M. Fatemeh, E. B. Nazanin / Open Journal of Obstetrics and Gynecology 2 (2012) 230-234 233
in Saudi Arabia in 2008 no significant difference was
confirmed for fetal complications between epileptic and
non-epileptic women [12].
Regarding maternal complications, in 15 patients
(30.0%) no complication was found, in 2 cases (4.0%)
PIH, in 12 cases (24.0%) PLP, in 4 cases (8.0%) bleeding,
in 14 cases (28.0%) PROM and in 3 cases (6.0%) other
complications were detected. In a study by Thomas SV,
et al in India in 2008, it was illustrated that spontaneous
miscarriage, anemia and seizure are the most important
complications in pregnant women [13]. In other study by
Kats O., et al. in Israel in 2006, high rate of gestational
diabetes and congenital malformation was reported in
epileptic pregnant women [14]. In our study we also
found a considerable rate (74.0%) of cesarean section. In
a study by Richmond J.R., et al. in Canada in 2004, it
was revealed that the rate of PIH which required induc-
tion and fetal malformation is high in epileptic women;
we also found some cases of PIH in our study. In contrast
to our findings, in a study by Saleh A.M., et al. in Saudi
Arabia in 2008 no significant difference was detected for
maternal complications in epileptic and non-epileptic
women, they had totally 4 cases of seizure and 2 cases of
fetal disorders [12].
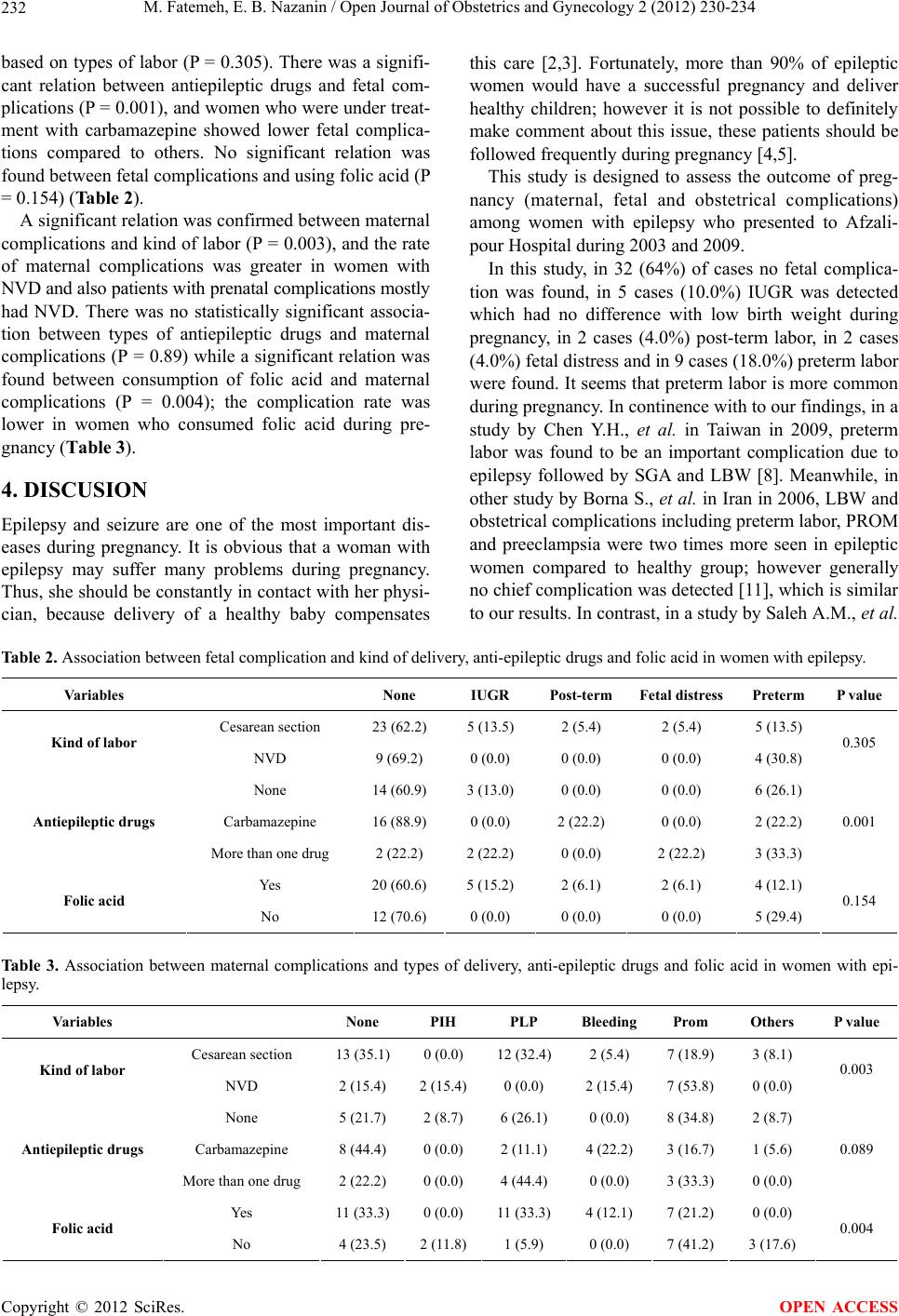
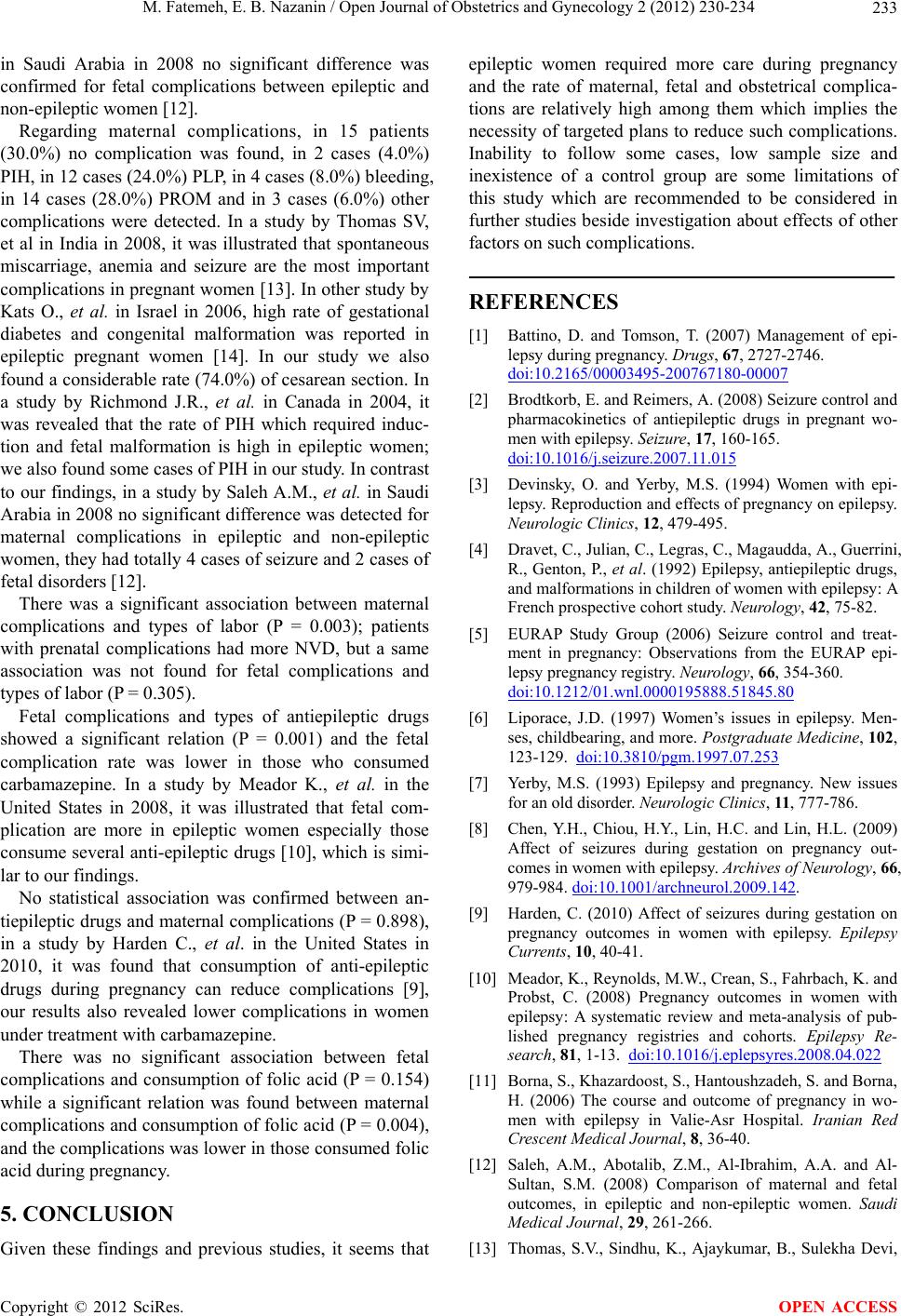
There was a significant association between maternal
complications and types of labor (P = 0.003); patients
with prenatal complications had more NVD, but a same
association was not found for fetal complications and
types of labor (P = 0.305).
Fetal complications and types of antiepileptic drugs
showed a significant relation (P = 0.001) and the fetal
complication rate was lower in those who consumed
carbamazepine. In a study by Meador K., et al. in the
United States in 2008, it was illustrated that fetal com-
plication are more in epileptic women especially those
consume several anti-epileptic drugs [10], which is simi-
lar to our findings.
No statistical association was confirmed between an-
tiepileptic drugs and maternal complications (P = 0.898),
in a study by Harden C., et al. in the United States in
2010, it was found that consumption of anti-epileptic
drugs during pregnancy can reduce complications [9],
our results also revealed lower complications in women
under treatment with carbamazepine.
There was no significant association between fetal
complications and consumption of folic acid (P = 0.154)
while a significant relation was found between maternal
complications and consumption of folic acid (P = 0.004),
and the complications was lower in those consumed folic
acid during pregnancy.
5. CONCLUSION
Given these findings and previous studies, it seems that
epileptic women required more care during pregnancy
and the rate of maternal, fetal and obstetrical complica-
tions are relatively high among them which implies the
necessity of targeted plans to reduce such complications.
Inability to follow some cases, low sample size and
inexistence of a control group are some limitations of
this study which are recommended to be considered in
further studies beside investigation about effects of other
factors on such complications.
REFERENCES
[1] Battino, D. and Tomson, T. (2007) Management of epi-
lepsy during pregnancy. Drugs, 67, 2727-2746.
doi:10.2165/00003495-200767180-00007
[2] Brodtkorb, E. and Reimers, A. (2008) Seizure control and
pharmacokinetics of antiepileptic drugs in pregnant wo-
men with epilepsy. Seizure, 17, 160-165.
doi:10.1016/j.seizure.2007.11.015
[3] Devinsky, O. and Yerby, M.S. (1994) Women with epi-
lepsy. Reproduction and effects of pregnancy on epilepsy.
Neurologic Clinics, 12, 479-495.
[4] Dravet, C., Julian, C., Legras, C., Magaudda, A., Guerrini,
R., Genton, P., et al. (1992) Epilepsy, antiepileptic drugs,
and malformations in children of women with epilepsy: A
French prospective cohort study. Neurology, 42, 75-82.
[5] EURAP Study Group (2006) Seizure control and treat-
ment in pregnancy: Observations from the EURAP epi-
lepsy pregnancy registry. Neurology, 66, 354-360.
doi:10.1212/01.wnl.0000195888.51845.80
[6] Liporace, J.D. (1997) Women’s issues in epilepsy. Men-
ses, childbearing, and more. Postgraduate Medicine, 102,
123-129. doi:10.3810/pgm.1997.07.253
[7] Yerby, M.S. (1993) Epilepsy and pregnancy. New issues
for an old disorder. Neurologic Clinics, 11, 777-786.
[8] Chen, Y.H., Chiou, H.Y., Lin, H.C. and Lin, H.L. (2009)
Affect of seizures during gestation on pregnancy out-
comes in women with epilepsy. Archives of Neurology, 66,
979-984. doi:10.1001/archneurol.2009.142.
[9] Harden, C. (2010) Affect of seizures during gestation on
pregnancy outcomes in women with epilepsy. Epilepsy
Currents, 10, 40-41.
[10] Meador, K., Reynolds, M.W., Crean, S., Fahrbach, K. and
Probst, C. (2008) Pregnancy outcomes in women with
epilepsy: A systematic review and meta-analysis of pub-
lished pregnancy registries and cohorts. Epilepsy Re-
search, 81, 1-13. doi:10.1016/j.eplepsyres.2008.04.022
[11] Borna, S., Khazardoost, S., Hantoushzadeh, S. and Borna,
H. (2006) The course and outcome of pregnancy in wo-
men with epilepsy in Valie-Asr Hospital. Iranian Red
Crescent Medical Journal, 8, 36-40.
[12] Saleh, A.M., Abotalib, Z.M., Al-Ibrahim, A.A. and Al-
Sultan, S.M. (2008) Comparison of maternal and fetal
outcomes, in epileptic and non-epileptic women. Saudi
Medical Journal, 29, 261-266.
[13] Thomas, S.V., Sindhu, K., Ajaykumar, B., Sulekha Devi,
Copyright © 2012 SciRes. OPEN ACCESS