Open Journal of Obstetrics and Gynecology, 2012, 2, 244-246 OJOG
http://dx.doi.org/10.4236/ojog.2012.23050 Published Online September 2012 (http://www.SciRP.org/journal/ojog/)
Cesarean scar abscess: A case repor t and a review of
the literature*
Takako Taguchi1, Seiji Mabuchi1#, Toshio Kimura2, Tadashi Kimura1
1Department of Ob s tetrics and Gynecology, Osaka University Graduate School of Medicine, Suita, Japan
2Department of Gynecology, Ashiya Municipal Hospi t a l , Ashiya, Japan
Email: #smabuchi@gyne.med.osaka-u.ac.jp
Received 4 May 2012; revised 8 June 2012; accepted 20 June 2012
ABSTRACT
Cesarean section and the resultant Cesarean scar are
known to be associated with obstetric complications
in subsequent pregnancies. Cesarean scar is also as-
sociated with gynecological conditions that can ad-
versely affect the patient’s quality of life. We describe
a very rare case of Cesarean scar abscess that deve-
loped 8 years after a Cesarean delivery, which was
managed by emergency hysterectomy.
Keywords: Cesarean Section; Cesarean Scar Dehiscence;
Abscess
1. INTRODUCTION
The increasing rates of Cesarean section and its compli-
cations are global issues in developed countries. Cesa-
rean section and the resultant Cesarean scar in the lower
uterine segment are known to be associated with obstet-
ric complications in subsequent pregnancies, such as
uterine rupture; Cesarean scar pregnancy (CSP); placenta
previa; and placenta accreta, increta, or percreta. Cesar-
ean scars are also associated with gynecological condi-
tions that can ad versely affect the patient’s quality of life,
e.g., abnormal uterine bleeding, chronic pain, or secon-
dary infertility [1].
We herein describe a very rare case of Cesarean scar
abscess that developed 8 years after a Cesarean delivery,
which was m a naged by emergency hysterectomy.
2. CASE REPORT
A 44-year-old Japanese woman (gravida 1, para 1) visited
our hospital complaining of abdominal pain that had
lasted for 2 weeks accompanied by uterine bleeding. Her
obstetric history included a lower uterine segment trans-
verse Cesarean section 8 years earlier. Her medical his-
tory was unremarkable. Physical examinations including
pelvic examination revealed a body temperature of 39˚C,
marked bloody cervical discharge with an odious smell,
cervical motion tenderness, and lower abdominal ten-
derness, but no rebound tenderness. Transvaginal ultra-
sonography showed a normal-sized uterus with an 8 × 7
cm spherical mass in the lower uterine segment, which
was located on the scar cau sed by the previous Cesarean
section. The inner part of the mass was irregular (both
hyperechogenic and anechogenic). Both ovaries were
normal, and there was no intraperitoneal fluid. Labora-
tory tests revealed an elevated white blood cell count
(12,120/mm3), an elevated C-reactive protein level (14.9
mg/dl), and a negative pregnancy test result. She was
admitted, and initial treatment with antibiotics was per-
formed on the same day. A subsequent pelvic magnetic
resonance imaging (MRI) examination revealed an 11 ×
10 × 9 cm exophytic tumor in the lower uterine segment.
Both transvaginal ultrasonography and pelvic MRI sug-
gested that the tumor was connected to the uterine cavity
through a small defect in the lower anterior wall of the
uterus, which might have been a Cesarean scar defect. A
diagnosis of Cesarean scar abscess was suspected. As her
infectious symptoms progressed and she did not want to
preserve her fertility, we offered her abdominal hyste-
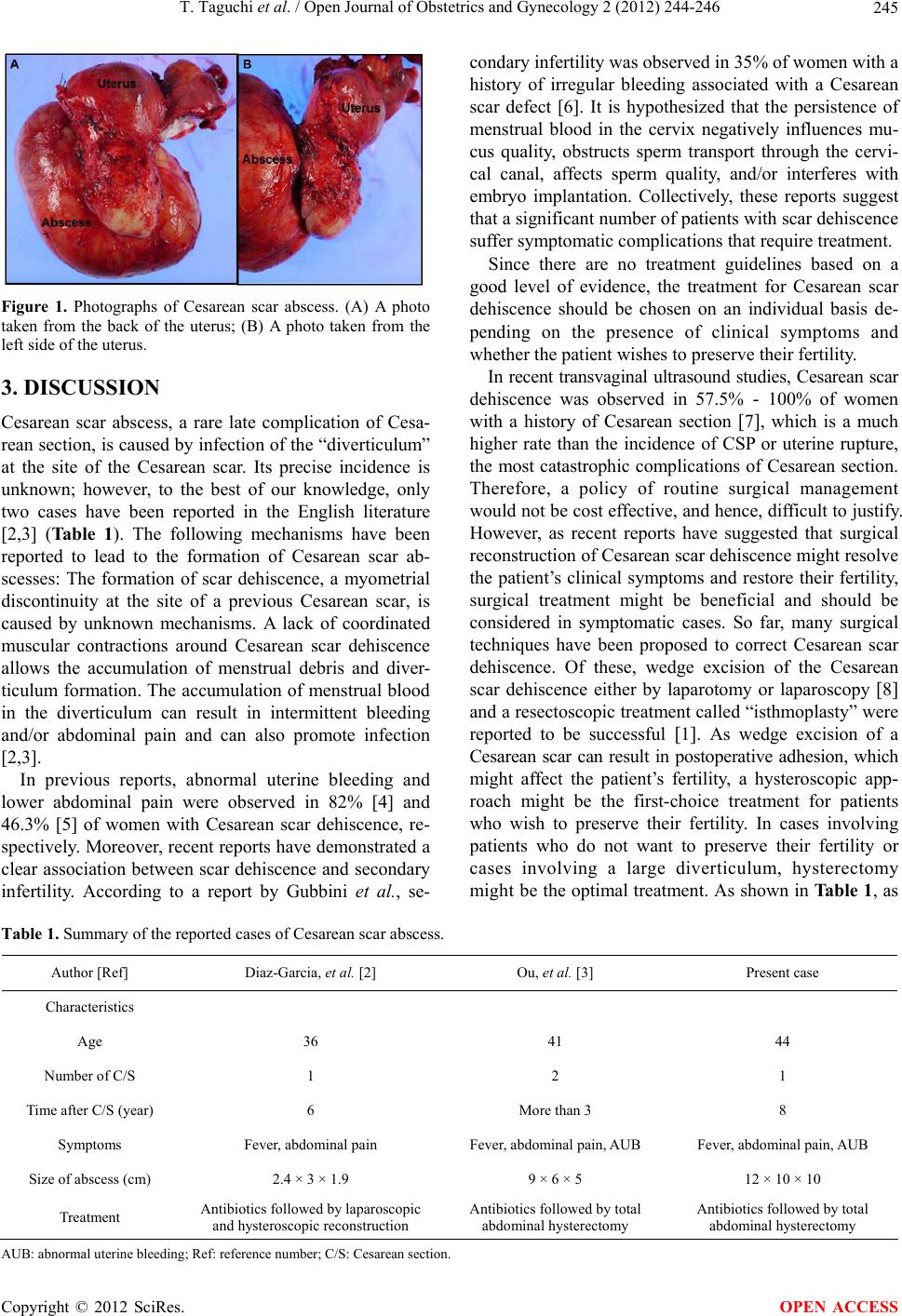
rectomy. Exploratory laparotomy revealed a 12 × 10 × 10
cm elastic mass arising from the lower anterior uterine
wall, which was adherent to the right pelvic sidewall, and
total abdominal hysterectomy was performed (Figure 1).
Grossly, the mass contained bloody purulent discharge
and was connected to the uterine cavity by a thin piece of
tissue. A pathological examination showed a bundle-like
mass of muscle tissue without any findings of degene-
rated leiomyoma. The cavity of the tumor and the tissue
connecting it to th e uterus were lined with colu mnar cells
resembling those found in the endocervical epithelium.
Culturing of the abscess contents produced Enterobacter
cloacae. The diagnosis of Cesarean scar abscess was
confirmed. The patient received intravenous antibiotics
for 2 days after the surgery and was discharged.
*Conflicts of Interest Statement: The authors declare that no conflicts
of interest exist.
#Corresponding author.
OPEN ACCESS