M. HANADA ET AL. 429
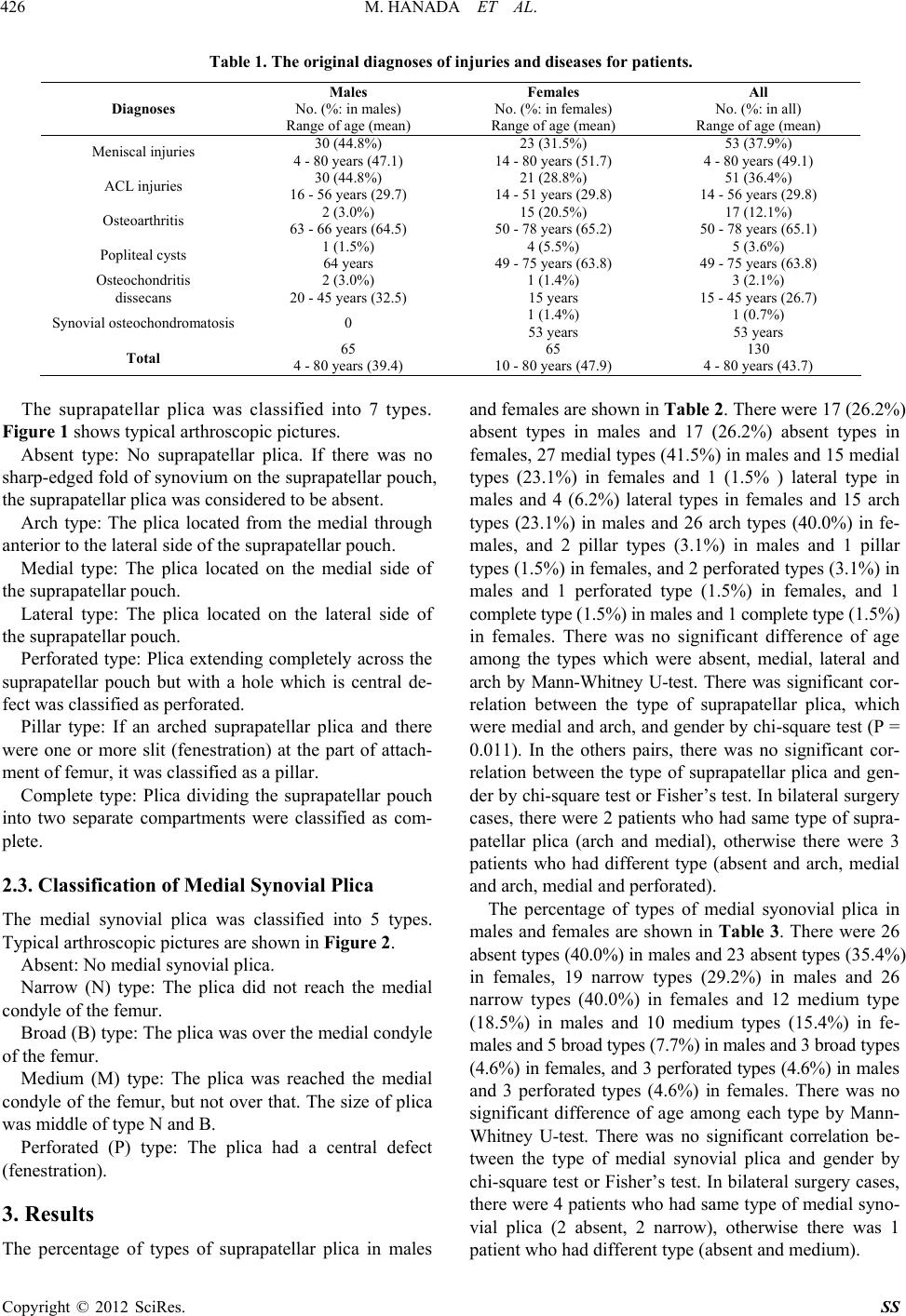
Table 6. The comparison of frequency of types of medial
synovial plica betwe en the study by Sakakibara’s classifica -
tion and ours.
Classification
(Sakakibara/Ours)
Sakakibara
(N = 100 knees)
Ours
(N = 130 knees)
Absent 55 (55.0%) 49 (37.7%)
A/narrow 4 (4.0%) 45 (34.6%)
B/medium 16 (16.0%) 22 (16.9%)
C/broad 23 (23.0%) 8 (6.2%)
D/perforated 2 (2.0%) 6 (4.6%)
5. Conclusion
We arthroscopically investigated and classified suprapa-
tellar plica and medial synovial plica in the Japanese
population. There was no relationship between suprapa-
tellar plica and medial synovial plica. We classified more
simply into 6 types of suprapatellar plica by only location
and shape of plica than Dandy’s classification. We clas-
sified simpler type of medial synovial plica by the size of
plica because Sakakibara’s Type A is a cord-like eleva-
tion in the synovial wall which is difficult to distinguish
with no existence of this plica.
REFERENCES
[1] D. Patel, “Arthroscopy of the Plicae-Synovial Folds and
Their Significance,” The American Journal of Sports
Medicine, Vol. 6, No. 5, 1978, pp. 217-225.
doi:10.1177/036354657800600502
[2] J. D. Dorchak, R. L. Barrack, J. S. Kneisl and A. H.
Alexander, “Arthroscopic Treatment of Symptomatic
Synovial Plica of the Knee. Long-Term Followup,” The
American Journal of Sports Medicine, Vol. 19, No. 5,
1991, pp. 503-507. doi:10.1177/036354659101900515
[3] A. E. Strover, E. Rouholamin, N. Guirguis and H. Behdad.
“An Arthroscopic Technique of Demonstrating the Patho-
mechanics of the Suprapatellar Plica,” Arthroscopy, Vol.
7, No. 3, 1991, pp. 308-310.
doi:10.1016/0749-8063(91)90133-I
[4] T. Zidorn, “Classification of the Suprapatellar Septum
Considering Ontogenetic Development,” Arthroscopy,
Vol. 8, No. 4, 1992, pp. 459-464.
doi:10.1016/0749-8063(92)90008-Y
[5] J. Y. Dupont, “Synovial Plicae of the Knee. Controversies
and Review,” Clinics in Sports Medicine, Vol. 16, No. 1,
1997, pp. 87-122. doi:10.1016/S0278-5919(05)70009-0
[6] S. J. Kim, S. J. Shin and T. Y. Koo, “Arch Type Patho-
logic Suprapatellar Plica,” Arthroscopy, Vol. 17, No. 5,
2001, pp. 536-538. doi:10.1053/jars.2001.21845
[7] M. Pekmezci, O. A. Atay, U. Kerimoğlu, U. Aydingöz, O.
Tetik and M. N. Doral, “A Complete Supra-Patellar Plica
with an Unusual Presentation,” Knee Surgery, Sports
Traumatology, Arthroscopy, Vol. 14, No. 9, 2006, pp.
872-874. doi:10.1007/s00167-006-0037-6
[8] J. W. Ewing, “Plica: Pathologic or Not?” Journal of the
American Academy of Orthopaedic Surgeons, Vol. 1, No.
2, 1993, pp. 117-121.
[9] J. Sakakibara, “Arthroscopic Study on Iino’s Band (Plica
Synovialis Mediopatellaris),” Japanese Orthopaedic As-
sociation, Vol. 50, 1976, pp. 513-522.
[10] D. J. Dandy, “Anatomy of the Medial Suprapatellar Plica
and Medial Synovial Shelf,” Arthroscopy, Vol. 6, No. 2,
1990, pp. 79-85. doi:10.1016/0749-8063(90)90002-U
[11] H. Gurbuz, O. U. Calpur, M. Ozcan, T. Kutoglu and R.
Mesut, “The Synovial Plicae in the Knee Joint,” Saudi
Medical Journal, Vol. 27, 2006, pp. 1839-1842.
Copyright © 2012 SciRes. SS