M. Eskandar et al. / Open Journal of Obstetrics and Gynecology 2 (2012) 265-269
268
rare uterine rupture (0.15%) when labor was spontaneous
without augmentation [12]. The reasonable explanation
is that the interval since the Previous Cesarean Section
(PCS) in the present study was long (Tabl e 2 ), our pa-
tients came in spontaneous labor and augmentation with
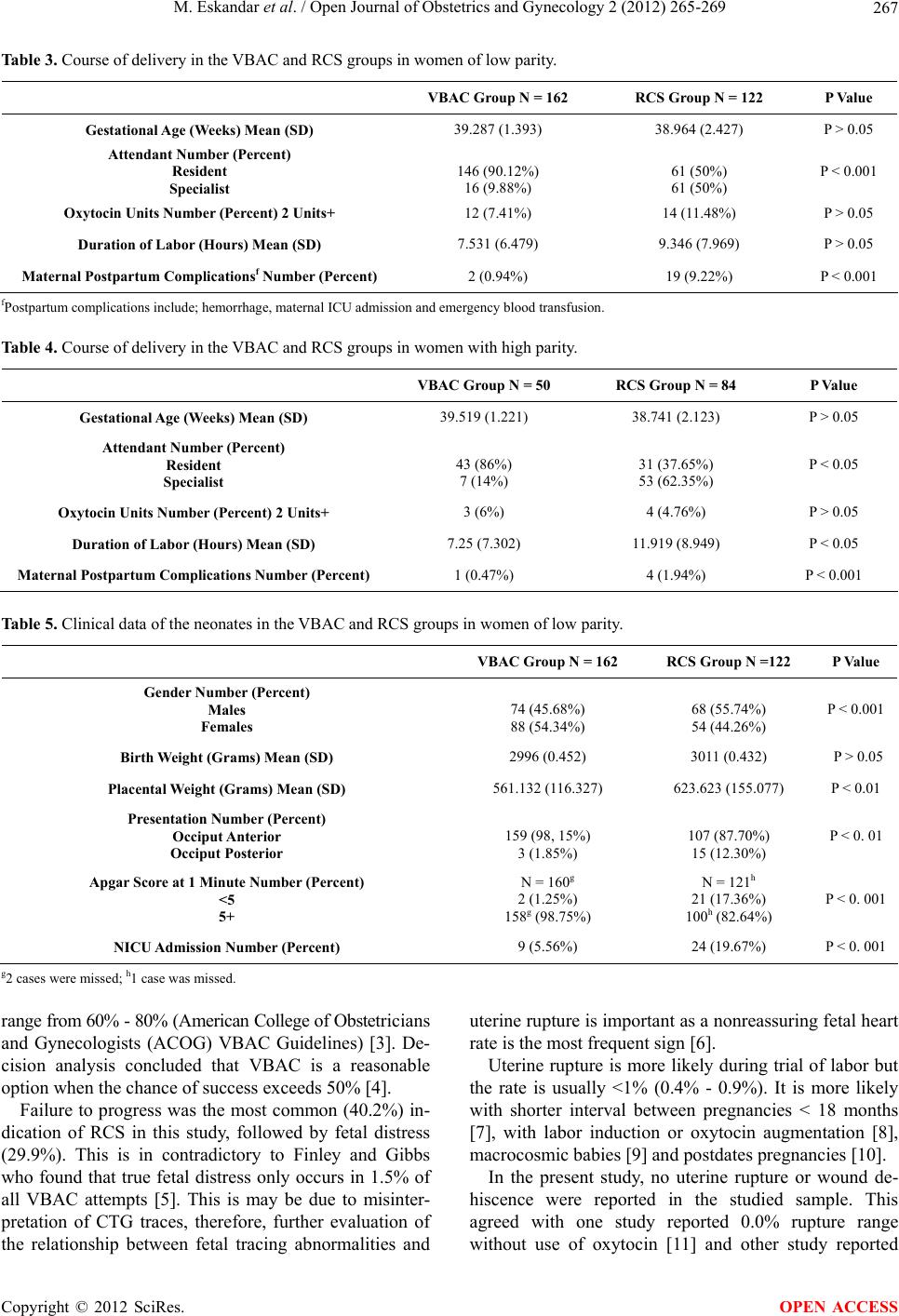
Oxytocin was used in small dose only in 7.4% - 11.5% of
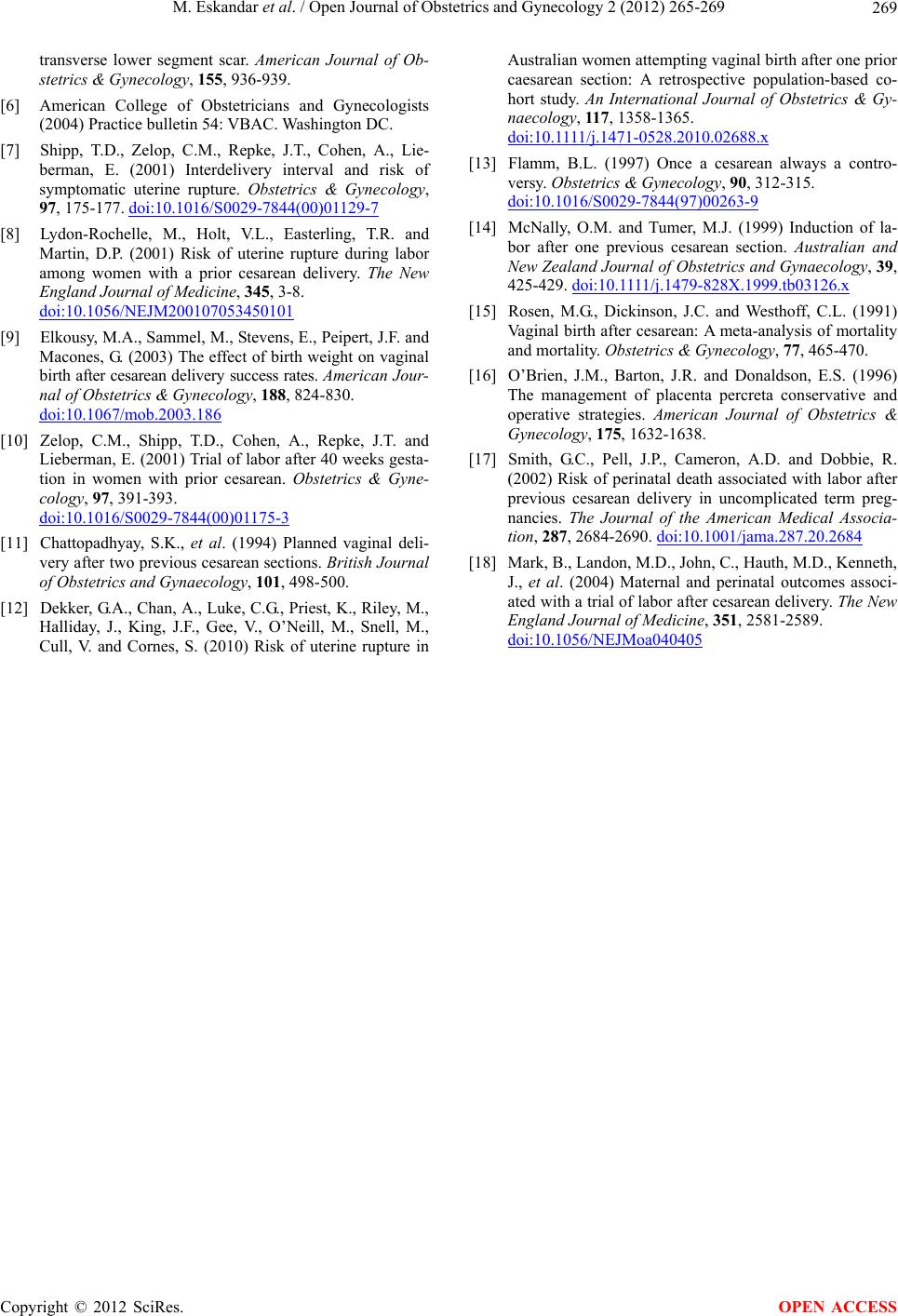
patients (Ta b l e 3 ). Also we have no postdates (Ta bl e 4)
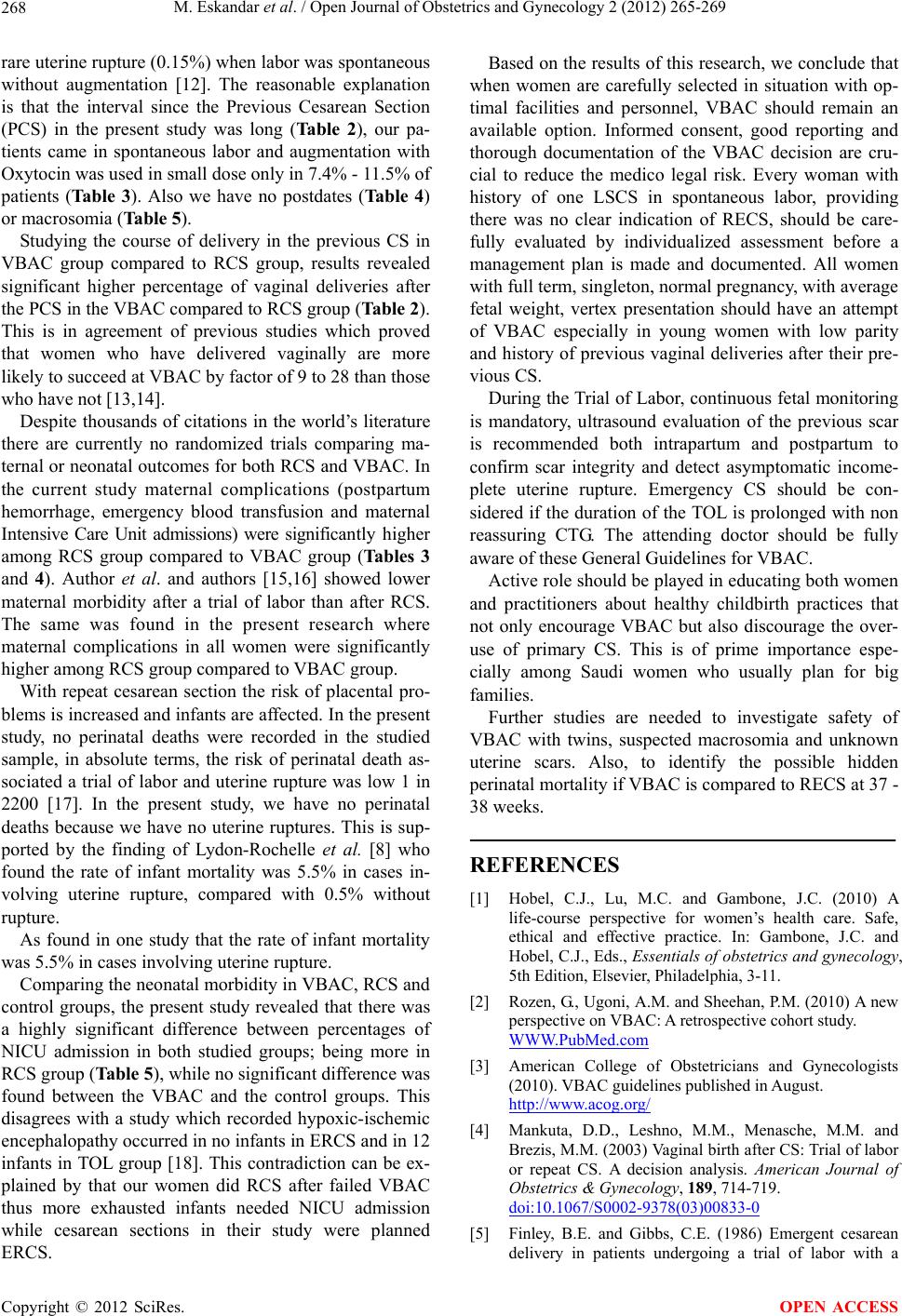
or macrosomia (Table 5).
Studying the course of delivery in the previous CS in
VBAC group compared to RCS group, results revealed
significant higher percentage of vaginal deliveries after
the PCS in the VBAC compared to RCS group (Table 2).
This is in agreement of previous studies which proved
that women who have delivered vaginally are more
likely to succeed at VBAC by factor of 9 to 28 than those
who have not [ 13,14].
Despite thousands of citations in the world’s literature
there are currently no randomized trials comparing ma-
ternal or neonatal outcomes for both RCS and VBAC. In
the current study maternal complications (postpartum
hemorrhage, emergency blood transfusion and maternal
Intensive Care Unit admissions) were significantly higher
among RCS group compared to VBAC group (Ta b le s 3
and 4). Author et al. and authors [15,16] showed lower
maternal morbidity after a trial of labor than after RCS.
The same was found in the present research where
maternal complications in all women were significantly
higher among RCS group compared to VBAC group.
With repeat cesarean section the risk of placental pro-
blems is increased and infants are affected. In the present
study, no perinatal deaths were recorded in the studied
sample, in absolute terms, the risk of perinatal death as-
sociated a trial of labor and uterine rupture was low 1 in
2200 [17]. In the present study, we have no perinatal
deaths because we have no uterine ruptures. This is sup-
ported by the finding of Lydon-Rochelle et al. [8] who
found the rate of infant mortality was 5.5% in cases in-
volving uterine rupture, compared with 0.5% without
rupture.
As found in one study that the rate of infant mortality
was 5.5% in cases involving uterine rupture.
Comparing the neonatal morbidity in VBAC, RCS and
control groups, the present study revealed that there was
a highly significant difference between percentages of
NICU admission in both studied groups; being more in
RCS group (Table 5), while no significant difference was
found between the VBAC and the control groups. This
disagrees with a study which recorded hypoxic-ischemic
encephalopathy occurred in no infants in ERCS and in 12
infants in TOL group [18]. This contradiction can be ex-
plained by that our women did RCS after failed VBAC
thus more exhausted infants needed NICU admission
while cesarean sections in their study were planned
ERCS.
Based on the results of this research, we conclude that
when women are carefully selected in situation with op-
timal facilities and personnel, VBAC should remain an
available option. Informed consent, good reporting and
thorough documentation of the VBAC decision are cru-
cial to reduce the medico legal risk. Every woman with
history of one LSCS in spontaneous labor, providing
there was no clear indication of RECS, should be care-
fully evaluated by individualized assessment before a
management plan is made and documented. All women
with full term, singleton, normal pregn an cy, with average
fetal weight, vertex presentation should have an attempt
of VBAC especially in young women with low parity
and history of previous vaginal deliveries after their pre-
vious CS.
During the Trial of Labor, continuous fetal monitoring
is mandatory, ultrasound evaluation of the previous scar
is recommended both intrapartum and postpartum to
confirm scar integrity and detect asymptomatic income-
plete uterine rupture. Emergency CS should be con-
sidered if the duration of the TOL is prolonged with non
reassuring CTG. The attending doctor should be fully
aware of these General Guidelines for VBAC.
Active role should be played in educating both women
and practitioners about healthy childbirth practices that
not only encourage VBAC but also discourage the over-
use of primary CS. This is of prime importance espe-
cially among Saudi women who usually plan for big
families.
Further studies are needed to investigate safety of
VBAC with twins, suspected macrosomia and unknown
uterine scars. Also, to identify the possible hidden
perinatal mortality if VBAC is compared to RECS at 37 -
38 weeks.
REFERENCES
[1] Hobel, C.J., Lu, M.C. and Gambone, J.C. (2010) A
life-course perspective for women’s health care. Safe,
ethical and effective practice. In: Gambone, J.C. and
Hobel, C.J., Eds., Essentials of obstetrics and gynecology,
5th Edition, Elsevier, Philadelphia, 3-11.
[2] Rozen, G., Ugoni, A.M. and Sheehan, P.M. (2010) A new
perspective on VBAC: A retrospective cohort study.
WWW.PubMed.com
[3] American College of Obstetricians and Gynecologists
(2010). VBAC guidelines published in August.
http://www.acog.org/
[4] Mankuta, D.D., Leshno, M.M., Menasche, M.M. and
Brezis, M.M. (2003) Vaginal birth after CS: Trial of labor
or repeat CS. A decision analysis. American Journal of
Obstetrics & Gynecology, 189, 714-719.
doi:10.1067/S0002-9378(03)00833-0
[5] Finley, B.E. and Gibbs, C.E. (1986) Emergent cesarean
delivery in patients undergoing a trial of labor with a
Copyright © 2012 SciRes. OPEN ACCESS