Surgical Science, 2012, 3, 460-462
http://dx.doi.org/10.4236/ss.2012.39091 Published Online September 2012 (http://www.SciRP.org/journal/ss)
A Calcified Artery of Drummond, Could It Be a Sentinel
Sign of Further Complications?
Shahe Boghossian, Arpan K. Banerjee
Heart of England NHS Trust, Birmingham, UK
Email: shaboghru@gmail.com
Received March 24, 2012; revised April 30, 2012; accepted May 18, 2012
ABSTRACT
Objective: To und erstand the role of the artery of Drummo nd in the elderly population. The artery plays a crucial role
in the anastomosis between the inferior mesenteric artery and sup erior mesenteric artery. Its maintenance is particularly
important for the survivability of the bowel in events of stenosis of either one of the native arteries; SMA or IMA.
Method: A 94 year old lady presents with post-prandial abdominal pain and significant emaciation. The patient under-
goes clinical and radiological investigations to find out the cause of her ailments. Results: Abdominal X-ray revealed a
serpentine structure that was later defined as the artery of Drummond, CT scan revealed a calcified and enlarged artery
of Drummond in addition to an occluded origin of SMA and celiac artery as well as a severe stenosis origin of IMA.
Conclusion: The artery of Drummond was immensely hypertrophied and was supplying the entire bowel through the
native IMA; subsequent occlusion of the IMA was the main cause that caused the demise of the patient.
Keywords: Artery of Drummond; Mesenteric Ischemia; Refeeding Syndrome
1. Case Report
A 94 year old lady was admitted to Accident and Emer-
gency complaining of six week history of abdominal pain,
nausea and significant emaciation. She was alert with a
GCS of 15. Examination of the abdomen revealed two
well healed midline incisions. Palpation of the abdomen
revealed fullness on the left side of her abdomen as well
as a hard palpable tube like structure that rolled under-
neath the examiner’s fingers. Auscultation of her abdo-
men showed faint yet audible bowel sounds. Rectal ex-
amination showed an empty rectum. Chest X-ray showed
bibasal collapse but no obstruction of the bronchi and no
signs of any pulmonary malignancy.
On admission, her initial blood test showed the fol-
lowing: Na: 132, K: 4.2, Creatin ine: 82 mmo l/lit, Alb: 40,
Bilirubin: 16, Phosphate: 1.02, Hemoglobin: 14.4, Plate-
lets: 252, White cell count: 11.32. Her observation chart
was normal however the patient looked dehydrated and
hence the patient was put on a slow IV drip. The patient
looked generally emaciated and was put on IV rehydra-
tion, oral rehydration, as well as fortified oral protein
sachets. The patient was not able to tolerate the oral feed
and hence a provisional diagnosis of Refeeding Syn-
drome was put forward. Three days later, a random arte-
rial blood gas showed an elevation of serum lactate to 6.5
mmol/lit with a base excess of –3.0 mmol/lit, pCO2: 4.58
kPa, pO2: 12.0 kPa, pH: 7.4 and a CRP of 161. Her white
cell count was elevated at 19.38/ml. Unfortunately, the
patient expired a week later.
2. Findings
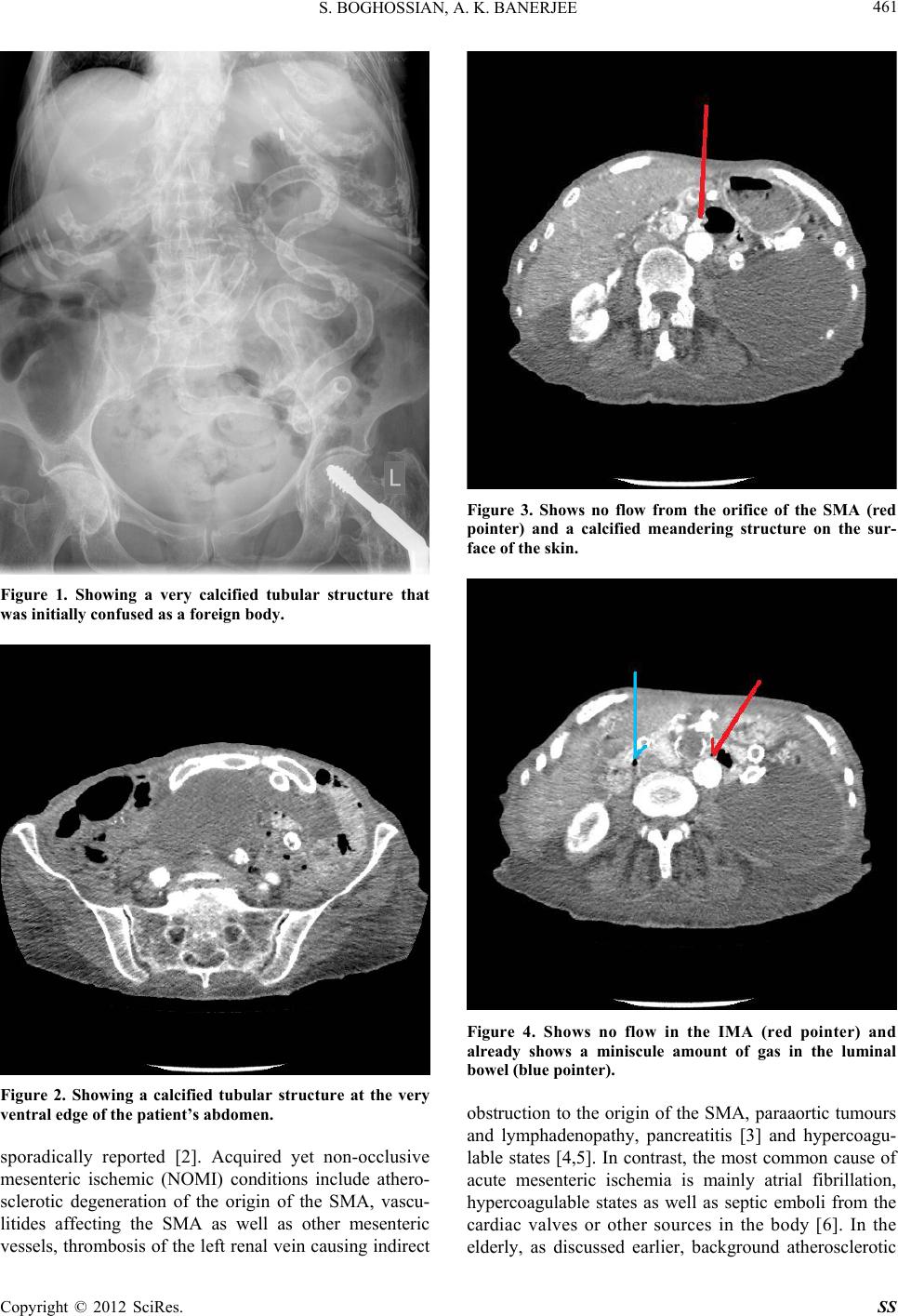
The abdominal and chest X-ray showed a calcified trans-
versely oriented tube like structure the crossed the full
spectrum of the abdomen (Figure 1). This was initially
thought to be a foreign body but later confirmed to be a
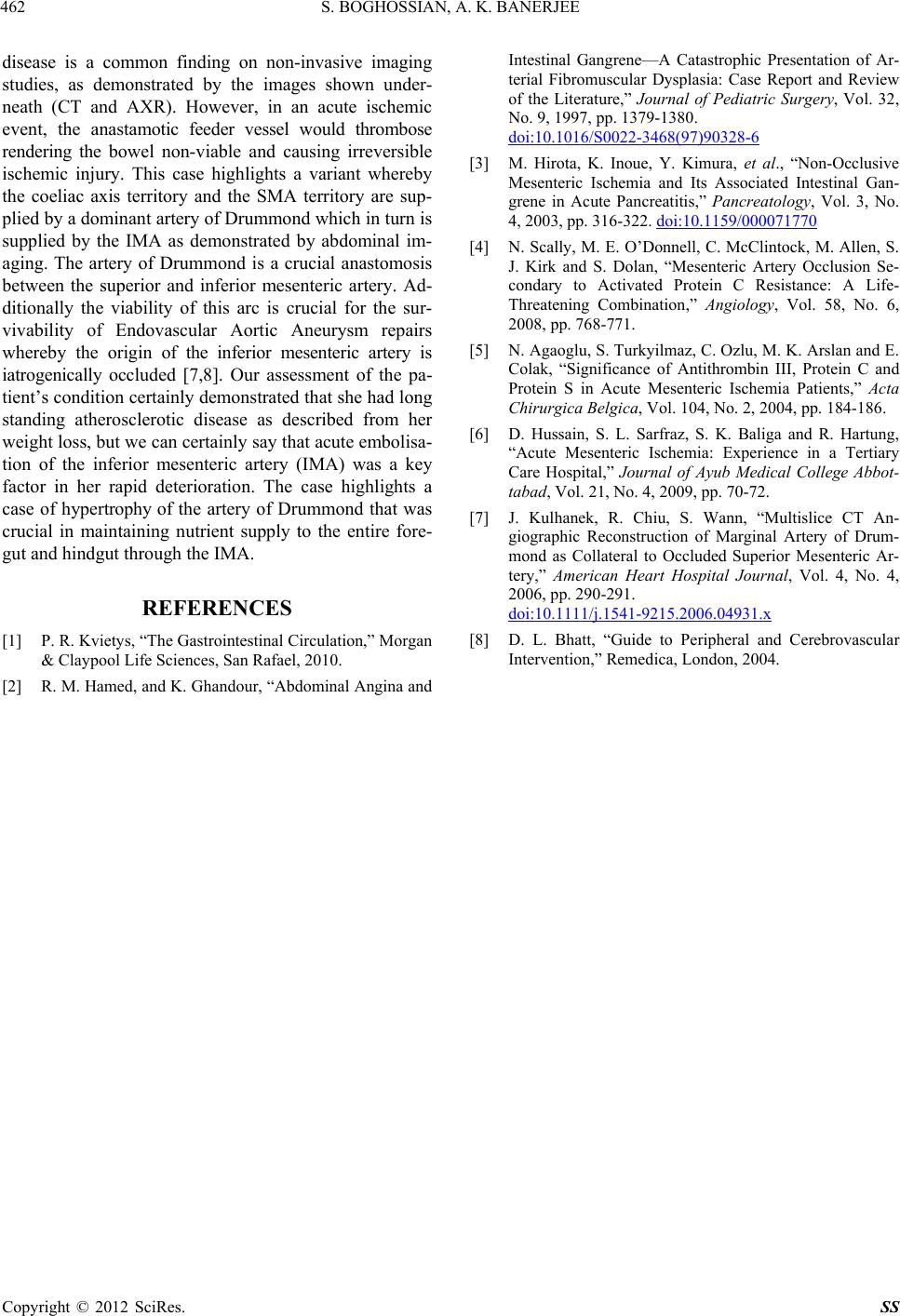
calcified vascular structure. Contrast enhanced Computer
Tomography confirmed the structure to be a calcified
artery of Drummond (Figure 2) with a stenosed origin of
the Celiac, Superior Mesenteric Artery (Figure 3) and
the Inferior Mesenteric Artery (Figure 4). The diagnosis
eventually confirmed mesenteric ischemia in the elderly.
3. Discussion
Chronic mesenteric ischemia is an indolent condition af-
fecting mainly the vascular supply to the small bowel. It
is mainly manifested by postprandial pain and subse-
quent weight loss. The most common artery involved is
the Superior Mesenter ic Artery (SMA) which supplies th e
duodenum, the jejunum, the ileum as well as the right
si de of the large bowel [1]. Occasionally, the coeliac art er y
may be involved as well, either as a solitary condition or
in association with widespread atherosclerosis of the A or ta .
Congenital conditions such as acute angulation of the S MA
with the Aorta or fibromuscular dysplasia have been
C
opyright © 2012 SciRes. SS