, pp. 41-48.
Copyright © 2012 SciRes. WJA