 Vol.2, No.7, 652-660 (2010) doi:10.4236/health.2010.27099 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ Health PET in uterine malignancies Valeria Pirro1, Andrea Skanjeti1, Ettore Pelosi2* 1Nuclear Medicine Unit, San Giovanni Battista Hospital, University of Turin, Turin, Italy 2PET Centre, IRMET S.p.A., Turin, Italy; *Corresponding Author: e.pelosi@irmet.com Received 7 March 2010; revised 2 April 2010; accepted 5 May 2010. ABSTRACT Positron Emission Tomography (PET) or inte- grated PET/Computed Tomography (PET/CT) with 18F-Flu o ro-D eoxy-Glucos e (18F-FDG) is a fu- nctional imaging modality, useful in the char- acterization of undetermined morphological fin- dings, and in the staging/re-staging of a large number of malignancies. Although its use in uterine malignancies has been poorly investi- gated, in recent years the employment of this technique has constantly increased. In this re- view, we evaluate the role of PET (/CT) with 18F- FDG in uterine malignancies (cervical and en- dometrial cancers as well as uterine sarcomas), underlying its advantages and discussing its limitations. Metabolic and anatomic information given by PET/C T with 18F-FDG could be use ful in the evaluation of local and distant disease in- volvement at the staging, in the detection of disease recurrence, and in the evaluation of the response after chemotherapy and/or radio-the- rapy. Keywords: 18F-FDG PET/CT; Ute rine Maligna nci es; Cervical Cancer; Endometrial Cancer; Uterine Sarc omas 1. INTRODUCTION Positron Emission Tomography (PET) or integrated PET/Computed Tomography (PET/CT) with 18F-Fluoro- Deoxy-Glucose (18F-FDG) study is a functional, non invasive whole body examination, that allows to metab- olically characterize undetermined morphological find- ings, stage/re-stage disease, evaluate treatment response and monitor the therapy in a large number of malignan- cies (lymphomas, lung, breast, colon-rectal cancer, etc). In the genital tract of women the use of PET is contro- versial and it is limited by the urinary excretion of the 18F-FDG, that interfere with the evaluation of uterus and vagina, and by the numerous false positive findings re- lated to the presence of physiological tracer uptakes in the bowel, ovaries, and in the uterus itself. However, the clinical introduction of integrated PET/CT tomography, allowing the co-registration and the superimposition of anatomical and functional images and thus the exact localization of all the 18F-FDG uptakes, improved PET diagnostic accuracy [1]. The aim of the presen t review is to discuss the role of 18F-FDG-PET or PET/CT (PET/(CT)) exam in the uterine cervical cancer, in the endometrial adenocarcinoma and in the uterine sarcoma. 2. LITERATURE SEARCH For this review, in the matter of the role of 18F-FDG-PET (/CT) in the above mentioned gynaecological malignan- cies, a MEDLINE search has been performed in order to find relevant articles. For all the evaluated malignancies we included only primary studies and meta-analysis published in the English language in the last five years. We did not include case reports, and abstracts. For uter- ine cervical cancer we used as keywords: uterine cancer, cervical cancer, and uterine cervix carcinoma; while for endometrial cancer we used: uterine corpus carcinoma or neoplasm, and endometrial cancer. Finally, in the case of uterine sarcomas, we used as keywords uterine sarcoma, uterine carcinosarcoma, and uterine leyomiosarcoma. In all of the above mentioned cases, each keyword was always associated with Positron Emission Tomography, PET/CT, and 18F-FDG-PET/CT. Furthermore, to com- plete the search we look for in the bibliography of the founded studies and considered the most recent and in- teresting works. 3. CERVICAL CANCER Cervical cancer is the third most common neoplasm in women. Recent data report an incidence rate of about 42,000 new cases/year in the United States and in the European Union [2,3] and 150,000 deaths/year world-  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 653 653 wide [4]. In the last decades, the introduction of the Pa- panicolau screening test (Pap-test) has allowed an in- crease in the detection rate of pre-invasive lesions; in the same time the mortality due to the invasive cervical cancer has not substantially decreased [5,6]. To stage cervical cancer the International Federation of Gynaecologists and Obstetrics (FIGO) staging system is currently used [7,8]. In patients with small localized carcinomas (stage IA and IB1) radical hysterectomy or radiotherapy alone are equally recommended [9]. For large lesions and/or locally advanced cancers (stage IB2– IVA), chemo-radiotherapy is the treatment of choice [10,11]. Tumour size, parametrial tissue involvement, pelvic and/or para-aortic lymph node spread and deep invasion of nearby organs are the most important prog- nostic parameters at the diagnosis [12]. Patients with these unfavourable prognostic factors are at high risk of developing disease recurrence with an estimated recur- rence rate rangi ng bet ween 23% and 3 5% [1 3,14]. Even if the assessment of local and distant disease ex- tension is a crucial point both in the pre- and post-treat- ment phases, however a standardized protocol to stage/ re-stage these patients has not been established [15]. In particular, no imaging modalities are routinely used in this work up, which is based on physical examination, Pap-test, serum markers assay and surgical evaluation. Currently, the use of 18F-FDG-PET/CT in the manage- ment of patients with cervical cancer has been investi- gated in different settings. 3.1. Staging The assessment of the primary lesion is actually based on the clinical examination and on morphological imag- ing modalities, in particular MRI. One of the crucial data is the presence of uterine parametrial invasion. In this field, despite the presence of co-registered CT images, the diagnostic performance of 18F-FDG-PET/CT is worse than MRI, due to the lack of a good spatial reso lution. In the local staging of 32 primary tumour s, Park et al. high- lighted a higher number of false negative results at PET scan than at MRI (3 and 1 case, respectively) [9]. Proba- bly, in stage IA or IB the amount of disease is under or at the limit of the PET system resolution and its detection can be elusive. Moreover, the interference of urinary activity, that of physiological processes (such as hor- mone-dependent changes in the ovaries and endome- trium during the phases of menstrual cycle) and some benign pathologies (such as corpus luteum cysts, endo- metriosis, inflammations, menstruations, etc.) can inter- fere with the optimal evaluation of the primary lesion, leading to difficulties in exam interpretation [12,16]. Some of these PET limitations can be reduced with prac- tical expedients: for example, the urinary interference can be avoided by emptying the bladder just before the start of the exam, or by the hydration and administration of diuretics, or by the continuous bladder irrigation to dilute and remove the radioactive urine. On the basis of these limitations, it is clear that, despite the on-going technical improvements, PET is still unsatisfactory in the evaluation of the primary lesion and particularly in the identification of the deep uterine tissue involvement. On the other hand, an application of PET exam in these cases is actually under debate, i.e. the prognostic value of the primary lesion 18F-FDG uptake. The tumour 18F-FDG uptake, generally measured by the maximum Standardized Uptake Value (SUVmax), seems to be strictly related to the behaviour and to the aggressiveness of the tumour itself as in other malignancies (head and neck, lung and oesophageal cancers). In uterine cancer different authors reported an independent correlation between the cancer SUVmax and: the lymph node status, the disease response to chemo/radio therapy, the fre- quency of pelvic recurrence, the disease free and the overall survival [12,17-20]. In a study on 240 patients, Kidd et al. [21] confirmed the correlation between the SUVmax at the staging and the presence of lymph node metastases. Moreover, Lee and colleagues [22] observed a good correlation between SUVmax and DFS in early stages of cervical cancer. From these experiences, it seems that SUVmax could be a useful prognostic tool in this cancer too. In the pre-treatment disease staging, the identification of nodal (loco-regional and para-aortic) and distant me- tastasis are crucial points, which present prognostic and therapeutic significance. In fact, in locally advanced cervical cancer the 5 year survival rate is 57%, 34% or 12%, in node negative cases, pelvic nodes metastasis or para-aortic nodes metastasis, respectively [23]. In a re- cent meta-analysis, the most accurate method to study lymph node involvement resulted to be the sentinel node biopsy; however, this is a (minimal) invasive procedure, that often requires the administration of anaesthetic drugs, and that could lead to some complications. Among the imaging tests, the authors of this meta-analysis af- firm that PET/CT presents better accuracy than contrast enhancement (CE) CT and MRI and that it could be used to guide laparoscopic staging procedures [24]. In fact, the sensitivity of CECT and/or MRI in identifying nodal metastasis is very low. A Gynaecological Oncology Group (GOG) study reported a sensitivity of 34% in the detection of para-aortic lymph nodes by CECT [25]. Furthermore, in patients with gynaecological cancer and CECT negative for lymph node metastasis, PET/CT showed sensitivity and specificity of 50% and 83.3% respectively [25]. The good accuracy of PET and PET/CT scans in detecting lymph nodes has been established by 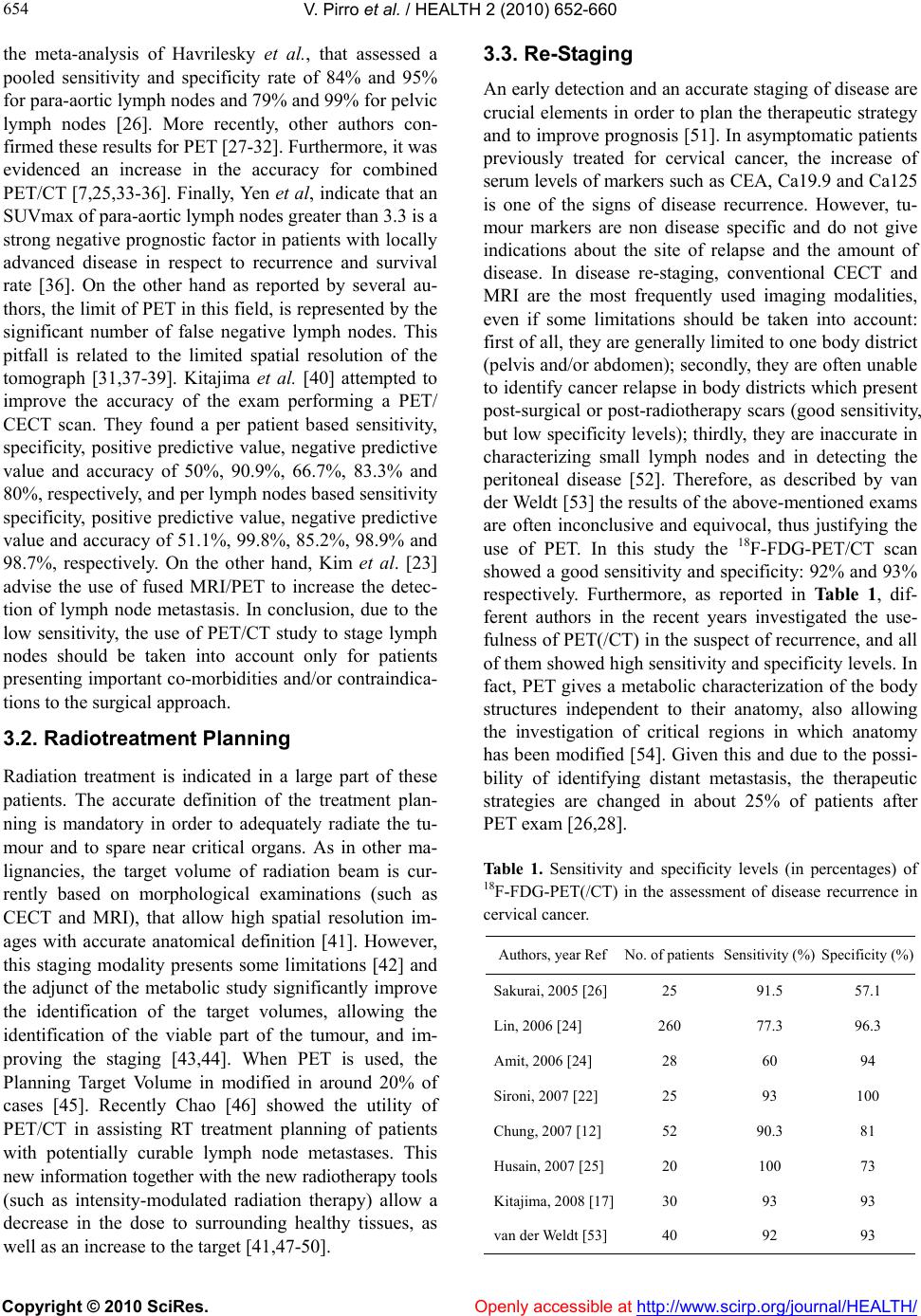 V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 654 the meta-analysis of Havrilesky et al., that assessed a pooled sensitivity and specificity rate of 84% and 95% for para-aortic lymph nodes and 79% and 99% for pelvic lymph nodes [26]. More recently, other authors con- firmed these results for PET [27-32]. Furthermore, it was evidenced an increase in the accuracy for combined PET/CT [7,25,33-36]. Finally, Yen et al, indicate that an SUVmax of para-aortic lymph nodes greater than 3.3 is a strong negative prognostic facto r in patients with locally advanced disease in respect to recurrence and survival rate [36]. On the other hand as reported by several au- thors, the limit of PET in this field, is represented by the significant number of false negative lymph nodes. This pitfall is related to the limited spatial resolution of the tomograph [31,37-39]. Kitajima et al. [40] attempted to improve the accuracy of the exam performing a PET/ CECT scan. They found a per patient based sensitivity, specificity, positive predictive value, negative predictive value and accuracy of 50%, 90.9%, 66.7%, 83.3% and 80%, respectively, and per lymph nodes based sensitiv ity specificity, positive predictive value, negative predictive value and accuracy of 51.1%, 99.8%, 85.2%, 98.9% and 98.7%, respectively. On the other hand, Kim et al. [23] advise the use of fused MRI/PET to increase the detec- tion of lymph node metastasis. In conclusion, due to the low sensitivity, the use of PET/CT study to stage lymph nodes should be taken into account only for patients presenting importan t co-morbidities and/or co ntraindica- tions to the surgical approach. 3.2. Radiotreatment Planning Radiation treatment is indicated in a large part of these patients. The accurate definition of the treatment plan- ning is mandatory in order to adequately radiate the tu- mour and to spare near critical organs. As in other ma- lignancies, the target volume of radiation beam is cur- rently based on morphological examinations (such as CECT and MRI), that allow high spatial resolution im- ages with accurate anatomical definition [41]. However, this staging modality presents some limitations [42] and the adjunct of the metabolic study significantly improve the identification of the target volumes, allowing the identification of the viable part of the tumour, and im- proving the staging [43,44]. When PET is used, the Planning Target Volume in modified in around 20% of cases [45]. Recently Chao [46] showed the utility of PET/CT in assisting RT treatment planning of patients with potentially curable lymph node metastases. This new information together with the new radiotherapy tools (such as intensity-modulated radiation therapy) allow a decrease in the dose to surrounding healthy tissues, as well as an increase to the target [41,47-50]. 3.3. Re-Staging An early detection and an accurate staging of disease are crucial elements in order to plan the therapeu tic strategy and to improve prognosis [51]. In asymptomatic patients previously treated for cervical cancer, the increase of serum levels of markers such as CEA, Ca19.9 and Ca125 is one of the signs of disease recurrence. However, tu- mour markers are non disease specific and do not give indications about the site of relapse and the amount of disease. In disease re-staging, conventional CECT and MRI are the most frequently used imaging modalities, even if some limitations should be taken into account: first of all, they are generally limited to o ne body district (pelvis and/or abdomen); secondly, they are often unable to identify cancer relapse in body districts which present post-surgical or post-radiotherapy scars (good sensitiv ity, but low specificity levels); thirdly, they are inaccurate in characterizing small lymph nodes and in detecting the peritoneal disease [52]. Therefore, as described by van der Weldt [53] the results of the above-mentioned exams are often inconclusive and equivocal, thus justifying the use of PET. In this study the 18F-FDG-PET/CT scan showed a good sensitiv ity and specificity: 92% and 93% respectively. Furthermore, as reported in Table 1, dif- ferent authors in the recent years investigated the use- fulness of PET(/CT) in the suspect of recurrence, and all of them showed high sensitiv ity and specificity levels. In fact, PET gives a metabolic characterization of the body structures independent to their anatomy, also allowing the investigation of critical regions in which anatomy has been modified [54]. Given this and due to the possi- bility of identifying distant metastasis, the therapeutic strategies are changed in about 25% of patients after PET exam [26,28]. Table 1. Sensitivity and specificity levels (in percentages) of 18F-FDG-PET(/CT) in the assessment of disease recurrence in cervical cancer. Authors, year RefNo. of patients Sensitivity (%) Specificity (%) Sakurai, 2005 [26]25 91.5 57.1 Lin, 2006 [24] 260 77.3 96.3 Amit, 2006 [24] 28 60 94 Sironi, 2007 [22] 25 93 100 Chung, 2007 [12] 52 90.3 81 Husain, 2007 [25] 20 100 73 Kitajima, 2008 [17]30 93 93 van der Weldt [53]40 92 93  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 655 655 As regards the follow-up, Brooks [4] demonstrated that PET/CT presents a good accuracy in detecting re- currences in both asymptomatic and symptomatic women. In his study, it was interestingly sh owed that the survival of women with asymptomatic recurrences was superior to the symptomatic subjects. As regards the prognosis, the modifications of the 18F-FDG-uptake during the course of the treatment re- presents an important predictor of tumour response and patient’s survival [55]. Nishiyama [19] evaluated the role of PET in monitoring the neo-adjuvant therapy in pa- tients with advanced stages of gynaecological cancers. In his study, PET showed an accuracy of 85% in predicting response to the treatment, when the SUVmax was de- creased more than 65%. However, larger studies are needed to better define the PET role in this context [56]. 4. ENDOMETRIAL CANCER Endometrial cancer is a common malignant disease, be- ing the fourth cancer in post-menopausal women. In Europe, about 1 out of 20 new cancers’ cases interests the endometrium and in the United States the incidence rate is about 40,000 new cases/year [57,58]. As in cervi- cal cancer, the surgical-pathological FIGO staging sys- tem is used to address patients to the more appropriate treatment. Patients with FIGO stage IA and IB (in- volvement of less than 50% of myometrium thickness) can be treated with a tumour resection, while patients with stage IC (involvement of more than 50% of myo- metrium thickness) the para-aortic lymphnode dissection and the use of adjuvant chemo-radiotherapy is one of the proposed therapeutic strategy, due to the fact that this stage has a greater inciden ce of nodal and distant metas- tasis, with a worse prognosis [59]. Generally, patients with the clinical suspect of deep myometrial invasion undergo further examinations (CT or MRI), in order to assess the extra uterine disease spread. The role of 18F-FDG-PET/CT in the management of this neoplasm is not well defined due to the lack of con- sistent data in the literature, and due to this reason uter- ine corpus cancer is not included among appropriate applications in oncology [4 5] . Few small studies assessed the validity of PET alone in the evaluation of primary endometrial cancer, show- ing good levels of sensitiv ity (rang e 83.3 -96.7 % [59-61]). Torizuka et al. affirmed the feasibility of PET study in the assessment of myometrial involvement, reporting a better diagnostic accuracy than MRI (86.4% versus 77.3% respectively) [59]. In fact, in this study the SUV of the tumour correlated significantly with the depth of the tumour invasion. Furthermore, the authors used SUV of the primary tumour, dichotomized to 12, in order to predict the depth of the tumour invasion. They showed that SUV < 12 correlated significantly with superficial invasion, while SUV > 12 correlated with profound in- vasion of the tumour. However, due to th e limited spatial resolution of the PET study, a limited size of invasion could be missed, leading to false negative PET results [62]. Recently, two randomized trials showed that in early stages of endometrial cancer the routine pelvic lymphadenectomy improves the staging, furthermore this surgical staging correlated with prognosis of the patients. However, the advantage gained was only fur- ther knowledge, since no survival benefits were ob- served in these patients. On the contrary, women that undergo surgical staging have increase the risks of com- plications. Therefore, the goal of the non-invasive stag- ing in these women would be to select those patients in whom the surgical staging could improve prognosis not only the staging [63-65]. In regard to PET/CT, Park et al. showed in a population of 53 patients weak levels of sensitivity and specificity in the staging of primary le- sions (89.4 and 50.5%, respectively) and in the staging of regional lymph nodes (69.2 and 90.3%, respectively). On the other hand, high accuracy levels were reported in the detection of distant metastasis. The authors con- cluded that there are two main advantages of 18F-FDG- PET/CT in the preoperative assessment of endometrial cancer: the good negative predictive value in predicting lymph node metastasis, that allows avoidance of surgical staging in poor candidates for such procedure; the high accuracy in detecting distant metastasis [66]. However, again it must be reminded that in the above mentioned study, the negative pr edictive value (NPV) was good but not excellent (98.9% in the pelv ic evaluation, decrease in 87.5% for the para-aortic nodes). Furthermore the NPV was further investigated by Signorelli [63]. It was indi- cated that in high risk early stages the high NPV could be useful to avoid systemic lymphaedenectomy. In such cases a de-bulking surgery of the involved nodes could be sufficient. With the decrease of lymph node dimen- sion, a progressive significant reduction of sensitivity has been observed by Kitajima et al.: 93.3% for lesions greater than 10 mm, 66.7% for lesions between 5 and 9 mm, and 16.7% for lesions smaller than 4 mm [67] Fur- thermore, Inubashiri [68] observed in recent work that 18F-FDG-PET/CT cannot change the medical manage- ment of the patients if a MRI is previously performed. As indicated by some authors, in endometrial cancer the major contribution of 18F-FDG-PET/CT could be in the early assessment of disease recurrence after therapy [60,69]. The go od performance of 18F-FDG-PET/ CT has been confirmed by Kitajima et al. in a recent paper in- cluding 30 patients, that sho wed an overall patient-b ased sensitivity, specificity and accuracy of 93% [70].  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 656 In conclusion, in endometrial cancer, the most rele- vant indications obtained by PET are: the possibility of detecting disease recurrence in asymptomatic patients presenting an increase of the Ca125 serum levels; the ability in distinguishing fibrotic tissue from viable le- sions after the treatment; the metabolic definition of the radiotherapy treatment planning. Encouraging results are also available in the assessment of lymph nodes and dis- tant metastasis during the disease staging. 5. UTERINE SARCOMAS Uterine sarcomas are rare neoplastic diseases which represent about a 2-4% of all uterine malignancies [71]. The histology is heterogeneous, but the more represented variety are the leiomyosarcoma, the carcinosarcoma and the endometrial sarcoma. These malignancies present an extremely poor prognosis and, despite their rarity, they are responsible for a large number of deaths every year, in women with uterine cancer. As with t he be ni g n u terine leiomyoma, clinical features are represented by vaginal bleeding and pain. Therefore, during the diagnostic process, the differential diagnosis is crucial. Unfortu- nately, in the maj ority of cases this is o btained only after surgery at the histopathological examination, because morphological imaging (US and MRI) is often in conclu- sive. Therapeutic options in these cancers actually include the surgery (hysterectomy) when the cancer is localized, and chemotherapy if the tumour is locally and/or dis- tantly extended. During the follow-up about one half of Stage I cases develop a recurrence [72]. In the manage- ment of sarcomas (soft tissues and bone sarcoma), the current literature evidences discordant data on the accu- racy and the usefulness of 18F-FDG-PET scan due to the small number and to the heterogeneity of the included cases; however, PET seems to be capable of differenti- ating between low and high grade sarcomas, and in the evaluation of residual disease after therapy [73]. In the case of uterine sarcomas, some authors suggest the use of PET study to distinguish between leiomyomas and leiomyosarcomas [74]. The identification of distant me- tastases could be another reason for the execution of a PET scan in the staging of these patients. However, a recent study presented that only 9% of patients per- formed an 18F-FDG-PET scan as part of perioperative imaging. [75]. Despite the spare chemotherapy response the preco- cious and accurate detection of disease recurrence is crucial. However, an effective diagnostic strategy for an early identification of relapse is missing, and specific serological tumour markers are not available. Even if, at this moment, there is not enough ev id ence to valid ate th e use of this exam in the follow up of asymptomatic pa- tients and in the evaluation of clinically suspected recur- rences, in this scenario 18F-FDG-PET/CT could be use- ful. In fact in a recent study Ho and colleagues [76] showed that PET scan could change the management in falsely inoperable patients or showing distant metastases. On the other hand Park et al. [77] showed that the PET scan has a good impact in the surveillance of patients with uterine sarcomas. In fact, in this study, PET scan, show a very good accur acy (94,4%) in women with sus- pected recurrence and a good sensitivity (87,5%) in as- ymptomatic women and contribute to change the treat- ment in 1/3 of the population. The results of the few small reports are encouraging in this way, but not com- pletely in agreement [72,76,77]. Further, clinical studies are needed to define the role of 18F-FDG-PET/CT in uterine sarcomas. 6. CONCLUSIONS In this review, we evaluated the role of 18F-FDG-PET/ CT in uterine malignancies. This safe, non invasive, im- aging modality gives useful metabolic and anatomic information, and, as in the other field of oncology, it is beginning to play an important role in the management of these patients. Despite the relatively low number of studies, its usefulness in the assessment of lymph-nodal involvement at the staging, in the detection and staging of disease recurrence, and in the evaluation of the re- sponse after chemo- and radio-therapy has been proved. In fact the use of PET/CT in uterine cancer seems to be controversial. Despite numerous and rigorous study demonstrated the utility, gynecologic oncologist are not very enthusiastic of this exam. In fact, such as Kizer et al. [78] demonstrated in a recent study, when 83% of them routinely order CT scan, only 28% of them rou- tinely order PET/CT scan. Some of them believe that PET/CT does not provide useful prognostic information whereas others causes could be the difficulty to obtain third party payment from the private paying clients. It seems that the better staging of metastatic lymph nodes or distant metastases, the very good negative predictive value in early stages, the correlation of before/after treatment PET result with the overall survival, data al- ready available, have little impact and do not convince the gynecologic oncologist. However, these data are good sources for the planning of other prospective stud- ies that could have a greater impact. REFERENCES [1] Tatsumi M, Cohade C, Bristow R.E. and Wahl R.L. (2009) Imaging uterine cervical cancer with FDG-PET/  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 657 657 CT: Direct comparison with PET. Molecular Imaging and Biology, 11(4), 229-235. [2] National Cancer Institute, Cervical Cancer, Bethesda (MD). www.cancer.gov/cancertopics/types /cervical [3] Arbyn, M., Raifu, A.O. and Ferlay, J. (2007) Burden of cervical cancer in Europe. Annals of Oncology, 18(10), 1708-1715. [4] Brooks, R.A, Rader, J.S., Dehdashti, F., Mutch, D.G., Powell, M.A., Thaker, P.H., Siegel, B.A. and Grigsby, P.W. (2009) Surveillance FDG-PET detection of asymp- tomatic recurrences in patients with cervical cancer. Gy- necologic Oncolology, 112(1), 104-109. [5] Jemal, A., Siegel, R., Ward, E., Hao, Y., Xu, J. and Thun, M.J. (2009) Cancer statistics. CA: A Cancer Journal for Clinicians, 59(4), 225-249. [6] Jemal, A., Siegel, R., Ward, E., Hao, Y., Xu, J., Murray, T. and Thun, M.J. (2008) Cancer statistics, 2008. CA: A Cancer Journal for Clinicians, 58(2), 71-96. [7] Loft, A., Berthelsen, A.K., Roed, H., Ottosen, C., Lund- wall, L., Knudsen, J., Nedergaard, L., Højgaard, L. and Engelholm, S.A. (2007) The diagnostic value of PET/CT scanning in patients with cervical cancer: A prospective study. Gynecologic Oncolology, 106(1), 29-34. [8] Pecorelli, S., Benedet, J.L., Creasman, W.T. and Shep- herd J.H. (1999) FIGO staging of gynecologic cancer. 1994-1997 FIGO committee on gynecologic oncology. international federation of gynecology and obstetrics. In- ternational Journal of Gynaecology and Obstetrics, 65(3), 243-269. [9] Park, W., Park, Y.J. , Huh. S.J., Kim, B.G., Bae, D.S., Lee J., Kim, B.H., Choi, J.Y., Ahn, Y.C. and Lim, D.H. (2005) The usefulness of MRI and PET imaging for the detec- tion of parametrial involvement and lymph node metas- tasis in patients with cervical cancer. Japanese Journal of Clinical Oncology, 35(5), 260-264. [10] Grigsby, P.W. and Herzog, T.J. (2001) Current manage- ment of patients with invasive cervical carcinoma. Clinical Obstetrics and Gynecology, 44(3), 531-537. [11] Nicolet, V., Carignan, L., Bourdon, F. and Prosmanne, O. (2000) MR imaging of cervical carcinoma: A practical staging approach. Radiographics, 20(6), 1539-1549. [12] Kumar, R. and Dadparvar, S. (2007) 18F-Fluoro-2-de- oxy-D-glucose-Positron Emission Tomography (PET)/ PET-Computed Tomography in carcinoma of the cervix. Cancer, 110(8), 1650-1653. [13] Chung, H.H., Kim, S.K., Kim, T.H., Lee, S., Kang, K.W., Kim, J.Y. and Park, S.Y. (2006) Clinical impact of 18F-FDG-PET imaging in post-therapy surveillance of uterine cervical cancer: From diagnosis to prognosis. Gynecologic Oncolology, 103(1), 165-170. [14] Ryu, S.Y., Kim, M.H., Choi, S.C., Choi, C.W. and Lee, K.H. (2003) Detection of early recurrence with 18F-18F- FDG PET in patients with cervical cancer. Journal of Nuclear Medicine, 44(3), 347-352. [15] Harry, V.N. (2010) Novel imaging techniques as response biomarkers in cervical cancer. Gynecologic Oncolology, 116(2), 253-261. [16] Lerman, H., Metser, U., Grisaru, D., Fishman, A., Lievshitz, G. and Even-Sapir, E. (2004) Normal and ab- normal 18F-18F-FDG endometrial and ovarian uptake in pre- and post- menopausal patients: Assessment by PET/ CT. Journal of Nuclear Medicine, 45(2), 266-271. [17] Kidd, E.A., Siegel, B.A., Dejdashti, F. and Grigsby, P.W. (2007) The standardized uptake value for F18-Fluorodeoxy- glucose is a sensitive predictive biomarker for cervical cancer treatment response and survival. Cancer, 110(8), 1738-1744. [18] Xue, F., Lin, L.L., Dehdashti, F., Miller, T.R., Siegel, B.A. and Grigsby, P.W. (2006) F18 fluorodeoxyglucose uptake in primary cervical cancer as an indicator of prognosis after radiation therapy. Gynecologic Oncolology, 101(1), 146-151. [19] Nishiyama, Y., Yamamoto, Y., Kanenishi, K., Ohno, M., Hata, T., Kushida, Y., Haba, R. and Ohkawa, M. (2008) Monitoring the neoadjuvant therapy response in gyneco- logical cancer patients using FDG PET. European Jour- nal of Nuclear Medicine and Molecular Imaging, 35(2), 287-295. [20] Yoshida, Y., Kurokawa, T., Kawahara, K., Yagihara, A., Tsuchida, T., Okazawa, H., Fujibayashi, Y., Yonekura, Y. and Kotsuji, F. (2004) Metabolic monitoring of advanced uterine cervical cancer neoadjuvant chemotherapy by using [F-18]-Fluorodeoxyglucose positron emission to- mography: Preliminary results in three patients. Gyneco- logic Oncolology, 95(3), 597-602. [21] Kidd, E.A., Spencer, C.R., Huettner, P.C., Siegel, B.A., Dehdashti, F., Rader, J.S. and Grigsby, P.W. (2009) Cer- vical cancer histology and tumor differentiation affect 18F-fluorodeoxyglucose uptake. Cancer, 115(15), 3548- 3554. [22] Lee, Y.Y., Choi, C.H., Kim, C.J., Kang, H., Kim, T.J., Lee, J.W., Lee, J.H. , Bae, D.S. a nd Kim, B.G. (2009) The prognostic significance of the SUVmax (maximum stan- dardized uptake value for F-18 fluorodeoxyglucose) of the cervical tumor in PET imaging for early cervical cancer: Preliminary results. Gynecologic Oncolology, 115(1), 65-68. [23] Kim, S.K., Choi, H.J., Park, S.Y., Lee, H.Y., Seo, S.S., Yoo, C.W., Jung, D.C., Kang, S. and Cho, K.S. (2009) Additional value of MR/PET fusion compared with PET/CT in the detection of lymph node metastases in cervical cancer patients. European Journal of Cancer, 45(12), 2103-2109. [24] Selman, T.J., Mann, C., Zamora, J., Appleyard, T.L. and Khan, K. (2008) Diagnostic accuracy of tests for lymph node status in primary cervical cancer: A systematic re- view and a metanalysis. Canadian Medical Association Journal, 178(7), 855-862. [25] Yildirim, Y., Sehirali, S., Avci, M.E., Yilmaz, C., Ertopcu K., Tinar, S., Duman, Y. and Sayhan, S. (2008) Integrated PET/CT for the evaluation of paraaortic nodal metastasis in locally advanced cervical cancer patients with negative conventional CT findings. Gynecologic Oncolology, 108(1), 154-159. [26] Havrilesky, L.J., Kulasingam, S.L., Matchar, D.B. and Myers, E.R. (2005) 18F-FDG-PET for management of cervical and ovarian cancer. Gynecologic Oncolology, 97(1), 183-191. [27] Husain, A., Akhurst, T., Larson, S., Alektiar, K., Barakat, R.R. and Chi, D.S. (2007) A prospective study of the ac- curacy of 18Fluorodeoxyglucose positron emission to- mography (18F-FDG PET) in identifying sites of metas- tasis prior to pelvic exenteration. Gynecologic Oncolol- ogy, 106(1), 177-180.  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 658 [28] Nakamoto, Y., Saga, T. and Fujii, S. (2005) Positron emission tomography application for gynecologic tumors. International Journal of Gynecological Cancer, 15(5), 701-709. [29] Roh, J.W., Seo, S.S., Lee, S., Kang, K.W., Kim, S.K., Sim, J.S., Kim, J.Y., Hong, E.K., Cho, D.S., Lee, J.S. and Park, S.Y. (2005) Role of positron emission tomography in pretreatment lymph node staging of uterine cervical cancer: A prospective surgicopathologic correlation study. European Journal of Cancer, 41(14), 2086-2092. [30] Unger, J.B., Lilien, D.L., Caldito, G., Ivy, J.J., Charrier, A. and Bellaire, B. (2007) The prognostic value of pretreat- ment 2-[18F]-fluoro-2-deoxy-D-glucose positron emis- sion tomography scan in women with cervical cancer. International Journal of Gynecological Cancer, 17(5), 1062-1067. [31] Wright, J.D., Dehdashti, F., Herzog, T.J., Mutch, D.G., Huettner, P.C., Rader, J.S., Gibb, R.K., Powell, M.A., Gao, F., Siegel, B.A. and Grigsby, P.W. (2005) Preopera- tive lymph node staging of early-stage cervical carci- noma by [18F]-fluoro-2-deoxy-D-glucose-positron emis- sion tomography. Cancer, 104(11), 2484-2491. [32] Rezvani, M. and Shaaban, A. (2009) Imaging of cervical pathology. Clinical Obstetrics and Gynecology, 52(1), 94-111. [33] Sironi, S., Buda, A., Picchio, M., Perego, P., Moreni, R., Pellegrino, A., Colombo, M., Mangioni, C., Messa, C. and Fazio, F. (2006) Lymph node metastasis in patients with clinical early-stage cervical cancer: Detection with integrated 18F-FDG PET/CT. Radiology, 238(1), 272- 279. [34] Choi, H.J., Roh, J.W., Seo, S.S., Lee, S., Kim, J.Y., Kim, S.K., Kang, K.W., Lee, J.S., Jeong, J.Y and Park, S.Y. (2006) Comparison of the accuracy of magnetic reso- nance imaging and positron emission tomography/com- puted tomography in the presurgical detection of lymph node metastases in patients with uterine cervical carci- noma: A prospective study. Cancer, 106(4), 914-922. [35] Chao, A., Ho, K.C., Wang, C.C., Cheng, H.H., Lin, G., Yen, T.C. and Lai, C.H. (2008) Positron emission tomo- graphy in evaluating the feasibility of curative intent in cervical cancer patients with limited distant lymph node metastasis. Gynecologic Oncology, 110(2), 172-178. [36] Yen, T.C., See, L.C., Lai, C.H., Tsai, C.S, Chao, A., Hsueh, S., Hong, J.H., Chang, T.C. and Ng, K.K. (2008) Standardized up-take value in paraaortic lymph nodes is a significant prognostic factor in patients with primary advanced squamous cervical cancer. European Journal of Nuclear Medicine and Molecular Imaging, 35(3), 493- 501. [37] Amit, A., Beck, D., Lowenstein, L., Lavie, O., Bar sha- lom, R., Kedar, Z. and Israel, O. (2006) The role of hy- brid PET/CT in the evaluation of patients with cervical cancer. Gynecologic Oncology, 100(1), 65-69. [38] Chou, H.H., Chang, T.C., Yen, T.C., Ng, K.K., Hsueh, S., Ya Ma, S., Chang, C.J., Huang, H.J., Chao, A., Wu, T.I., Jung, S.M., Lin, C.T., Huang, K.G. and Lai, C.H. (2006) Low value of [18F]-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography in primary staging of early stage cervical cancer before radical hysterectomy. Journal of Clinical Oncology, 24(1), 123-128. [39] Boughanim, M., Leboulleux, S., Rey, A., Pham, C.T., Zafrani, Y., Duvillard, P,, Lumbroso, J., Haie-Meder, C., Schlumberger, M. and Morice, P. (2008) Histologic re- sults of paraaortic lymphadenectomy in patients treated for stage IB2/II cervical cancer with negative [18F] Fluorodeoxy-glucose positron emission tomography scans in the paraaortic area. Journal of Clinical Oncology, 26(15), 2558- 2561. [40] Kitajima, K., Murakami, K., Yamasaki, E., Kaji, Y. and Sugimura, K. (2009) Accuracy of integrated FDG-PET/ contrast-enhanced CT in detecting pelvic and paraaortic lymph node metastasis in patients with uterine cancer. European Radiology, 19(6), 1529-1536. [41] Grosu, A.L., Piert , M., Weber, W., Jeremic, B., Pic cio, M., Schratzenstaller, U., Zimmermann, F.B., Schwaiger, M. and Molls, M. (2005) Positron Emission Tomography for radiation treatment planning. Strahlentherapie und Onko- logie, 181(8), 483-499. [42] Gold, M.A., Tian, C., Whitney, C.W., Rose, P.G. and Lanciano, R. (2008) Surgical versus radiographic deter- mination of paraaortic lymph node metastases before chemoradiation for locally advanced cervical carcinoma: A Gynecologic Oncology Group Study. Cancer, 112(9), 1954-1963. [43] Dolezelova, H., Slampa, P., Ondrova, B., Gombosova, J., Sovadinova, S., Novotny, T., Bolcak, K., Ruzickova, J., Hynkova, L. and Forbelska, M. (2008) The impact of PET with 18FDG in radiotherapy treatment planning and in the prediction in patients with cervix carcinoma: Re- sults of pilot study. Neoplasma, 55(5), 437-441. [44] Boughanim, M., Leboulleux, S., Rey, A., Pham, C.T., Zafrani, Y., Duvillard, P., Lumbroso, J., Haie-Meder, C., Schlumberger, M. and Morice, P. (2008) Histologic re- sults of paraaortic lymphadenectomy in patients treated for stage IB2/II cervical cancer with negative [18F] fluorodeoxyglucose positron emission tomography scans in the paraaortic area. Journal of Clinical Oncology, 26(15), 2558-2561. [45] Regione Emilia Romagna. 18F-FDG-PET in oncologia. Criteri per un uso appropriato, 2006. [46] Chao, A., Ho, K.C., Wang, C.C., Cheng, H.H., Lin, G., Yen, T.C. and Lai, C.H. (2008) Positron emission tomo- graphy in evaluating the feasibility of curative intent in cervical cancer patients with limited distant lymph node metastases. Gynecologic Oncology, 110(2), 172-178. [47] Lin, C.T., Yen, T.C., Chang, T.C., Ng, K.K., Tsai, C.S., Ho, K.C. and Lai, C.H. (2006) Role of [18F] fluoro-2- deoxy-D-glucose positron emission tomography in re-recurrent cervical cancer. International Journal of Gynecological Cancer, 16(6), 1994-2003. [48] Esthappan, J., Mutic, S., Malyapa, R.S., Grigsby, P.W., Zoberi, I., Dehdashti, F., Miller, T.R., Bosch, W.R. and Low, D.A. (2004) Treatment planning guidelines regard- ing the use of CT/PET-guided IMRT for cervical carci- noma with positive paraaortic lymph nodes. International Journal of Radiation Oncology, Biology, Physics, 58(4), 1289-1297. [49] Esthappan, J., Chaudhari, S., Santanam, L., Mutic, S., Olsen, J., MacDonald, D.M., Low, D.A., Singh, A.K. and Grigsby, P.W. (2008) Prospective clinical trial of Positron Emission Tomography/Computed Tomography image- guided intensity-modulated radiation therapy for cervical carcinoma with positive paraaortic lymph nodes. Inter-  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 659 659 national Journal of Radiation Oncology, Biology, Phys- ics, 72(4), 1134-1139 [50] Lin, L.L., Mutic, S., low, D., LaForest, R., Vicic, M., Zoberi, I., Miller, T.R. and Grigsby, P.W. (2007) Adaptive brachytherapy treatment planning for cervical cancer us- ing 18F-FDG-PET. Journal of Radiation Oncology, Bi- ology, Physics, 67(1), 91-96. [51] Kitajima, K., Murakami, K., Yamasaki, E., Hagiwara, S., Fukasawa, I., Inaba, N., Kaji, Y. and Sugimura, K. (2008) Performance of 18F-FDG-PET/CT in the diagnosis of re- current endometrial cancer. Annals of Nuclear Medicine, 22(2), 103-109. [52] Grisaru, D., Almog, B., Levine, C., Metser, U., Fishman A., Lerman, H., Lessing, J.B. and Even-Sapir, E. (2004) The diagnostic accuracy of 18F-fluorodeoxyglucose PET/ CT in patients with gynecological malignancies. Gyne- cologic Oncoloy, 94(3), 680-684. [53] van der Veldt, A.A., Buist, M.R., van Baal, M.W., Co- mans, E.F., Hoekstra, O.S. and Molthoff, C.F. (2008) Clarifying the diagnosis of clinically suspected recur- rence of cervical cancer: Impact of 18F-FDG PET. Jour- nal of Nuclear Medicine, 49(12), 1936-1943. [54] Bjurberg, M., Kjellen, E., Ohlsson, T., Ridderheim, M. and Brun, E. (2007) 18F-FDG-PET in cervical cancer: staging, re-stagting and follow up. Acta Obstetricia et Gynecologica, 86(11 ), 1385-1391. [55] Schwarz, J.K., Siegel, B.A., Dehdashti, F. and Grigsby, P.W. (2007) Association of posttherapy positron emission tomogramphy with tumor response and survival in cer- vical carcinoma. Journal of the American Medical Asso- ciation, 289(19), 2289-2295. [56] Schwarz, J.K., Grigsby, P.W., Dehdashti, F. and Delbeke, D. (2009) The role of 18F-FDG PET in assessing therapy response in cancer of the cervix and ovaries. Journal of Nuclear Medicine, 50 (Suppl 1), 64S-73S. [57] Bray, F., Dos, S.S.I., Moller, H. and Weiderpass, E. (2005) Endometrial cancer incidence trends in Europe: Under- lying determinants and prospects for prevention. Cancer Epidemiology, Biomarkers & Prevention, 14(5), 1132- 1142. [58] Jemal, A., Tiwari, R.C., Murray, T., Ghafoor, A., Samuel, A., Ward, E., Feuer, E.J. and Thun, M.J. (2004) American Cancer Society. Cancer Statistics, 2004. CA: A Cancer Journal for Clinicians, 54(1), 8-29. [59] Torizuka, T., Nakamura, F., Takekuma, M., Toshihiko, K., Ogusu, T., Yoshikawa, E., Okada, H., Maeda, M. and Ouchi, Y. (2006) 18F-FDG PET for the assessment of myometrial infiltration in clinical stage I uterine corpus cancer. Nuclear Medicine Communications, 27(6), 481- 487. [60] Chao, A., Chang, T. C., Ng, K.K., Hsueh, S., Huang, H.J., Chou, H.H., Tsai, C.S., Yen, T.C., Wu, T.I. and Lai, C.H. (2006) 18F-FDG PET in the management of endometrial cancer. European Journal of Nuclear Medicine and Mo- lecular Imaging, 33(1), 36-44. [61] Suzuki, R., Miyagi, E., Takahashi, N., Sukegawa, A., Suzuki, A., Koike, I., Sugiura, K., Okamoto, N., Inoue, T. and Hirahara, F. (2007) Validity of positron emission to- mography using fluoro-2-deoxyglucose for the preopera- tive evaluation of endometrial cancer. International Journal of Gynecological Cancer, 17(1), 890-896. [62] Horowitz, N.S., Dehdashti, F., Herzog, T.J., Rader, J.S., Powell, M.A., Gibb, R.K., Grigsby, P.W., Siegel, B.A, Mutch, D.G. (2004) Prospective evaluation of 18F-FDG- PET for detecting pelvic and para-aortic lymphnode me- tastasis in uterine corpus cancer. Gynecologic Oncology, 95(3), 546-551. [63] Signorelli, M., Guerra, L., Buda, A., Picchio, M., Mangili G., Dell’Anna, T., Sironi, S. and Messa, C. (2009) Role of the integrated FDG PET/CT in the surgical manage- ment of patients with high risk clinical early stage endo- metrial cancer: Detection of pelvic nodal metastases. Gynecologic Oncology, 115(2), 231-235. [64] ASTEC study group, Kitchener, H., Swart, A.M., Qian, Q., Amos, C. and Parmar, M.K. (2009) Efficacy of sys- tematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): A randomised study. Lancet, 373(9658), 125-136. [65] Benedetti, P. P., Basile, S., Maneschi, F., Alberto, L. A., Signorelli, M., Scambia, G., Angi oli, R., Tateo, S., Man g i l i , G., Katsaros, D., Garozzo, G., Campagnutta, E., Don a de ll o , N., Greggi, S., Melpignano, M., Ra spagl ies i, F., Ragni, N., Cormio, G., Grassi, R., Franchi, M., Giannarelli, D., Fossati, R., Torri, V., Amoroso, M., Crocè, C. and Man- gioni, C. (2008) Systematic pelvic lympha-denectomy vs. no lymphad-enectomy in early-stage endometrial carcino- ma: Randomized clinical trial. Journal of the National Cancer Institute, 100(23), 1707- 1716. [66] Park, J.Y., Kim, E.N., Suh, D.S., Kim, J.H., Kim, Y.M., Kim, Y.T. and Nam, J.H. (2008) Comparison of the va- lidity of magnetic resonance imaging and positron emis- sion tomography/ computed tomography in the preopera- tive evaluation of patients with uterine corpus cancer. Gynecologic Oncology, 108(3), 486-492. [67] Kitajima, K., Murakami, K., Yamasaki, E., Fukasawa, I., Inaba, N., Kaji, Y. and Sugimura, K. (2008) Accuracy of 18F-FDG PET/CT in detecting pelvic and paraaortic lymph node metastasis in patients with endometrial can- cer. American Journal of Roentgenology, 190(6), 1652- 1658. [68] Inubashiri, E., Hata, K., Kanenishi, K., Shiota, A., Ohno, M., Yamamoto, Y., Nishiyama, Y., Ohkawa, M. and Hata, T. (2009) Positron emission tomography with the glucose ana lo g [F]-fluoro-2-deoxy-D-glu cose for evaluating pelvic lymph node metastasis in uterine corpus cancer: Com- parison with CT and MRI findings. The Journal of Ob- stetrics and Gynaecology Research, 35(1), 26-34. [69] Sironi, S., Picchio, M., Landoni, C., Galimberti, S., Si- gnorelli, M., Bettinardi, V., Perego, P., Mangioni, C., Messa, C. and Fazio, F. (2007) Post-therapy surveillance of patients with uterine cancers: Value of integrated 18F-FDG-PET/CT in the detection of recurrence. Euro- pean Journal of Nuclear Medicine and Molecular Imag- ing, 34(4), 472-479. [70] Kitajima, K., Murakami, K., Yamasaki, E., Hagiwara, S., Fukasawa, I., Inaba, N., Kaji, Y. and Sugimura, K. (2008) Performance of 18F-FDG-PET/CT in the diagnosis of recurrent endometrial cancer. Annals of Nuclear Medi- cine, 22(2), 103-109. [71] Ho, K.C., Lai, C.H., Wu, T.I., Ng, K.K., Yen, T.C., Lin, G., Chang, T.C., Wang, C.C., Hsueh, S. and Huang, H.J. (2008) 18F-fluoro-deoxyglucose positron emission to- mography in uterine carcinosarcoma. European Journal of Nuclear Medicine and Molecular Imaging, 35(3),  V. Pirro et al. / HEALTH 2 (2010) 652-660 Copyright © 2010 SciRes. http://www.scirp.org/journal/HEALTH/Openly accessible at 660 484-492. [72] Murakami, M., Tsukada, H., Shida, M., Watanabe, M., Maeda, H., Koido, S., Hirasawa, T., Muramatsu, T., Mi- yamoto, T., Nasu, S., Yasuda, S., Kajiwara, H. and Ya- suda, Ide, M. (2006) Whole-body positron emission to- mography with F18 fluorodeoxyglucose for the detection of recurrence in uterine sarcomas. International journal of gynecological Cancer, 16(2), 854-860. [73] Bastiaannet, E., Groen, H., Jager, P.L., Cobben, D.C., van der Graaf, W.T., Vaalburg, W. and Hoekstra, H.J. (2004) The value of 18F-FDG-PET in the detection, grading and response to therapy of soft tissue and bone sarcomas; a systematic review and meta-analysis. Cancer Treatment Reviews, 30(1), 83-101. [74] Rebollo, A.A.C., Ramos, F.C., Bellon G.M.E., Cabello G. D., Gallego P.M, Rodriguez, F.A. and Llamas E.J.M. (2007) Positron Emission Tomography with 18F-fluoro- deoxyglucose in patients with uterine sarcoma. Revista Española de Medicina Nuclear, 26(4), 189-195. [75] Nugent, E.K., Zighelboim, I., Case, A.S., Gao, F., Thaker, P.H., Rader, J.S., Mutch, D.G. and Massad, L.S. (2009) The value of perioperative imaging in patients with uter- ine sarcomas. Gynecologic Oncology, 115(1), 37-40. [76] Ho, K.C., Lai, C.H., Wu, T.I., Ng. K.K., Yen. T.C., Lin, G., Chang, T.C., Wang. C.C., Hsueh, S. and Huang, H.J. (2008) 18F-fluorodeoxyglucose positron emission tomo- graphy in uterine carcinosarcoma. European Journal of Nuclear Medicine and Molecular Imaging, 35(3), 484- 492. [77] Park, J.Y., Kim, E.N., Kim, D.Y., Suh, D.S., Kim, J.H., Kim, Y.M., Kim, Y.T. and Nam, J.H. (2008) Role of PET or PET/CT in the post-therapy surveillance of uterine sarcoma. Gynecologic Oncology, 109(2), 255-262. [78] Kizer, N.T., Zighelboim, I., Case, A.S., Dewdney, S.B., Thaker, P.H. and Massad, L.S. (2009) The role of PET/CT in the management of patients with cervical cancer: Practice patterns of the members of the Society of Gynecologic Oncologists. Gynecologic Oncology, 114(2), 310-314. ABBREVIATIONS PET: Positron Emission Tomography; CT: Computed Tomography; PET/CT: integrated PET/CT; CECT: Contrast Enhancement Computed Tomography; 18F-FDG: 18F-Fluoro-Deoxy-Glucose; Pap-test: Papanicolau screening test; FIGO: Federation of Gynaecologists and Obstetrics; MRI: Magnetic Resonance Imaging; SUVmax: Standardized Uptake Value; DFS: Disease Free Survival; GOG: Gynaecological Oncology Group; RT: Radiotherapy; CEA: Carcinoembryonic Antigen; CA 19.9: Carbohydrate Antigen 19.9; CA 125: Carbohydrate Antigen 125; NPV: Negative Predictive Value; US: Ultrasonography
|