A. Sebastian et al. / Open Journal of Obstetrics and Gynecology 2 (2012) 220-222 221
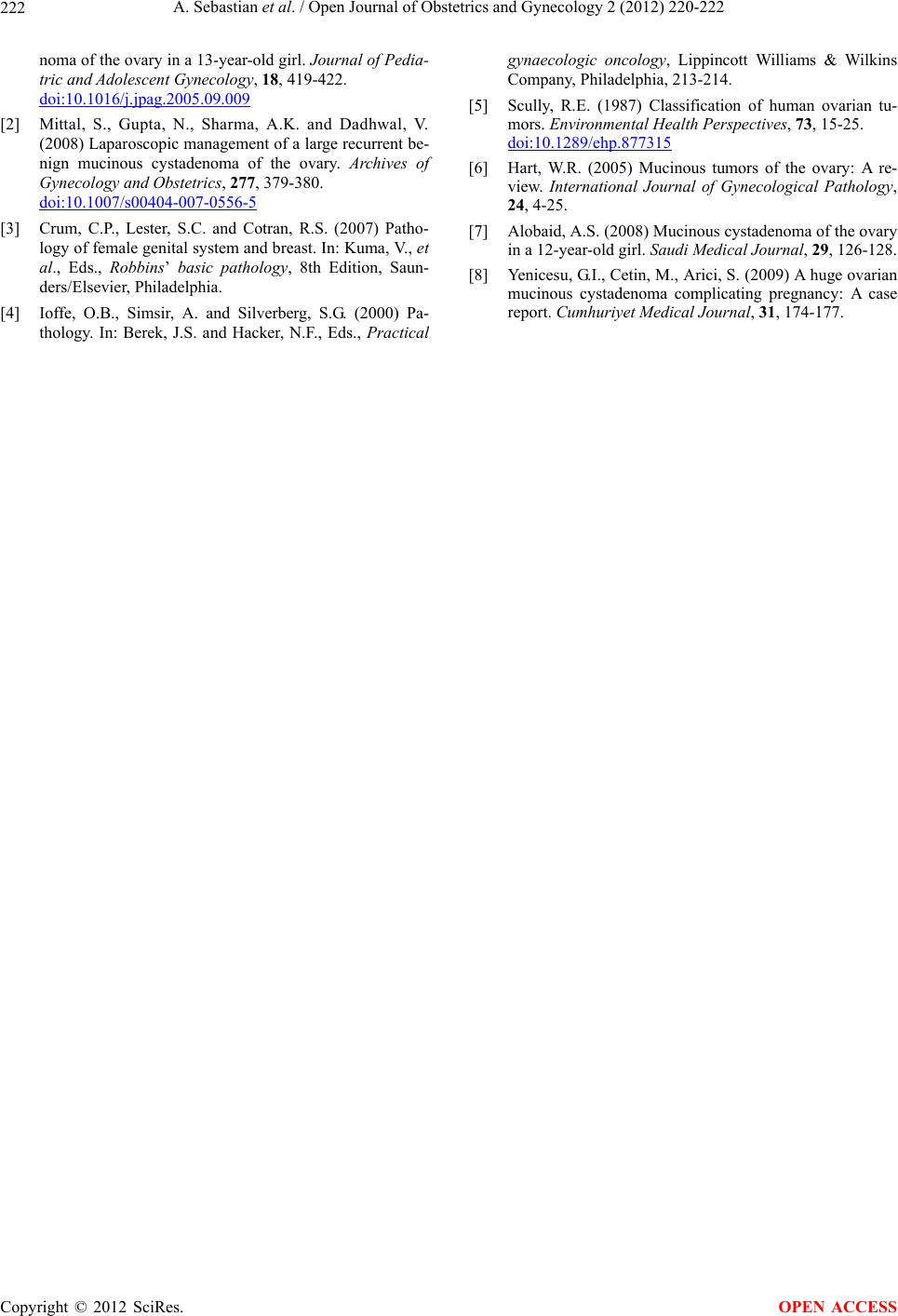
pushing the liver, bowel and spleen upwards (Figure 2).
The specimen after decompression weighed 5 kg with
multiple solid and cystic areas. The uterus and other
ovary were normal. Bilateral ureteric stenting was also
done.
Post operatively patient was managed in intensive care
unit for a day and transfused one unit of blood. She
weighed 38 kg post operatively and had a uneventful
post operative period. She was discharged on the 6th post
operative day. Patient was advised to follow up after 6
weeks for ureteric stent removal. The biopsy was re-
ported as benign mucinous cystadenoma .She recovered
completely from her surgery and has gone back to her
normal daily activity as a daily wages worker.
3. DISCUSSION
There are four major categories of ovarian tumors:
1) Epithelial tumors (65% - 75%)—serous or muci-
nous cystadenoma/carcinoma, clear cell carcinoma, Br en-
ner tumor;
2) Germ cell tumors (15%)—dysgerminoma, embryo-
nal cell cancer, choriocarcinoma, teratoma;
3) Sex-chord-stromal tumors (5% - 10%)—granulosa
cell tumor, thecoma, fibroma;
4) Metastatic tumors (10%)—uterine, stomach, colon,
breast, lymphoma [5].
These tumors are usually evaluated using ultrasound,
CT scan, or MRI. Findings on imaging studies are non-
specific. These ovarian tumors may be multi-septated,
cystic masses with thin walls. They may contain varying
amounts of solid tissue which consists of proliferating
stromal tissue, papillae, or malignant tumor cells. Tu-
mour markers may also aid us in telling us the origin of
the tumour.
Mucinous cystadenomas are divided into three catego-
ries: benign, borderline, and malignant. Survival is
largely dependent on the histology of the tumor, with a
Figure 2. Cut section of the large ovarian tumour.
10 year survival rate of 100% for benign tumors, 60% for
borderline tumors, and only 34% for the malignant sub-
type. Benign mucinous tumors tend to present earlier,
while malignant tumors are often seen later in life.
Benign mucinous cystadenomas comprise 80% of
mucinous ovarian tumors and 20% - 25% of benign
ovarian tumors overall. The peak incidence occurs be-
tween 30 - 50 years of age. Benign tumors are bilateral in
5% - 10% of cases.
Borderline mucinous cystadenomas make up about
10% of mucinous ovarian neoplasm’s and are bilateral in
10% of cases.
Malignant mucinous cystadenoms are rare, and en-
compass 10% of mucinous ovarian tumors and 5% - 10%
of primary malignant ovarian neoplasms overall. They
are bilateral in 15% - 30% of cases and have a peak in-
cidence between 40 - 70 years of age.
Giant ovarian tumours have become rare in current
medical practice, as most cases are discovered early dur-
ing routine check-ups. Detection of ovarian cysts causes
considerable worry for women because of fear of malig-
nancy, but fortunately the majority of ovarian cysts are
benign. These giant tumours may be associated with
pressure symptoms, urinary tract changes, respiratory
embarrassment and debilitation. While operating on su ch
tumours care has to be taken to manage these complica-
tions as well as the problems associated with sudden de-
compensation of such large tumours.
Histologically, mucinous cystadenoma is lined by tall
columnar non-ciliated epithelial cells with apical mucin
and basal nuclei. 80% tumours are cystadenomas while
the remaining 20% is of the borderline variety, noninva-
sive (intraglandular; intraepithelial) carcinomas, or inva-
sive carcinomas. The borderline tumors may be of intes-
tinal type or mullerian (endocervical-like) type. The in-
testinal-type tumors are by far the most common [6].
Mucinous cystadenoma is a benign ovarian tumor. It is
reported to occur in middle-aged women. It is rare
among adolescents [7] or in association with pregnancy
[8]. On gross appearance, mucinous tumors are charac-
terised by cysts of variable sizes without surface invasion.
Only 10% of primary mucinous cystadenoma is bilateral
[7]. In our case, the tumor was unilateral, affecting the
left ovary. The cyst was filled with sticky gelatinous fluid
rich in glycoprotein.
Management of ovarian cysts depends on the patient’s
age, the size of the cyst and its histo-pathological nature.
Conservative surgery as ovarian cystectomy and salpingo-
oophorectomy is adequate for benign lesions [7].
REFERENCES
[1] Vi zza, E., Galati, G.M., Corrado, G., Atlante, M., Infante,
C. and Sbiroli, C. (2005) Voluminous mucinous cystade-
Copyright © 2012 SciRes. OPEN ACCESS