Smoking Cause Specific Lung Cancer—Evidence from Non-Smoking Lung Adenocarcinoma
440
smokers had higher response rates and lower rates of
progressive disease than former and current smokers [8].
As chemotherapy drugs work directly on the cancer cells,
different responses indicate different intracellular mecha-
nisms [20]. Previous study shows, compared with people
who never smoke, people with lung adenocarcinoma who
smoked or stopped smoking less than 25 years ago have
significant less EGFR mutations in exons 19 and 21 [21].
A study of comparing gene expression profiles in never
smokers and smokers with lung adenocarcinoma by
Powell et al. reported that there might be different path-
ways of cell transformation and tumor formation in two
groups, with many differences in gene expression. [22]
Those are strong evidences for the “different cancers”.
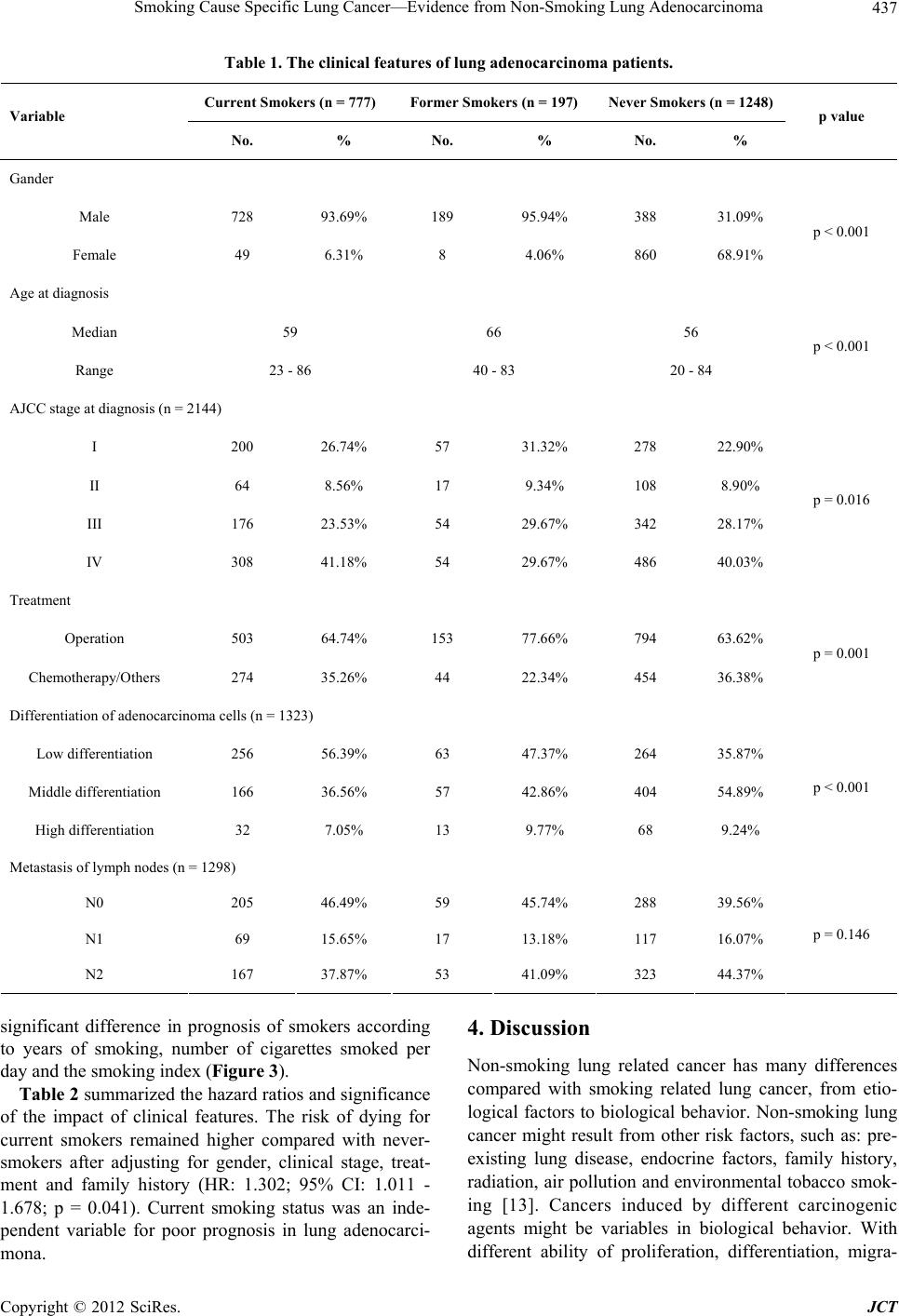
Surviving time of patients is considered as the most
important characteristics in cancer research. Different
subtypes of cancer usually have dissimilar prognosis,
such as: lung squamous cell cancer and adenocarcinoma;
gastric signet-ring cell carcinoma and adenocarcinoma;
hepatic cellular cancer and hepatobiliary cancer. Non-
smoking lung adenocarcinoma patients had a better prog-
nosis than current and former smokers. Interestingly,
former smoking patients had similar survival with non-
smoking patients and much better than current smoking
patients in the early stage, which is a good message for
patients who quit smoking. Study from Nordquist et al.
reported 5 years survival were 16% for current smokers
and 23% for never-smokers in 654 patients with lung
adenocarcinoma [23]. Similar results were reported by
Tammemagi et al., they studied 1155 lung cancer pa-
tients and found cigarette smoking was an important in-
dependent pred ictor of shor tened lung can cer surviv al [7].
Bryant et al. also found never smoker patients with early-
stage cancer have a significantly b etter survival rate than
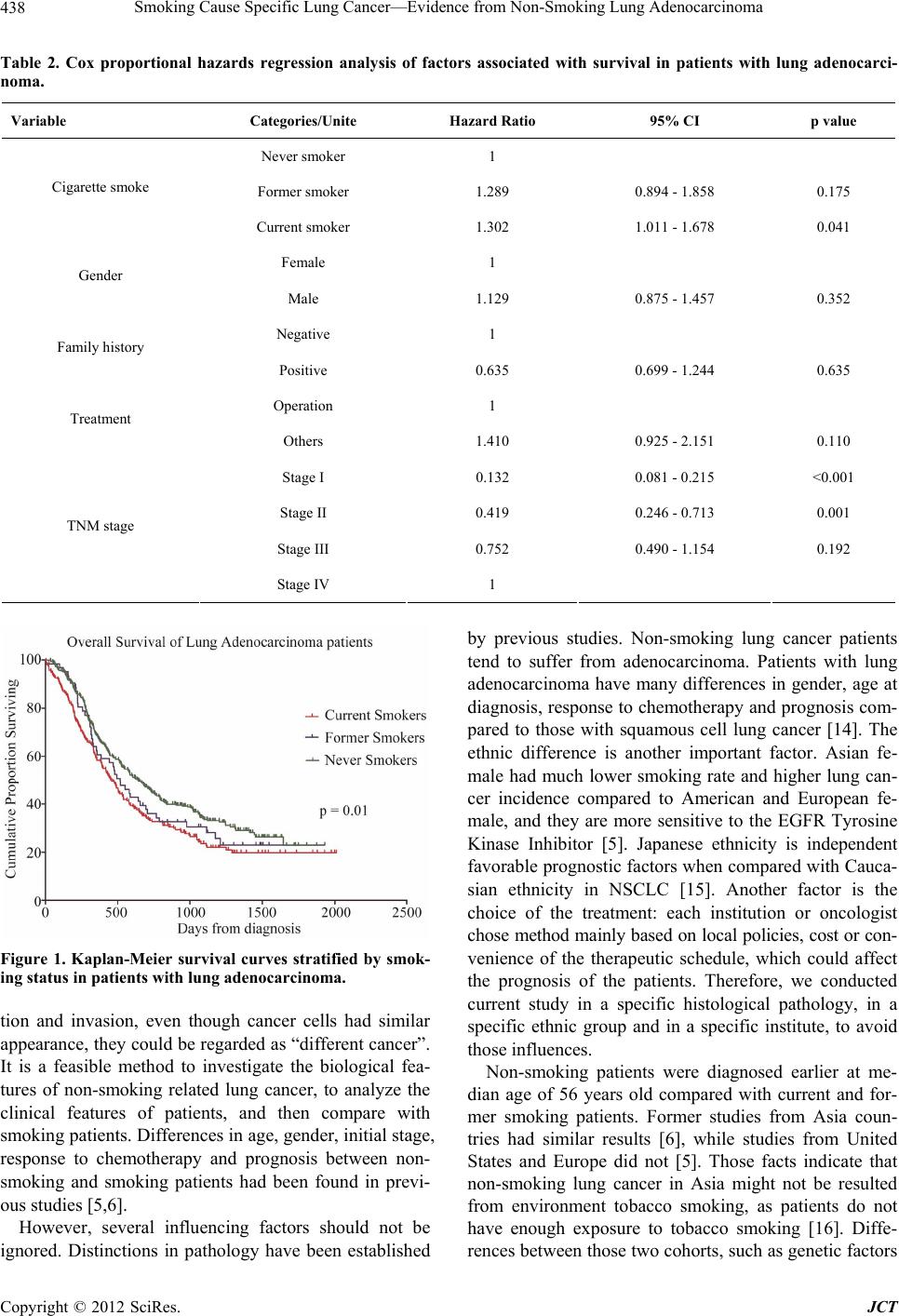
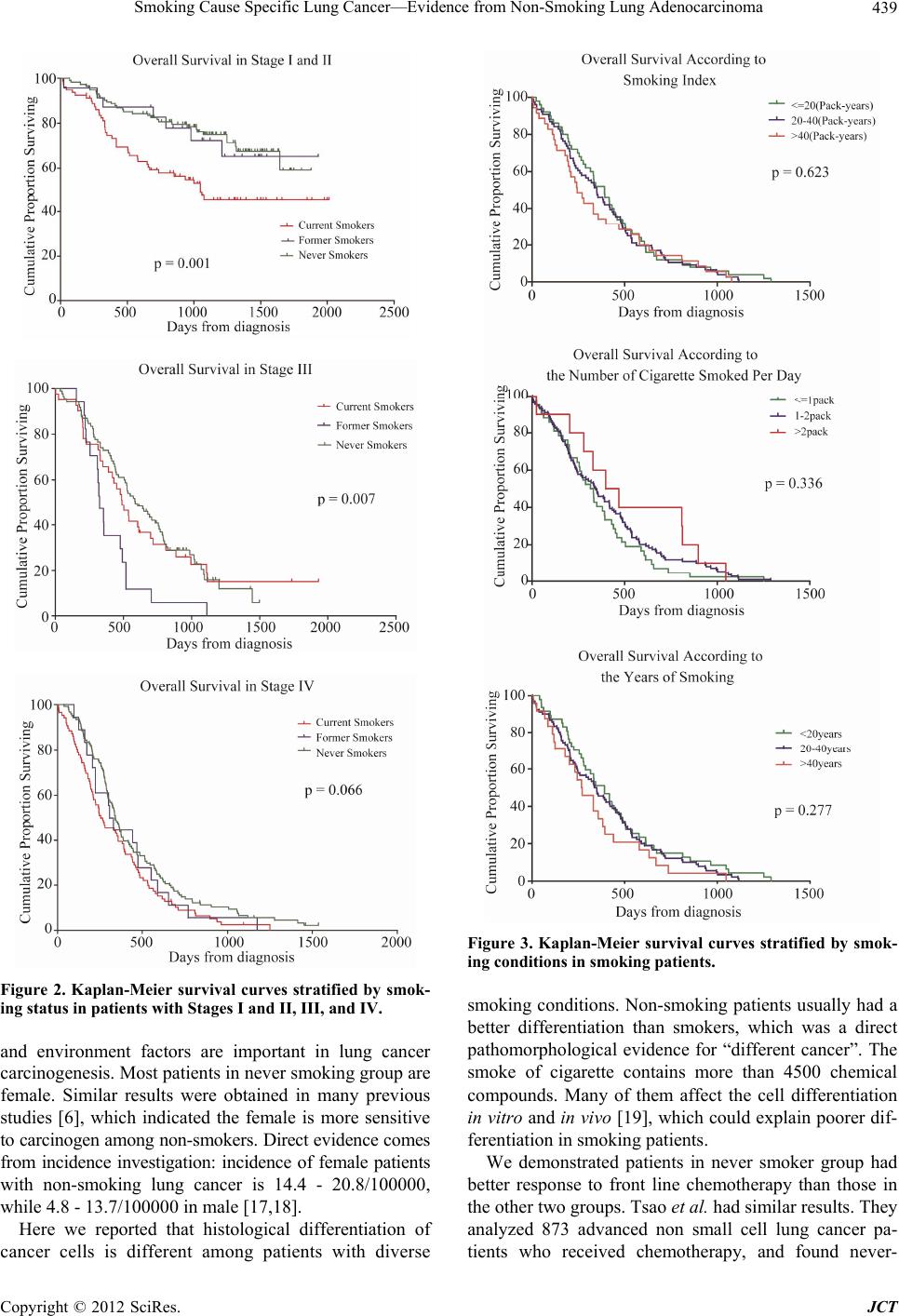
smokers [24]. As expected, in current study, we found
smoking conditions such as the number of cigarettes
smoked per day, years of smoking and the smoking index
do not affect the prognosis. The comorbidity of smoking
such as chronic obstructive pulmonary disease, hyperten-
sion, atherosclerosis and aortic aneurysm are more seri-
ous in heavy smoker; which may indicate that the diffe-
rence in prognosis was not because of the comorbidities
but the nature of cancer. We can infer that lung cancer
caused by smoking is the same type of cancer, which has
no correlation in prognosis with cigarette smoke burden.
With difference in prognosis, non-smoking lung adeno-
carcinoma could be considered as a different cancer.
In summary, we demonstrate significant differences
between non-smoking and smoking patients with lung
adenocarcinoma in age at diagnosis, gender, initial stage
at diagnosis, cell differentiation, response to chemothe-
rapy and prognosis. Furthermore, we suggest non-smok-
ing and smoking lung adenocarcinoma could be consi-
dered as different cancers with many distinctions in clin i-
cal features.
REFERENCES
[1] A. Jemal, T. Murray, E. Ward, et al., “Cancer Statistics,
2005,” CA—A Cancer Journal for Clinicians, Vol. 55,
No. 1, 2005, pp. 10-30. doi:10.3322/canjclin.55.1.10
[2] E. L. Wynder and E. A. Graham, “Landmark Article May
27, 1950: Tobacco Smoking as a Possible Etiologic Fac-
tor in Bronchiogenic Carcinoma. A Study of Six Hundred
and Eighty-Four Proved Cases,” JAMA, Vol. 253, No. 20,
1985, pp. 2986-2994.
doi:10.1001/jama.1985.03350440064033
[3] D. M. Parkin, F. Bray, J. Ferlay and P. Pisani, “Global
Cancer Statistics, 2002,” CA—A Cancer Journal for Cli-
nicians, Vol. 55, No. 2, 2005, pp. 74-108.
doi:10.3322/canjclin.55.2.74
[4] R. Gealy, L. Zhang, J. M. Siegfried, J. D. Luketich and P.
Keohavong, “Comparison of Mutations in the p53 and
K-Ras Genes in Lung Carcinomas from Smoking and
Nonsmoking Women,” Cancer Epidemiology, Biomar-
kers & Prevention, Vol. 8, No. 4, 1999, pp. 297-302.
[5] S. Sun, J. H. Schiller and A. F. Gazdar, “Lung Cancer in
Never Smokers—A Different Disease,” Nature Reviews
Cancer, Vol. 7, 2007, pp. 778-790. doi:10.1038/nrc2190
[6] C. K. Toh, F. Gao, W. T. Lim, et al., “Never-Smokers
with Lung Cancer: Epidemiologic Evidence of a Distinct
Disease Entity,” Journal of Clinical Oncology, Vol. 24,
No. 34, 2006, pp. 2245-2251.
doi:10.1200/JCO.2005.04.8033
[7] C. M. Tammemagi, C. Neslund-Dudas, M. Simoff and P.
Kvale, “Smoking and Lung Cancer Survival: The Role of
Comorbidity and Treatment,” Chest, Vol. 125, No. 1,
2004, pp. 27-37. doi:10.1378/chest.125.1.27
[8] A. S. Tsao, D. Liu, J. J. Lee, M. Spitz and W. K. Hong,
“Smoking Affects Treatment Outcome in Patients with
Advanced Nonsmall Cell Lung Cancer,” Cancer, Vol.
106, No. 11, 2006, pp. 2428-2436.
doi:10.1002/cncr.21884
[9] T. J. Lynch, D. W. Bell, R. Sordella, et al., “Activating
Mutations in the Epidermal Growth Factor Receptor Un-
derlying Responsiveness of Non-Small-Cell Lung Cancer
to Gefitinib,” New England Journal of Medicine, Vol.
350, No. 21, 2004, pp. 2129-2139.
doi:10.1056/NEJMoa040938
[10] S. W. Han, T. Y. Kim, P. G. Hwang, et al., “Predictive
and Prognostic Impact of Epidermal Growth Factor Re-
ceptor Mutation in Non-Small-Cell Lung Cancer Patients
Treated with Gefitinib,” Journal of Clinical Oncology,
Vol. 23, No. 16, 2005, pp. 2493-2501.
doi:10.1200/JCO.2005.01.388
[11] S. N. Rodin and A. S. Rodin, “On the Excess of G --> T
Transversions in the p53 Gene in Lung Cancer Cell Lines.
Reply to Pfeifer and Hainaut,” Mutation Research, Vol.
545, No. 1-2, 2004, pp. 141-147.
doi:10.1016/j.mrfmmm.2003.09.008
[12] C. K. Toh, E. H. Wong, W. T. Lim, et al., “The Impact of
Smoking Status on the Behavior and Survival Outcome of
Copyright © 2012 SciRes. JCT