A Unique Case? Darier’s Disease Presented as Porcupine-Like Appearance and the Observation on Acitretin Treatment 139
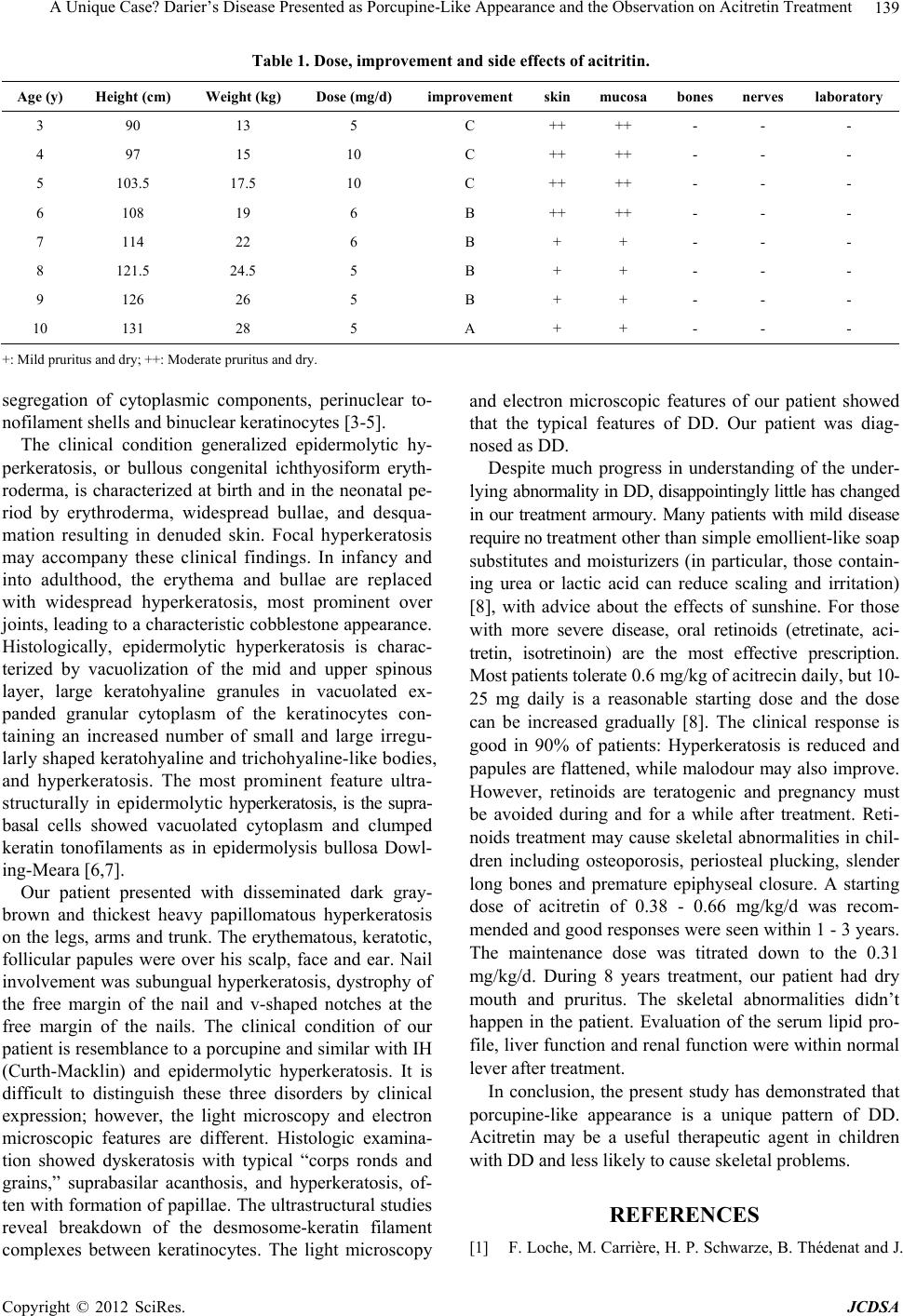
Table 1. Dose, improvement and side effects of acitritin.
Age (y) Height (cm) Weight (kg) Dose (mg/d) improvement skinmucosa bones nerves laboratory
3 90 13 5 C ++ ++ - - -
4 97 15 10 C ++ ++ - - -
5 103.5 17.5 10 C ++ ++ - - -
6 108 19 6 B ++ ++ - - -
7 114 22 6 B + + - - -
8 121.5 24.5 5 B + + - - -
9 126 26 5 B + + - - -
10 131 28 5 A + + - - -
+: Mild pruritus and dry; ++: Moderate pruritus and dry.
segregation of cytoplasmic components, perinuclear to-
nofilament shells and binuclear keratinocytes [3-5].
The clinical condition generalized epidermolytic hy-
perkeratosis, or bullous congenital ichthyosiform eryth-
roderma, is characterized at birth and in the neonatal pe-
riod by erythroderma, widespread bullae, and desqua-
mation resulting in denuded skin. Focal hyperkeratosis
may accompany these clinical findings. In infancy and
into adulthood, the erythema and bullae are replaced
with widespread hyperkeratosis, most prominent over
joints, leading to a characteristic cobblestone appearance.
Histologically, epidermolytic hyperkeratosis is charac-
terized by vacuolization of the mid and upper spinous
layer, large keratohyaline granules in vacuolated ex-
panded granular cytoplasm of the keratinocytes con-
taining an increased number of small and large irregu-
larly shaped keratohyaline and trichohyaline-like bodies,
and hyperkeratosis. The most prominent feature ultra-
structurally in epidermolytic hyperkeratosis, is the supra-
basal cells showed vacuolated cytoplasm and clumped
keratin tonofilaments as in epidermolysis bullosa Dowl-
ing-Meara [6,7].
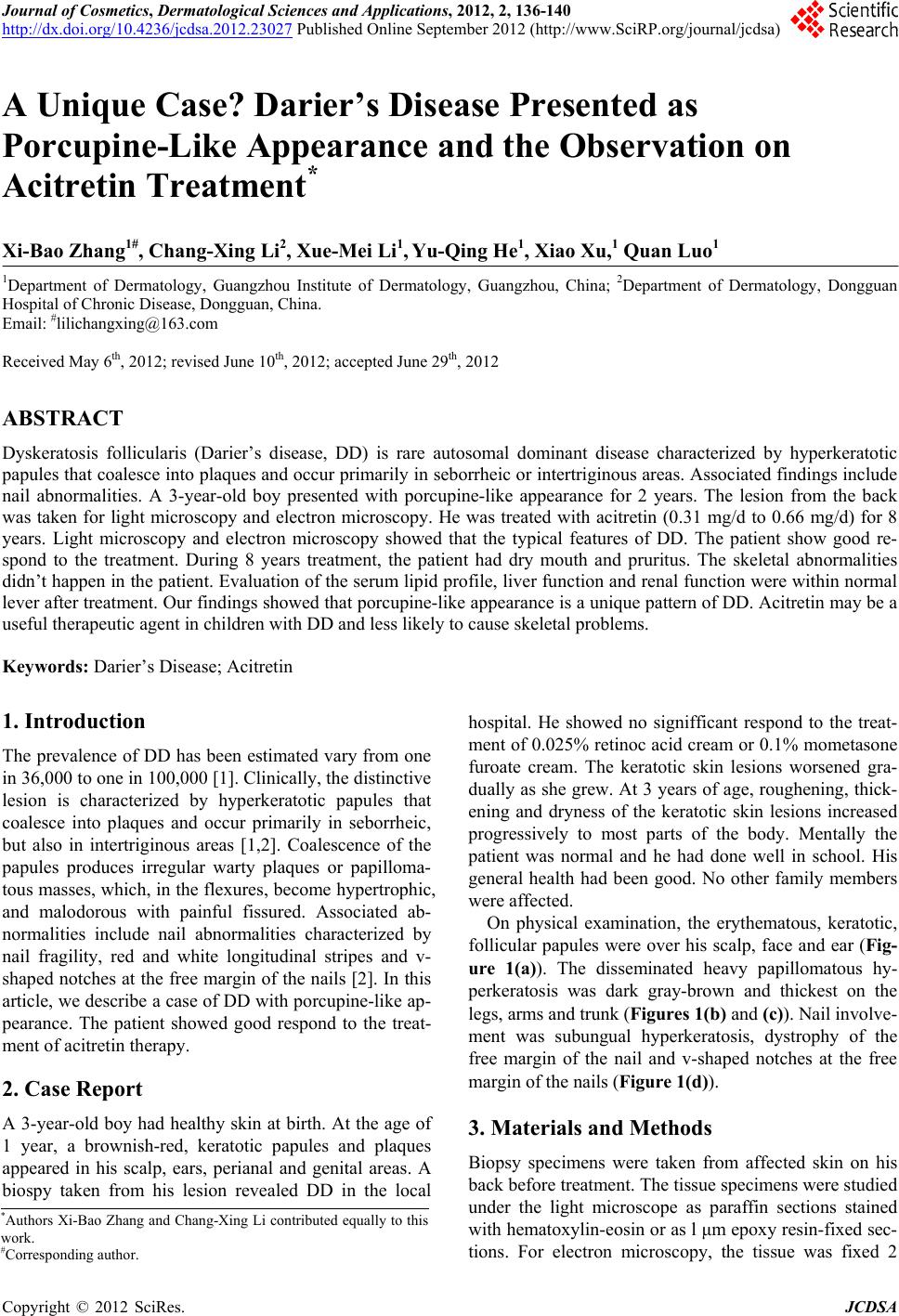
Our patient presented with disseminated dark gray-
brown and thickest heavy papillomatous hyperkeratosis
on the legs, arms and trunk. The erythematous, keratotic,
follicular papules were over his scalp, face and ear. Nail
involvement was subungual hyperkeratosis, dystrophy of
the free margin of the nail and v-shaped notches at the
free margin of the nails. The clinical condition of our
patient is resemblance to a porcupine and similar with IH
(Curth-Macklin) and epidermolytic hyperkeratosis. It is
difficult to distinguish these three disorders by clinical
expression; however, the light microscopy and electron
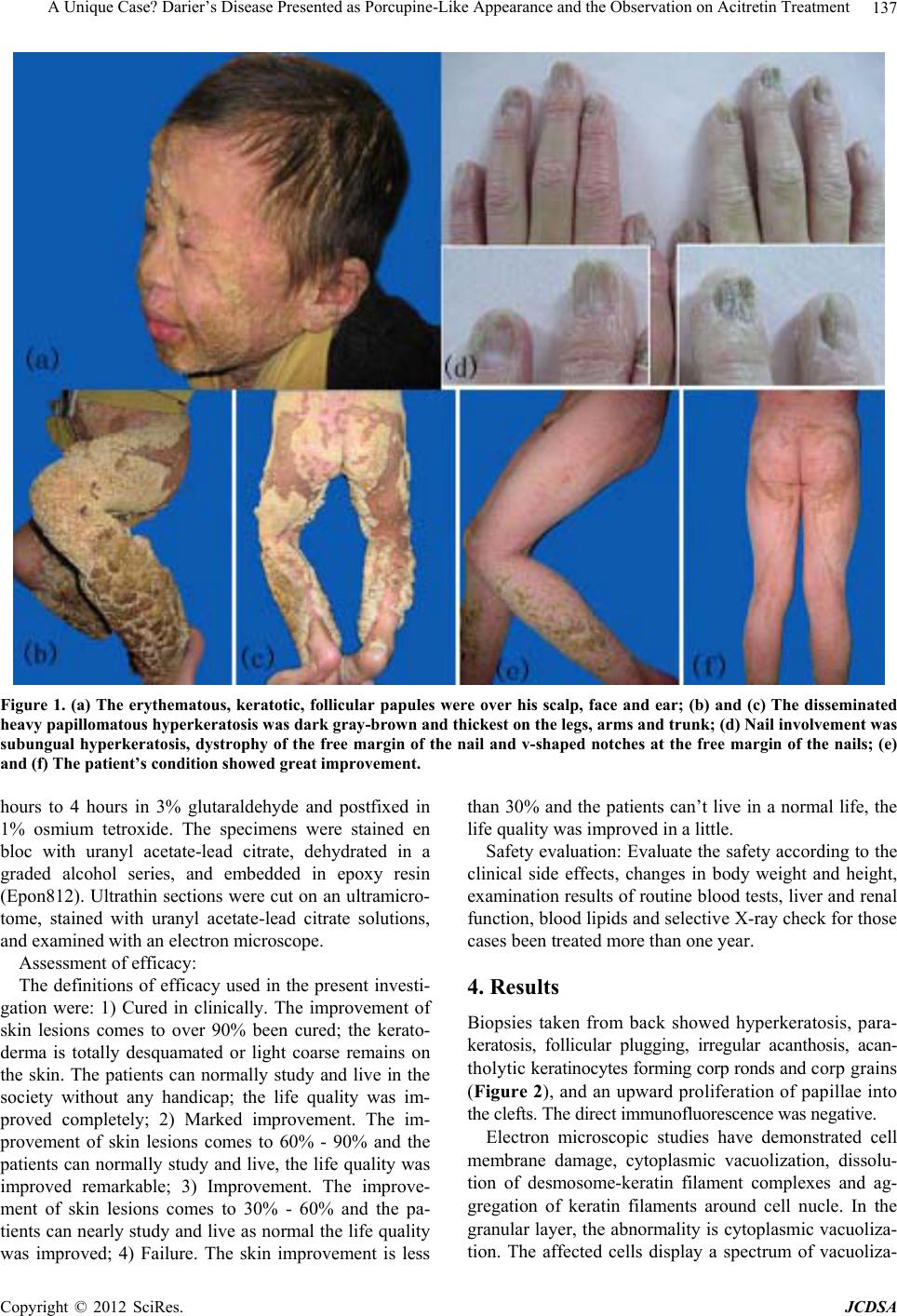
microscopic features are different. Histologic examina-
tion showed dyskeratosis with typical “corps ronds and
grains,” suprabasilar acanthosis, and hyperkeratosis, of-
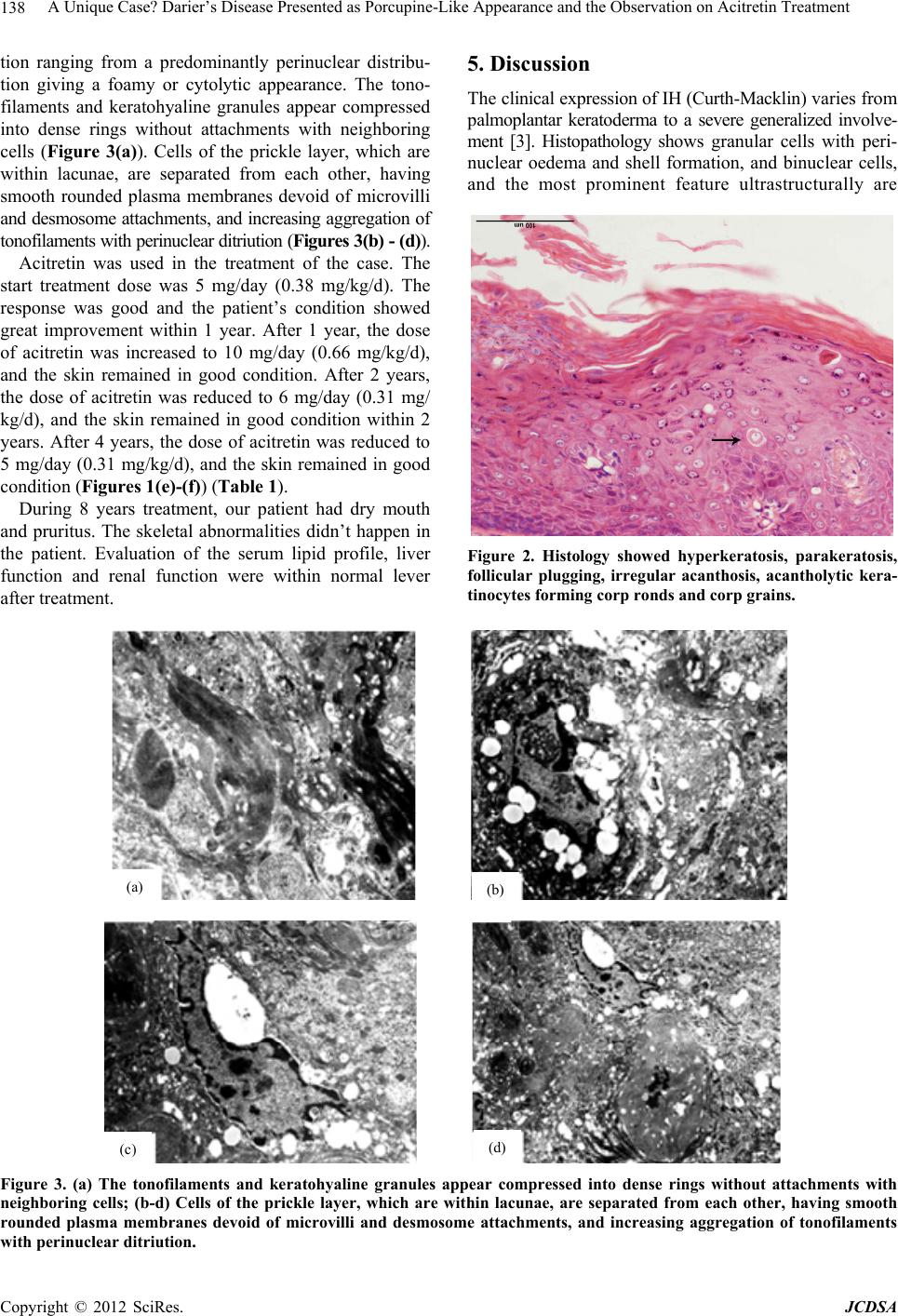
ten with formation of papillae. The ultrastructural studies
reveal breakdown of the desmosome-keratin filament
complexes between keratinocytes. The light microscopy
and electron microscopic features of our patient showed
that the typical features of DD. Our patient was diag-
nosed as DD.
Despite much progress in understanding of the under-
lying abnormality in DD, disappointingly little has changed
in our treatment armoury. Many patients with mild disease
require no treatment other than simple emollient-like soap
substitutes and moisturizers (in particular, those contain-
ing urea or lactic acid can reduce scaling and irritation)
[8], with advice about the effects of sunshine. For those
with more severe disease, oral retinoids (etretinate, aci-
tretin, isotretinoin) are the most effective prescription.
Most patients tolerate 0.6 mg/kg of acitrecin daily, but 10-
25 mg daily is a reasonable starting dose and the dose
can be increased gradually [8]. The clinical response is
good in 90% of patients: Hyperkeratosis is reduced and
papules are flattened, while malodour may also improve.
However, retinoids are teratogenic and pregnancy must
be avoided during and for a while after treatment. Reti-
noids treatment may cause skeletal abnormalities in chil-
dren including osteoporosis, periosteal plucking, slender
long bones and premature epiphyseal closure. A starting
dose of acitretin of 0.38 - 0.66 mg/kg/d was recom-
mended and good responses were seen within 1 - 3 years.
The maintenance dose was titrated down to the 0.31
mg/kg/d. During 8 years treatment, our patient had dry
mouth and pruritus. The skeletal abnormalities didn’t
happen in the patient. Evaluation of the serum lipid pro-
file, liver function and renal function were within normal
lever after treatment.
In conclusion, the present study has demonstrated that
porcupine-like appearance is a unique pattern of DD.
Acitretin may be a useful therapeutic agent in children
with DD and less likely to cause skeletal problems.
REFERENCES
[1] F. Loche, M. Carrière, H. P. Schwarze, B. Thédenat and J.
Copyright © 2012 SciRes. JCDSA