 Journal of Cosmetics, Dermatological Sciences and Applications, 2012, 2, 201-211 http://dx.doi.org/10.4236/jcdsa.2012.23037 Published Online September 2012 (http://www.SciRP.org/journal/jcdsa) 201 Utilizing Free Skin Grafts in the Repair of Surgical Wounds Madalene C. Y. Heng Department of Medicine/Dermatology, UCLA School of Medicine, Los Angeles, USA. Email: madaleneheng@aol.com Received May 24th, 2012; revised June 26th, 2012; accepted July 11th, 2012 ABSTRACT The use of free grafts to close defects in wounds following surgery has long been utilized in dermatology practice. However, because of the low survival of the grafts, their popularity has dwindled over recent years. The use of tech- niques such as attaching an “umbilical cord” from the base of the grafts to the underlying deep fascia or cartilage has markedly increased graft survival. In this paper, the scope of free grafts is presented, showing survival of even large grafts if anchored to the deep tissue with multiple “umbilical cord” attachments. The advantages of full-thickness free skin grafts include the ability to close the wound immediately following removal of the tumor, with decreased risk of infection and pain, requiring fewer dressing changes and visits. The technique of close stitching, with interrupted su- tures 1 - 2 mm apart, prevents contact of the wound with oxygen from the air, resulting in increased graft survival from revascularization of the free graft. With the added use of extra-strength curcumin gel, perfect regeneration may be achieved. In addition, in most free grafts, it was observed that there was recovery of sensation due to presumed nerve regeneration. Keywords: Free Skin Grafts; Surgical Wounds; Curcumin 1. Introduction The closure of wound defects following excision of skin cancers is a ubiquitous problem not only in dermatology, but also in plastic surgery. The initial popularity of spilt skin grafts (partial thickness skin grafts) for closing wound defects stemmed from frequent failure of the full-thickness grafts to survive. However, the result achieved by the use of split skin grafts is often cosmetically undesirable, with loss of sensation in the grafted areas. Pedicle flaps [1,2] were then developed in order to enhance graft survival using sequential revascularization techniques. These are difficult to perform, and involve the anastomoses of ar- teries and veins, and transfer of deep tissues such as the gracilis muscle, latissimus dorsi muscle, and bone [1-8]. They are also are frequently multi-staged [1,2], although single-staged free pedicle flaps from neighboring tissue have been described [3,4]. Full-thickness free grafts are simple, and easy to per- form. However, the low percentage of graft survival, with many of the larger grafts undergoing partial or complete necrosis within 7 days, leading to scarring and infection, may be the main reason for limitation of the technique to extremely small grafts. However, we have observed that the technique of using an “umbilical cord” attachment between the base of the graft to the floor of the open wound, achieved observed improved survival due to enhanced revascularization of the graft [8]. Recently, we have used multiple “umbilical cord” at- tachments to improve the survival of larger grafts. In this paper, we further describe our technique of enhancing survival of free grafts, and illustrate the efficacy of the technique in a number of cases which demonstrate the scope of free graft utilization in the repair of post-surgi- cal wounds. 2. Techniques and Methods 2.1. Selection of Donor Site for the Free Grafts It is important to carefully select the skin to be used to bridge the defect in the surgical wound after excision of the tumor. We have found that whenever possible, skin from the adjacent tissue is optimal because this serves as the best match for the skin overlying the open wound. If this is not possible, skin of similar thickness and similar number of hair follicles and sebaceous glands are se- lected. For example, for the nose, we have found the forehead skin around the glabella or mid forehead is probably more suitable than skin from behind the ears. For the skin of the dorsum of the fingers, the dorsum of Copyright © 2012 SciRes. JCDSA 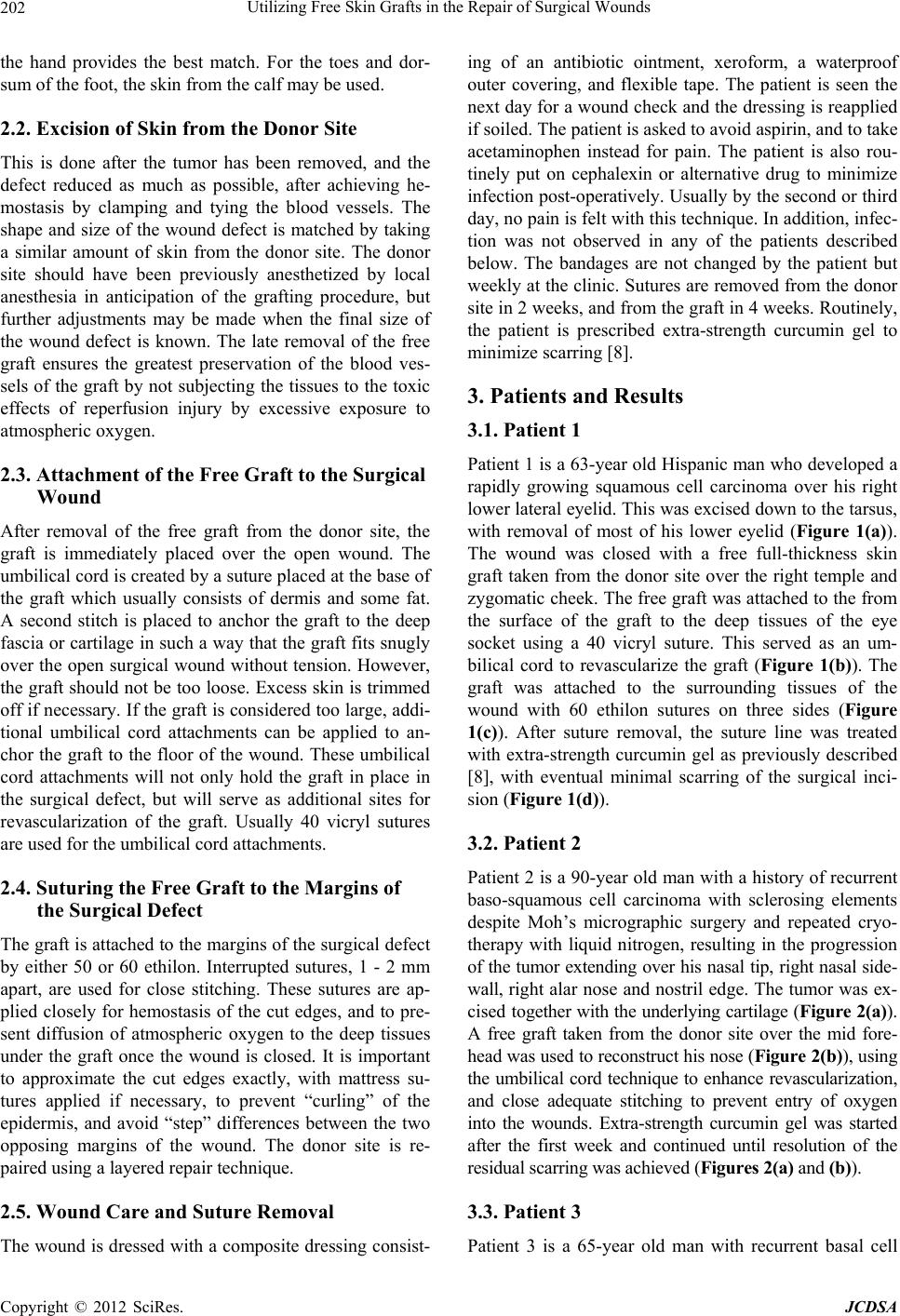 Utilizing Free Skin Grafts in the Repair of Surgical Wounds 202 the hand provides the best match. For the toes and dor- sum of the foot, the skin from the calf may be used. 2.2. Excision of Skin from the Donor Site This is done after the tumor has been removed, and the defect reduced as much as possible, after achieving he- mostasis by clamping and tying the blood vessels. The shape and size of the wound defect is matched by taking a similar amount of skin from the donor site. The donor site should have been previously anesthetized by local anesthesia in anticipation of the grafting procedure, but further adjustments may be made when the final size of the wound defect is known. The late removal of the free graft ensures the greatest preservation of the blood ves- sels of the graft by not subjecting the tissues to the toxic effects of reperfusion injury by excessive exposure to atmospheric oxygen. 2.3. Attachment of the Free Graft to the Surgical Wound After removal of the free graft from the donor site, the graft is immediately placed over the open wound. The umbilical cord is created by a suture placed at the base of the graft which usually consists of dermis and some fat. A second stitch is placed to anchor the graft to the deep fascia or cartilage in such a way that the graft fits snugly over the open surgical wound without tension. However, the graft should not be too loose. Excess skin is trimmed off if necessary. If the graft is considered too large, addi- tional umbilical cord attachments can be applied to an- chor the graft to the floor of the wound. These umbilical cord attachments will not only hold the graft in place in the surgical defect, but will serve as additional sites for revascularization of the graft. Usually 40 vicryl sutures are used for the umbilical cord attachments. 2.4. Suturing the Free Graft to the Margins of the Surgical Defect The graft is attached to the margins of the surgical defect by either 50 or 60 ethilon. Interrupted sutures, 1 - 2 mm apart, are used for close stitching. These sutures are ap- plied closely for hemostasis of the cut edges, and to pre- sent diffusion of atmospheric oxygen to the deep tissues under the graft once the wound is closed. It is important to approximate the cut edges exactly, with mattress su- tures applied if necessary, to prevent “curling” of the epidermis, and avoid “step” differences between the two opposing margins of the wound. The donor site is re- paired using a layered repair technique. 2.5. Wound Care and Suture Removal The wound is dressed with a composite dressing consist- ing of an antibiotic ointment, xeroform, a waterproof outer covering, and flexible tape. The patient is seen the next day for a wound check and the dressing is reapplied if soiled. The patient is asked to avoid aspirin, and to take acetaminophen instead for pain. The patient is also rou- tinely put on cephalexin or alternative drug to minimize infection post-operatively. Usually by the second or third day, no pain is felt with this technique. In addition, infec- tion was not observed in any of the patients described below. The bandages are not changed by the patient but weekly at the clinic. Sutures are removed from the donor site in 2 weeks, and from the graft in 4 weeks. Routinely, the patient is prescribed extra-strength curcumin gel to minimize scarring [8]. 3. Patients and Results 3.1. Patient 1 Patient 1 is a 63-year old Hispanic man who developed a rapidly growing squamous cell carcinoma over his right lower lateral eyelid. This was excised down to the tarsus, with removal of most of his lower eyelid (Figure 1(a)). The wound was closed with a free full-thickness skin graft taken from the donor site over the right temple and zygomatic cheek. The free graft was attached to the from the surface of the graft to the deep tissues of the eye socket using a 40 vicryl suture. This served as an um- bilical cord to revascularize the graft (Figure 1(b)). The graft was attached to the surrounding tissues of the wound with 60 ethilon sutures on three sides (Figure 1(c)). After suture removal, the suture line was treated with extra-strength curcumin gel as previously described [8], with eventual minimal scarring of the surgical inci- sion (Figure 1(d)). 3.2. Patient 2 Patient 2 is a 90-year old man with a history of recurrent baso-squamous cell carcinoma with sclerosing elements despite Moh’s micrographic surgery and repeated cryo- therapy with liquid nitrogen, resulting in the progression of the tumor extending over his nasal tip, right nasal side- wall, right alar nose and nostril edge. The tumor was ex- cised together with the underlying cartilage (Figure 2(a)). A free graft taken from the donor site over the mid fore- head was used to reconstruct his nose (Figure 2(b)), using the umbilical cord technique to enhance revascularization, and close adequate stitching to prevent entry of oxygen into the wounds. Extra-strength curcumin gel was started after the first week and continued until resolution of the residual scarring was achieved (Figures 2(a) and (b)). 3.3. Patient 3 Patient 3 is a 65-year old man with recurrent basal cell Copyright © 2012 SciRes. JCDSA  Utilizing Free Skin Grafts in the Repair of Surgical Wounds 203 (a) (b) (c) (d) Figure 1. Patient 1 with a large squamous cell carcinoma over the right lower eyelid. Following excision of the tumor, the defect was closed with a free full-thickness graft taken from the right temple. The deep surface of the graft was attached to the floor of the excision by a 40 vicryl suture, which serves as an umbilical cord for revascularization of the free graft. Three sides of the graft were attached to the surrounding tissues by 60 ethilon sutures. The donor site was repaired accordingly by a layered repair technique. Fol- lowing removal of the sutures, extra-strength curcumin gel was applied to decrease residual scarring. (a) (b) Copyright © 2012 SciRes. JCDSA 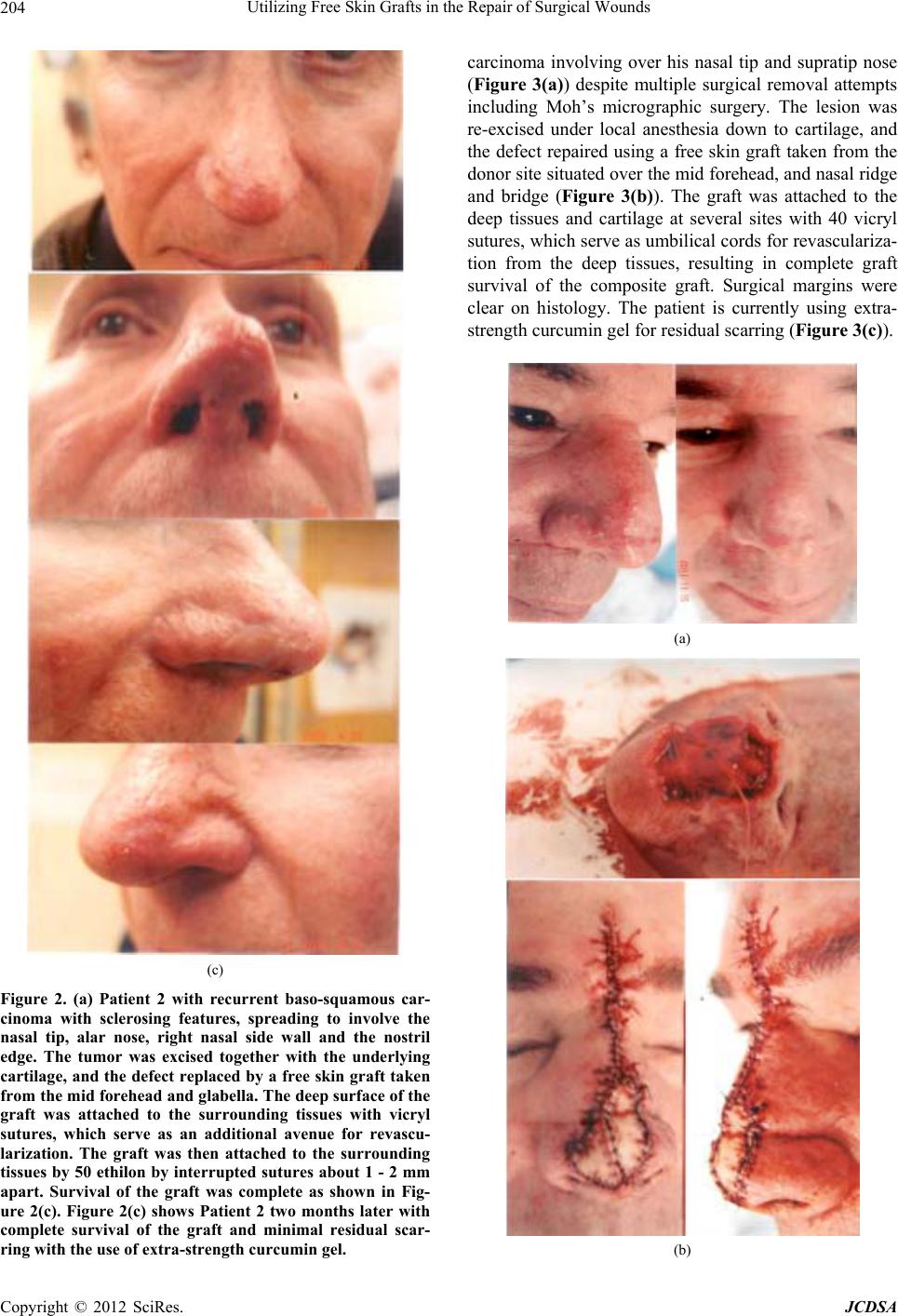 Utilizing Free Skin Grafts in the Repair of Surgical Wounds 204 (c) Figure 2. (a) Patient 2 with recurrent baso-squamous car- cinoma with sclerosing features, spreading to involve the nasal tip, alar nose, right nasal side wall and the nostril edge. The tumor was excised together with the underlying cartilage, and the defect replaced by a free skin graft taken from the mid forehead and glabella. The deep surface of the graft was attached to the surrounding tissues with vicryl sutures, which serve as an additional avenue for revascu- larization. The graft was then attached to the surrounding tissues by 50 ethilon by interrupted sutures about 1 - 2 mm apart. Survival of the graft was complete as shown in Fig- ure 2(c). Figure 2(c) shows Patient 2 two months later with complete survival of the graft and minimal residual scar- ring with the use of extra-strength curcumin gel. carcinoma involving over his nasal tip and supratip nose (Figure 3(a)) despite multiple surgical removal attempts including Moh’s micrographic surgery. The lesion was re-excised under local anesthesia down to cartilage, and the defect repaired using a free skin graft taken from the donor site situated over the mid forehead, and nasal ridge and bridge (Figure 3(b)). The graft was attached to the deep tissues and cartilage at several sites with 40 vicryl sutures, which serve as umbilical cords for revasculariza- tion from the deep tissues, resulting in complete graft survival of the composite graft. Surgical margins were clear on histology. The patient is currently using extra- strength curcumin gel for residual scarring (Figure 3(c)). (a) (b) Copyright © 2012 SciRes. JCDSA  Utilizing Free Skin Grafts in the Repair of Surgical Wounds 205 (c) Figure 3. (a) and (b) show Patient 3 with recurrent basal cell carcinoma following multiple Moh’s micrographic sur- gical procedures. The tumor was excised down to cartilage, and the defect closed with a composite free graft taken from the mid nasal ridge, glabella and mid forehead. The grafts were attached to the nasal cartilage by 40 vicryl sutures, which serve as umbilical cords that provide additional ave- nues for neovascularization of the free grafts. The grafts were attached to the surrounding tissues by 50 and 60 e- thilon sutures. The donor site was repaired accordingly with a layered repair technique. (c) shows Patient 3 with com- plete survival of the composite graft 2 months later. Resid- ual scarring is minimized with the use of extra-strength curcumin gel. 3.4. Patient 4 Patient 4 is a 92-year old female with a large baso-squa- mous cell carcinoma situated over the right nasal side wall. Following excision of the tumor, the defect was partially closed with a rotation flap. The remaining defect was closed with a full-thickness free skin graft taken from the donor site situated over the glabella forehead (Figure 4(a)). The deep surface of the graft was anchored to the deep tissues by a 40 vicryl suture, which served as an umbilical cord for revascularization of the graft. The sutures from the donor site were removed in 2 weeks and from the graft itself in 4 weeks. Following suture re- moval, the incision was treated with applications of ex- tra-strength curcumin gel twice daily, with resolution of the remaining scar tissue. A return of sensation in the graft was observed by the patient within 6 months. 3.5. Patient 5 Patient 5 is an 89-year old man with a squamous cell carcinoma situated over his left anterior pinna ear (Fig- ure 5). The tumor was excised down to and including the underlying cartilage, and the wound was closed with a free graft taken from the donor site situated over the left post-auricular neck. The graft was attached to the deep tissues using an umbilical cord consisting of a 40 vicryl suture between the deep tissues of the graft and the floor of the wound. The graft was then stitched in place with 60 ethilon sutures. The stitches were removed from the donor site after 2 weeks, and from the graft after 4 weeks. Extra-strength curcumin gel was used to minimize resid- ual scarring. A return of sensation in the graft was noted by the patient within 6 months. 3.6. Patient 6 Patient 6 is a 72-year old man with a large squamous cell carcinoma over his right superior and posterior pinna ear (Figure 6). The tumor was excised down to the cartilage and the defect closed with a free graft taken from his right post-auricular neck. The graft was attached to the cartilage using a 40 vicryl suture using the umbilical cord technique. The graft was stitched to the surrounding tis- sues with 60 interrupted sutures. Following suture re- moval in 4 weeks, extra-strength curcumin gel was used to remove residual scarring. In addition, sensation was observed to be partially restored to the graft within 6 months. 3.7. Patient 7 Patient 7 is a 76-year old female patient with squamous cell carcinoma over two thirds of her ring finger (Figure 7(a)). The tumor was excised down to deep fascia and the defect closed using a free graft taken from the donor Copyright © 2012 SciRes. JCDSA 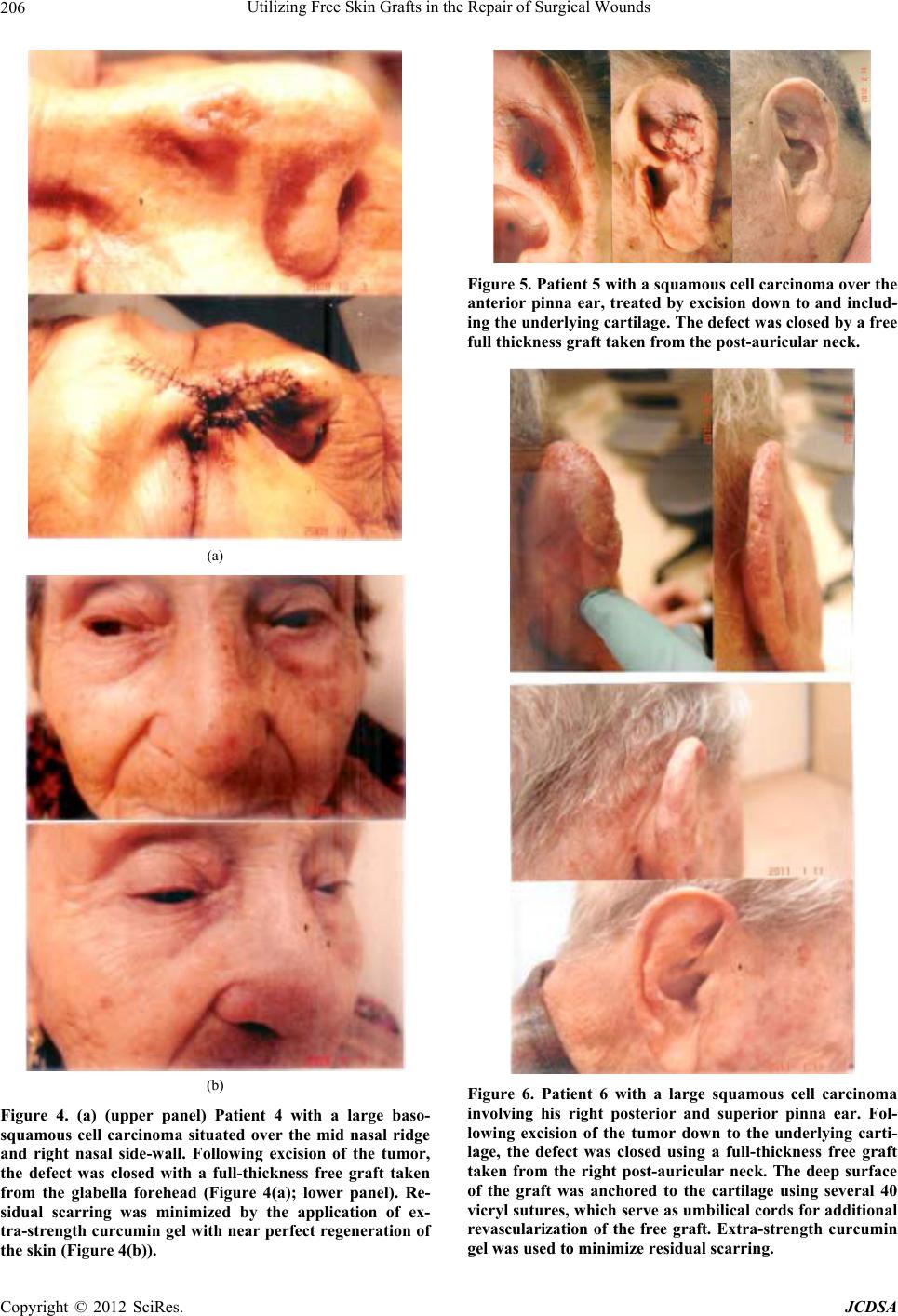 Utilizing Free Skin Grafts in the Repair of Surgical Wounds 206 (a) (b) Figure 4. (a) (upper panel) Patient 4 with a large baso- squamous cell carcinoma situated over the mid nasal ridge and right nasal side-wall. Following excision of the tumor, the defect was closed with a full-thickness free graft taken from the glabella forehead (Figure 4(a); lower panel). Re- sidual scarring was minimized by the application of ex- tra-strength curcumin gel with near perfect regeneration of the skin (Figure 4(b)). Figure 5. Patient 5 with a squamous cell carcinoma over the anterior pinna ear, treated by excision down to and includ- ing the underlying cartilage. The defect was closed by a free full thickness graft taken from the post-auricular neck. Figure 6. Patient 6 with a large squamous cell carcinoma involving his right posterior and superior pinna ear. Fol- lowing excision of the tumor down to the underlying carti- lage, the defect was closed using a full-thickness free graft taken from the right post-auricular neck. The deep surface of the graft was anchored to the cartilage using several 40 vicryl sutures, which serve as umbilical cords for additional revascularization of the free graft. Extra-strength curcumin gel was used to minimize residual scarring. Copyright © 2012 SciRes. JCDSA 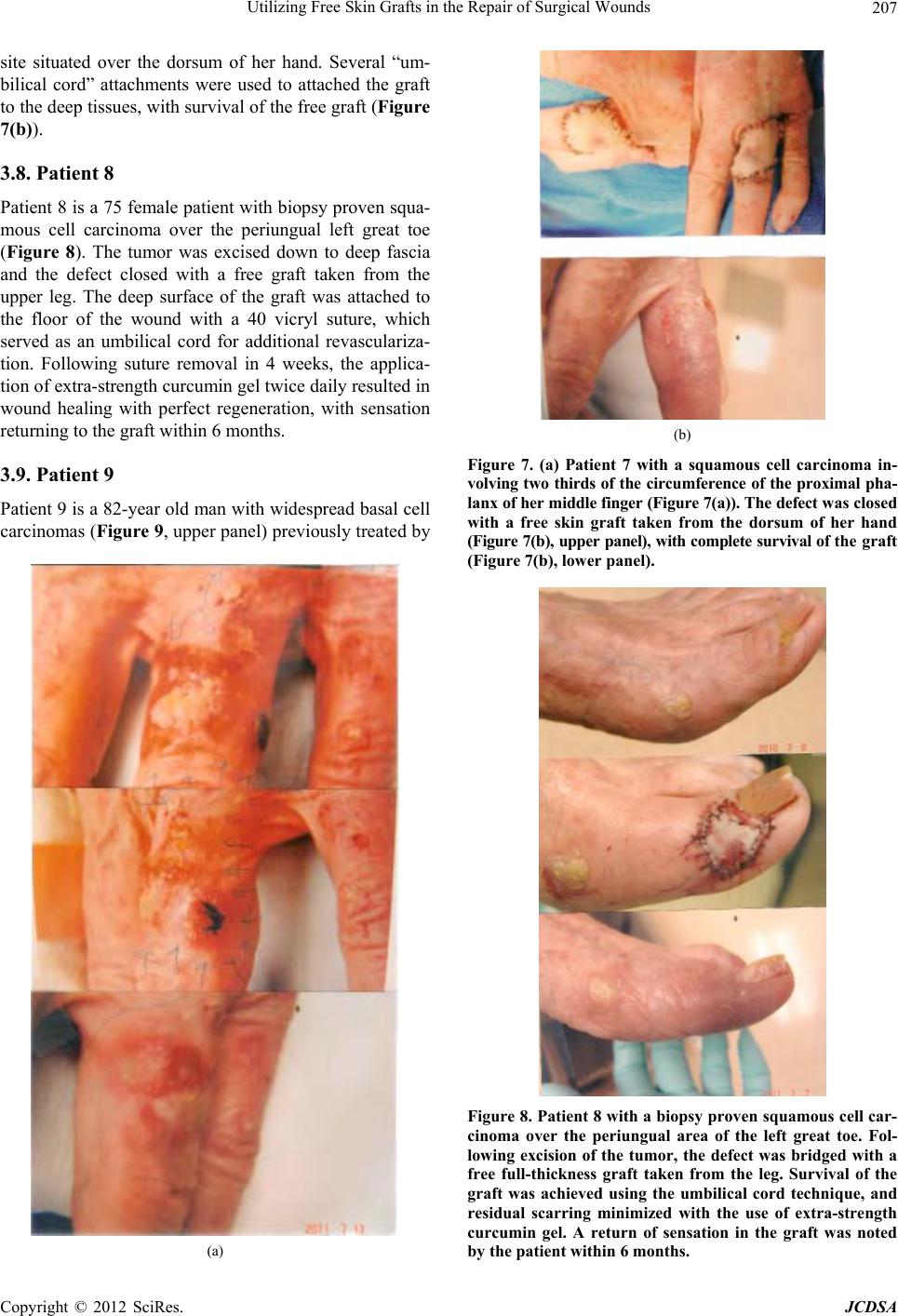 Utilizing Free Skin Grafts in the Repair of Surgical Wounds 207 site situated over the dorsum of her hand. Several “um- bilical cord” attachments were used to attached the graft to the deep tissues, with survival of the free graft (Figure 7(b)). 3.8. Patient 8 Patient 8 is a 75 female patient with biopsy proven squa- mous cell carcinoma over the periungual left great toe (Figure 8). The tumor was excised down to deep fascia and the defect closed with a free graft taken from the upper leg. The deep surface of the graft was attached to the floor of the wound with a 40 vicryl suture, which served as an umbilical cord for additional revasculariza- tion. Following suture removal in 4 weeks, the applica- tion of extra-strength curcumin gel twice daily resulted in wound healing with perfect regeneration, with sensation returning to the graft within 6 months. 3.9. Patient 9 Patient 9 is a 82-year old man with widespread basal cell carcinomas (Figure 9, upper panel) previously treated by (a) (b) Figure 7. (a) Patient 7 with a squamous cell carcinoma in- volving two thirds of the circumference of the proximal pha- lanx of her middle finger (Figure 7(a)). The defect was closed with a free skin graft taken from the dorsum of her hand (Figure 7(b), upper panel), with complete survival of the graft (Figure 7(b), lower panel). Figure 8. Patient 8 with a biopsy proven squamous cell car- cinoma over the periungual area of the left great toe. Fol- lowing excision of the tumor, the defect was bridged with a free full-thickness graft taken from the leg. Survival of the graft was achieved using the umbilical cord technique, and residual scarring minimized with the use of extra-strength curcumin gel. A return of sensation in the graft was noted by the patient within 6 months. Copyright © 2012 SciRes. JCDSA 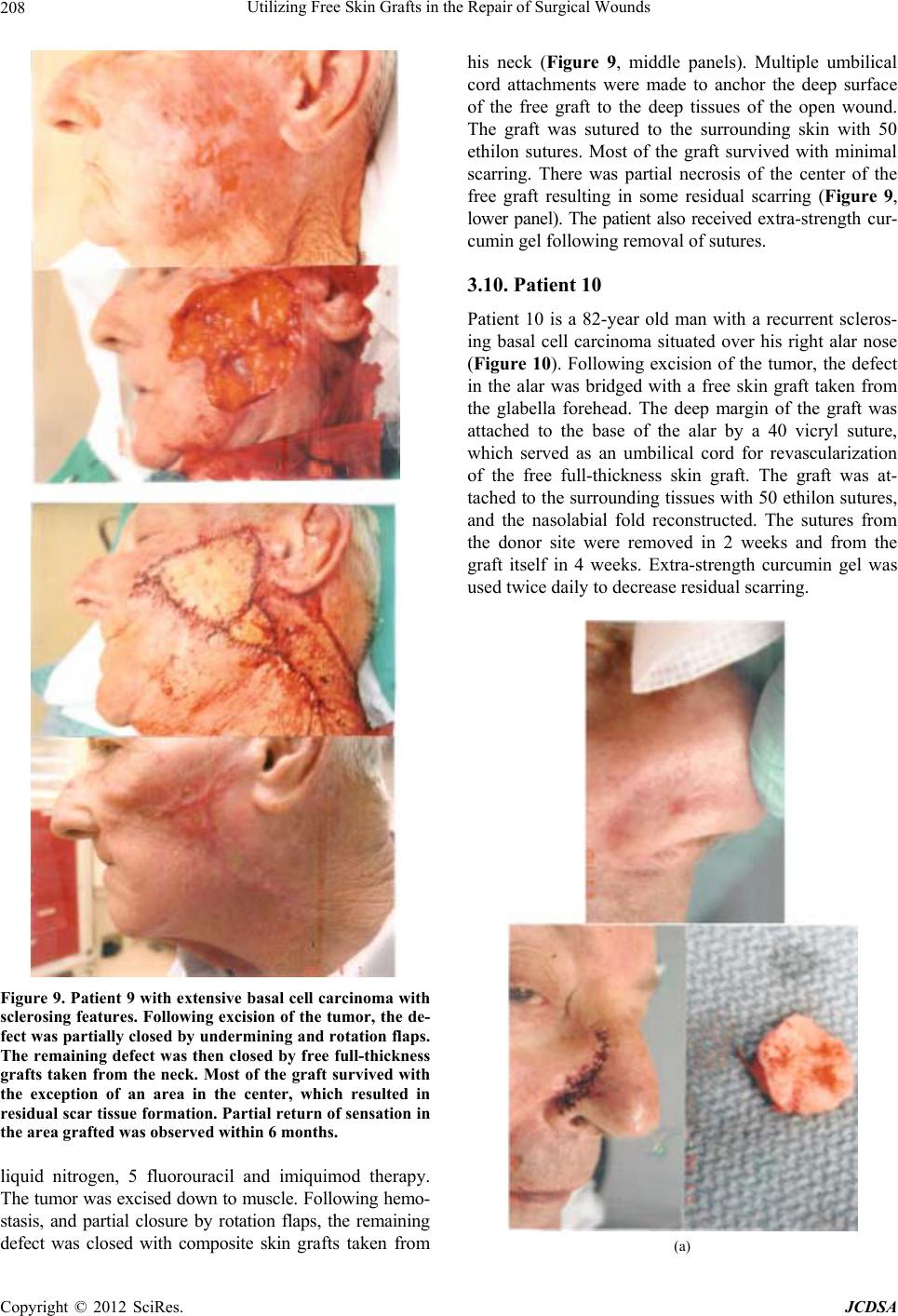 Utilizing Free Skin Grafts in the Repair of Surgical Wounds 208 Figure 9. Patient 9 with extensive basal cell carcinoma with sclerosing features. Following excision of the tumor, the de- fect was partially closed by undermining and rotation flaps. The remaining defect was then closed by free full-thickness grafts taken from the neck. Most of the graft survived with the exception of an area in the center, which resulted in residual scar tissue formation. Partial return of sensation in the area grafted was observed within 6 months. liquid nitrogen, 5 fluorouracil and imiquimod therapy. The tumor was excised down to muscle. Following hemo- stasis, and partial closure by rotation flaps, the remaining defect was closed with composite skin grafts taken from his neck (Figure 9, middle panels). Multiple umbilical cord attachments were made to anchor the deep surface of the free graft to the deep tissues of the open wound. The graft was sutured to the surrounding skin with 50 ethilon sutures. Most of the graft survived with minimal scarring. There was partial necrosis of the center of the free graft resulting in some residual scarring (Figure 9, lower panel). The patient also received extra-strength cur- cumin gel following removal of sutures. 3.10. Patient 10 Patient 10 is a 82-year old man with a recurrent scleros- ing basal cell carcinoma situated over his right alar nose (Figure 10). Following excision of the tumor, the defect in the alar was bridged with a free skin graft taken from the glabella forehead. The deep margin of the graft was attached to the base of the alar by a 40 vicryl suture, which served as an umbilical cord for revascularization of the free full-thickness skin graft. The graft was at- tached to the surrounding tissues with 50 ethilon sutures, and the nasolabial fold reconstructed. The sutures from the donor site were removed in 2 weeks and from the graft itself in 4 weeks. Extra-strength curcumin gel was used twice daily to decrease residual scarring. (a) Copyright © 2012 SciRes. JCDSA 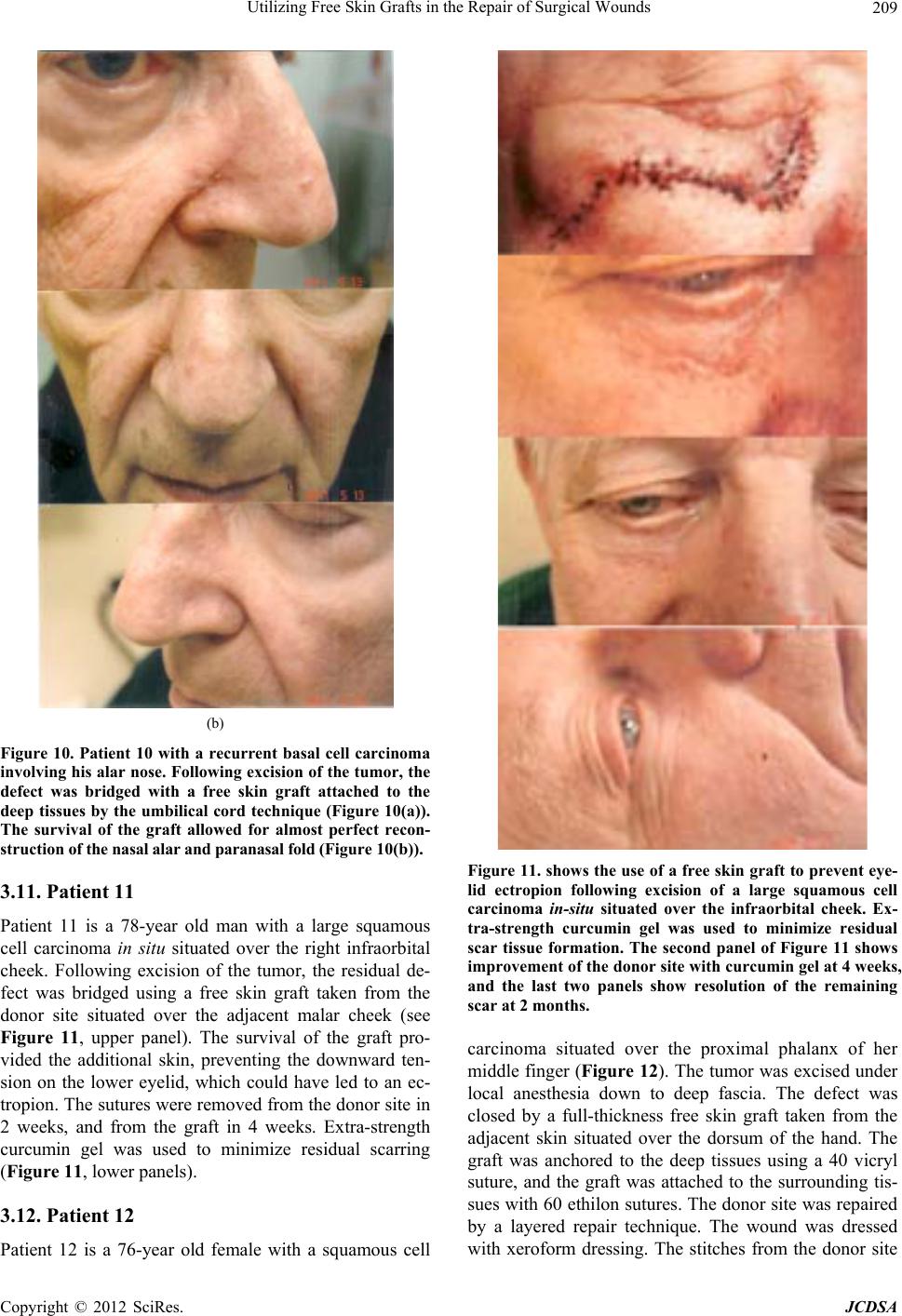 Utilizing Free Skin Grafts in the Repair of Surgical Wounds 209 (b) Figure 10. Patient 10 with a recurrent basal cell carcinoma involving his alar nose. Following excision of the tumor, the defect was bridged with a free skin graft attached to the deep tissues by the umbilical cord technique (Figure 10(a)). The survival of the graft allowed for almost perfect recon- struction of the nasal alar and paranasal fold (Figure 10(b)). 3.11. Patient 11 Patient 11 is a 78-year old man with a large squamous cell carcinoma in situ situated over the right infraorbital cheek. Following excision of the tumor, the residual de- fect was bridged using a free skin graft taken from the donor site situated over the adjacent malar cheek (see Figure 11, upper panel). The survival of the graft pro- vided the additional skin, preventing the downward ten- sion on the lower eyelid, which could have led to an ec- tropion. The sutures were removed from the donor site in 2 weeks, and from the graft in 4 weeks. Extra-strength curcumin gel was used to minimize residual scarring (Figure 11, lower panels). 3.12. Patient 12 Patient 12 is a 76-year old female with a squamous cell Figure 11. shows the use of a free skin graft to prevent eye- lid ectropion following excision of a large squamous cell carcinoma in-situ situated over the infraorbital cheek. Ex- tra-strength curcumin gel was used to minimize residual scar tissue formation. The second panel of Figure 11 shows improvement of the donor site with curcumin gel at 4 weeks, and the last two panels show resolution of the remaining scar at 2 months. carcinoma situated over the proximal phalanx of her middle finger (Figure 12). The tumor was excised under local anesthesia down to deep fascia. The defect was closed by a full-thickness free skin graft taken from the adjacent skin situated over the dorsum of the hand. The graft was anchored to the deep tissues using a 40 vicryl suture, and the graft was attached to the surrounding tis- sues with 60 ethilon sutures. The donor site was repaired by a layered repair technique. The wound was dressed with xeroform dressing. The stitches from the donor site Copyright © 2012 SciRes. JCDSA  Utilizing Free Skin Grafts in the Repair of Surgical Wounds 210 Figure 12. (upper panel) Patient 12 with a squamous cell carcinoma situated over the dorsum of the proximal pha- lanx of her middle finger. Following excision of the tumor, the defect was closed with a full thickness free skin graft taken from the adjacent skin over the dorsum of the hand (Figure 12, middle panel). The graft was anchored to the deep tissues using the umbilical cord technique, with sur- vival of the graft (Figure 12, lower panel). The patient re- ported return of sensation in the graft within 6 months. were removed in 2 weeks, and from the graft in 4 weeks. Extra-strength curcumin gel was applied twice daily to mi- nimize the residual scarring. 4. Discussion In this paper, we describe the use of full-thickness free skin grafts to repair defects in wounds following surgical excisions for tumors. The survival of the free grafts af- forded the essential skin required for the repair of eyelids (Patients 1 and 11), noses, including loss of skin over the nasal alar (Figure 10), nostril edge and underlying carti- lage (Patient 2), nasal tip and supratip nose (Patient 3), nasal side wall (Patient 4), pinna ears (Patients 5 and 6), fingers and toes (Patients 7, 8 and 12). In addition, the free skin graft technique can be used to close fairly large defects on the face, which are greater than 9 cm in size (Figure 9). The advantages of free skin grafts include the follow- ing: 1) Closure of the wound at the time of the surgery; 2) Decrease risk of infection since none of the grafts in our patients became infected; 3) Minimal complaints of pain; 4) Excellent cosmetic result, particularly when curcumin gel [8] is added for scar prevention; and 5) Restoration of sensation in the graft, usually within 6 months. Perhaps the greatest asset of the free graft technique is its sim- plicity. The procedure is relatively simple and may be easily used by dermatologists, with the procedure per- formed under local anesthesia in an out-patient clinic setting. By contrast, the pedicle grafts performed by plas- tic surgery with underlying muscle and sometimes, bone, require general anesthesia and hospitalization. In addition, with the free skin grafts, trauma to the tissues, and blood loss are minimal in all cases, and complications, such as those reported with the pedicle grafts, such as arterial and venous thrombosis [9,10], hematoma formation [9,10], infection [9], and failed flaps with necrosis [6], were not seen in our patients. Although free grafts have been used both by plastic surgeons and dermatologists for many years, their failure to survive is the main reason for simple free skin grafts falling into disrepute. Adequate perfusion [9,10] and re- vascularization [11] of the flaps is considered a major factor contributing to flap survival. Because all our free grafts survived without developing necrosis, with the exception of partial necrosis in the center of the ex- tremely large graft in patient 9, we believe that revascu- larization of our free grafts is the main reason for our high graft survival rate. It is also believed that our tech- nique of providing umbilical cord insertions from the deep surface of the graft may have contributed to the survival of the free grafts. In addition, our technique of minimizing the time between excision of the graft from the donor site and placement of the graft in the surgical defect may also contribute to the survival of the free grafts. Furthermore, the closure of the wound by our close stitching technique, which helps prevent the entry of atmospheric oxygen into the wound, may also be im- portant, since reperfusion injury [12], with its attendant release of free radicals, may be detrimental to graft sur- vival. It must be pointed out that our technique of close stitching, by preventing the entry of oxygen into the wound, maintains a state of hypoxia in the tissues of the graft. This is an important issue, since hypoxia is consid- ered to be the most potent stimulus for new blood vessel formation following injury [12]. In summary, we report the technical aspects of the use of full-thickness free skin grafts for repair of defects fol- lowing excisions of skin cancers. These patients are ex- Copyright © 2012 SciRes. JCDSA  Utilizing Free Skin Grafts in the Repair of Surgical Wounds Copyright © 2012 SciRes. JCDSA 211 amples that demonstrate the locations and size of the grafts that may be used without loss of graft survival. The cosmetic results are excellent and restoration of sen- sation in the graft is usually observed within 6 months. REFERENCES [1] F. J. Menick, “A 10-Year Experience in Nasal Recon- struction with the Three-Stage Forehead Flap,” Plastic Reconstructive Surgery, Vol. 109, No. 6, 2002, pp. 1839- 1855. doi:10.1097/00006534-200205000-00010 [2] F. J. Menick and A. Salibian, “Microvascular Repair of Heminasal, Subtotal, and Total Nasal Defects with a Folded Radial Forearm Flap and a Full-Thickness Fore- head Flap,” Plastic Reconstructive Surgery, Vol. 127, No. 2, 2011, pp. 637-651. doi:10.1097/PRS.0b013e3181fed686 [3] C. H. Wong, L. C. Teoh, J. Y. Lee, A. K. Yam, D. B. Khoo and F. C. Yong, “Free Digital Artery Flap: An Ideal Flap for Large Finger Defects in Situations Where Local Flaps Are Precluded,” Annals of Plastic Surgery, Vol. 60, No. 3, 2008, pp. 254-259. doi:10.1097/SAP.0b013e318061b7b0 [4] T. P. Lee, C. Y. Liao, I. C. Wu, C. C. Yu and S. G. Chen, “Free Flap from the Superficial Palmar Branch of the Ra- dial Artery (SPBRA Flap) for Finger Reconstruction,” Trauma, Vol. 66, No. 4, 2009, pp. 1173-1179. doi:10.1097/TA.0b013e31816a4eb7 [5] J. L. Orbay, J. G. Rosen, R. K. Khouri and I. Indriago, “The Glabrous Palmar Flap: The New Free or Reversed Pedicled Palmar Fasciocutaneous Flap for Volar Hand Reconstruction,” Techniques in Hand and Upper Extrem- ity Surgery, Vol. 13, No. 3, 2009, pp. 145-150. doi:10.1097/BTH.0b013e3181ac9183 [6] M. Tremp, R. Wettstein, W. Raffoul, D. J. Shaefer and D. F. Kalbermatten, “Secret Scar Free Gracilis Flap,” Jour- nal of Reconstructive Microsurgery, 15 May 2012 (Epub Ahead of Print). [7] A. J. Organek, M. J. Klebuc and R. M. Zuker, “Indica- tions and Outcomes of Free Tissue Transfer to the Lower Extremity in Children: A Review,” Journal of Recon- structive Microsurgery, Vol. 22, No. 3, 2006, pp. 173- 181. doi:10.1055/s-2006-939963 [8] M. C. Heng, “Wound Healing in Adult Skin: Aiming for Perfect Regeneration,” International Journal of Derma- tology, Vol. 50, No. 9, 2011, pp. 1058-1066. doi:10.1111/j.1365-4632.2011.04940.x [9] H. G. Machens, P. Mailaender, J. Pasel, B. S. Lutz, M. Funke, F Siemers, et al., “Flap Perfusion after Free Mus- culocutaneous Tissue Transfer: The Impact of Postopera- tive Complications,” Plastic Reconstructive Surgery, Vol. 105, No. 7, 2000, pp. 2395-2399. doi:10.1097/00006534-200006000-00013 [10] H. G. Machens, P. Mailaender, R. Reimer, N. Pallua, Y. Lei and A. Berger, “Post-Operative Blood Flow by Mens of the Hydrogen Clearance Technique,” Plastic Recon- structive Surgery, Vol. 99, No. 2, 1997, pp. 493-505. doi:10.1097/00006534-199702000-00027 [11] N. Lindenblatt, U. Platz, M. Althaus, N. Hegland, C. A. Schmidt, C. Contaldo, et al., “Temporary Antiogenic Trans- formation of the Skin Graft Vasculature after Reperfu- sion,” Plastic Reconstructive Surgery, Vol. 126, No. 1, 2010, pp. 61-70. doi:10.1097/PRS.0b013e3181da87f6 [12] M. C. Heng, J. Harker, G. Csathy, C. Marshall, J. Brazier, S. Sumampong, et al., “Angiogenesis in Necrotic Ulcers Treated with Hyperbaric Oxygen,” Ostomy/Wound Man- agement, Vol. 46, No. 9, 2000, pp. 18-32.
|