Lifa Disease: Frictional Dermal Melanosis over Bony Prominences (Clinicopathological Study) 197
All patients had clinical features of lifa disease that
characterized by rippled, spotty, or confluent macular hy-
per-pigmentation over the superficial bony prominences
with bilateral and symmetrical distribution.
The patients were questioned regarding the: Age, sex,
site of the lesions, age of onset and duration, presence of
itching, presence of friction, duration and type of friction
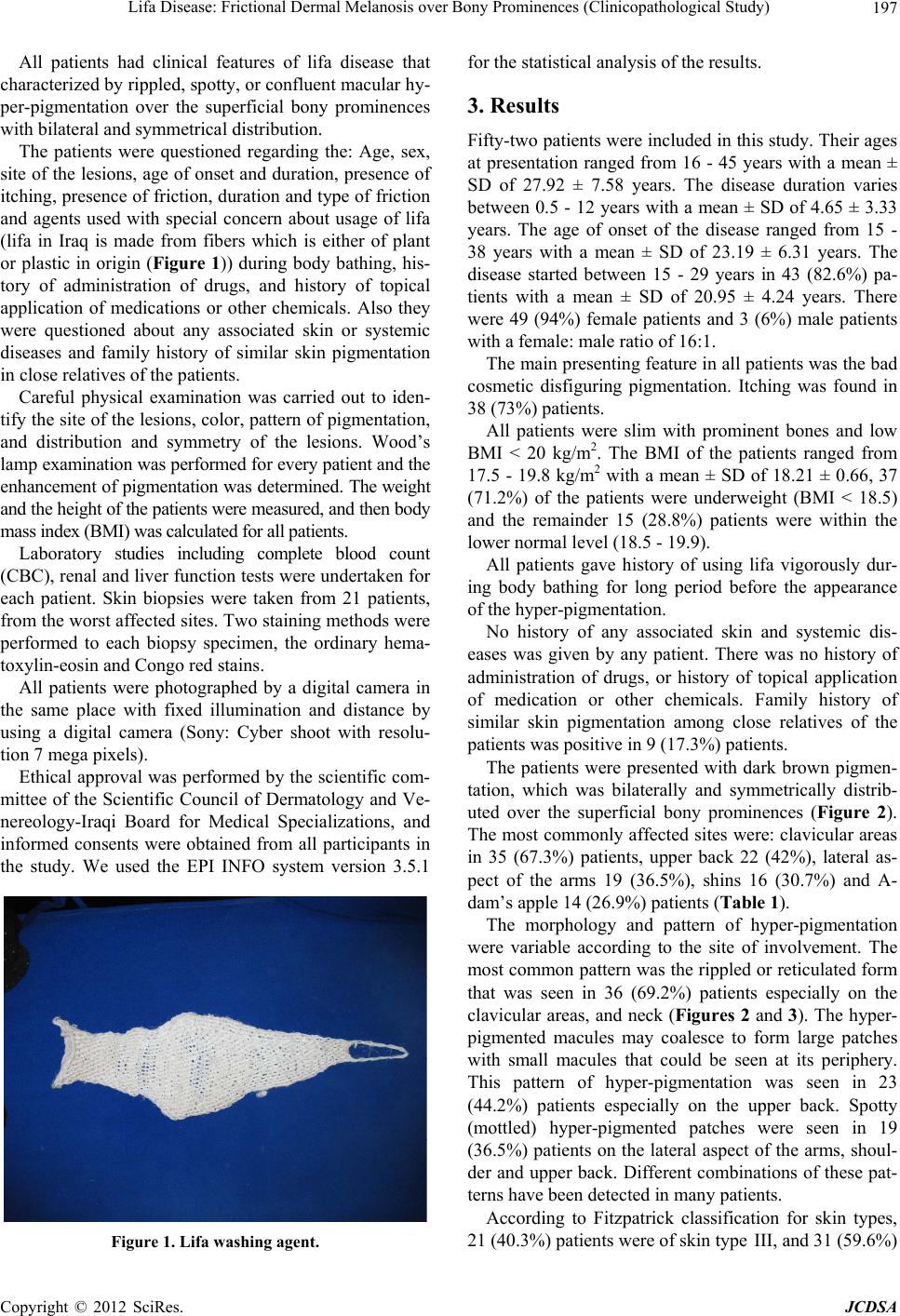
and agents used with special concern about usage of lifa
(lifa in Iraq is made from fibers which is either of plant
or plastic in origin (Figure 1)) during body bathing, his-
tory of administration of drugs, and history of topical
application of medications or other chemicals. Also they
were questioned about any associated skin or systemic
diseases and family history of similar skin pigmentation
in close relatives of the patients.
Careful physical examination was carried out to iden-
tify the site of the lesions, color, pattern of pigmentation,
and distribution and symmetry of the lesions. Wood’s
lamp examination was performed for every patient and the
enhancement of pigmentation was determined. The weight
and the height of the patients were measured, and then body
mass index (BMI) was calculated for all patients.
Laboratory studies including complete blood count
(CBC), renal and liver function tests were undertaken for
each patient. Skin biopsies were taken from 21 patients,
from the worst affected sites. Two staining methods were
performed to each biopsy specimen, the ordinary hema-
toxylin-eosin and Congo red stains.
All patients were photographed by a digital camera in
the same place with fixed illumination and distance by
using a digital camera (Sony: Cyber shoot with resolu-
tion 7 mega pixels).
Ethical approval was performed by the scientific com-
mittee of the Scientific Council of Dermatology and Ve-
nereology-Iraqi Board for Medical Specializations, and
informed consents were obtained from all participants in
the study. We used the EPI INFO system version 3.5.1
Figure 1. Lifa washing agent.
for the statistical analysis of the results.
3. Results
Fifty-two patients were included in this study. Their ages
at presentation ranged from 16 - 45 years with a mean ±
SD of 27.92 ± 7.58 years. The disease duration varies
between 0.5 - 12 years with a mean ± SD of 4.65 ± 3.33
years. The age of onset of the disease ranged from 15 -
38 years with a mean ± SD of 23.19 ± 6.31 years. The
disease started between 15 - 29 years in 43 (82.6%) pa-
tients with a mean ± SD of 20.95 ± 4.24 years. There
were 49 (94%) female patients and 3 (6%) male patients
with a female: male ratio of 16:1.
The main presenting feature in all patients was the bad
cosmetic disfiguring pigmentation. Itching was found in
38 (73%) patients.
All patients were slim with prominent bones and low
BMI < 20 kg/m2. The BMI of the patients ranged from
17.5 - 19.8 kg/m2 with a mean ± SD of 18.21 ± 0.66, 37
(71.2%) of the patients were underweight (BMI < 18.5)
and the remainder 15 (28.8%) patients were within the
lower normal level (18.5 - 19.9).
All patients gave history of using lifa vigorously dur-
ing body bathing for long period before the appearance
of the hyper-pigmentation.
No history of any associated skin and systemic dis-
eases was given by any patient. There was no history of
administration of drugs, or history of topical application
of medication or other chemicals. Family history of
similar skin pigmentation among close relatives of the
patients was positive in 9 (17.3%) patients.
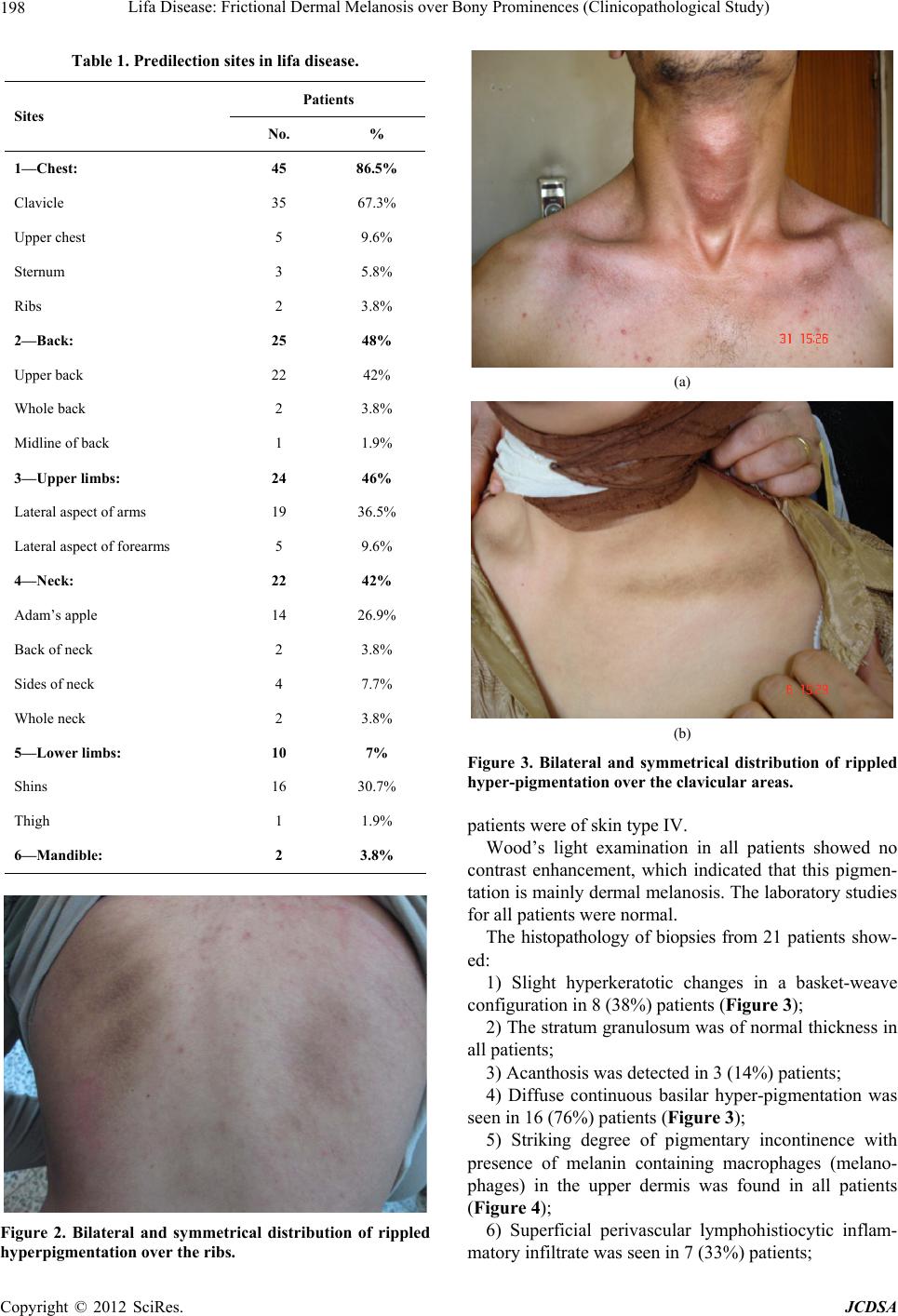
The patients were presented with dark brown pigmen-
tation, which was bilaterally and symmetrically distrib-
uted over the superficial bony prominences (Figure 2).
The most commonly affected sites were: clavicular areas
in 35 (67.3%) patients, upper back 22 (42%), lateral as-
pect of the arms 19 (36.5%), shins 16 (30.7%) and A-
dam’s apple 14 (26.9%) patients (Table 1).
The morphology and pattern of hyper-pigmentation
were variable according to the site of involvement. The
most common pattern was the rippled or reticulated form
that was seen in 36 (69.2%) patients especially on the
clavicular areas, and neck (Figures 2 and 3). The hyper-
pigmented macules may coalesce to form large patches
with small macules that could be seen at its periphery.
This pattern of hyper-pigmentation was seen in 23
(44.2%) patients especially on the upper back. Spotty
(mottled) hyper-pigmented patches were seen in 19
(36.5%) patients on the lateral aspect of the arms, shoul-
der and upper back. Different combinations of these pat-
terns have been detected in many patients.
According to Fitzpatrick classification for skin types,
21 (40.3%) patients were of skin type III, and 31 (59.6%)
Copyright © 2012 SciRes. JCDSA