A. Yoshida et al. / Open Journal of Obstetrics and Gynecology 2 (2012) 202-205
204
methods [4,6]. Epidural analgesia with morphine was
thought to increase post-cesarean urinary retention [6].
Not only cesarean section, but also post surgical epi-
dural analgesia is often complicated by urinary retention,
which usually disappears shortly after the discontinuance
of analgesics [7]. Therefore, it was thought to be unlikely
that urinary retention in this case was directly caused by
epidural analgesia. On the other hand, inserting or re-
moving epidural catheter may cause an epidural hema-
toma, which can lead to urinary retention. Epidural he-
matoma caused by epidural catheter is usually associated
with bleeding tendency in patients with complications
such as coagulopathy, liver disease or anticoagulant
medications. In our hospital, subcutaneous injection of
heparin is used for preventing postoperative venous
thrombosis in almost all cesarean cases but in the heparin
administered cases, the epidural catheter is removed at
least 4 hours after heparin injection. In this case of post-
operative heparin injection the epidural catheter was re-
moved after 5 hours of last heparin. Therefore, the possi-
bility of an epidural hematoma caused by removal of the
epidural catheter was not thought to be strong, but an
epidural hematoma formation in a patient ordinary with-
out bleeding tendency is reported [8]. Epidural hema-
toma is usually thought to be formed shortly after inser-
tion or removal of epidural catheter, but the formation of
epidural hematoma 9 days after removal of the epidural
catheter is reported [9]. In our case, urinary retention
occurring 6 days after the insertion and 4 days after the
removal of the epidural catheter could not readily rule
out the relationship between urinary retention and hema-
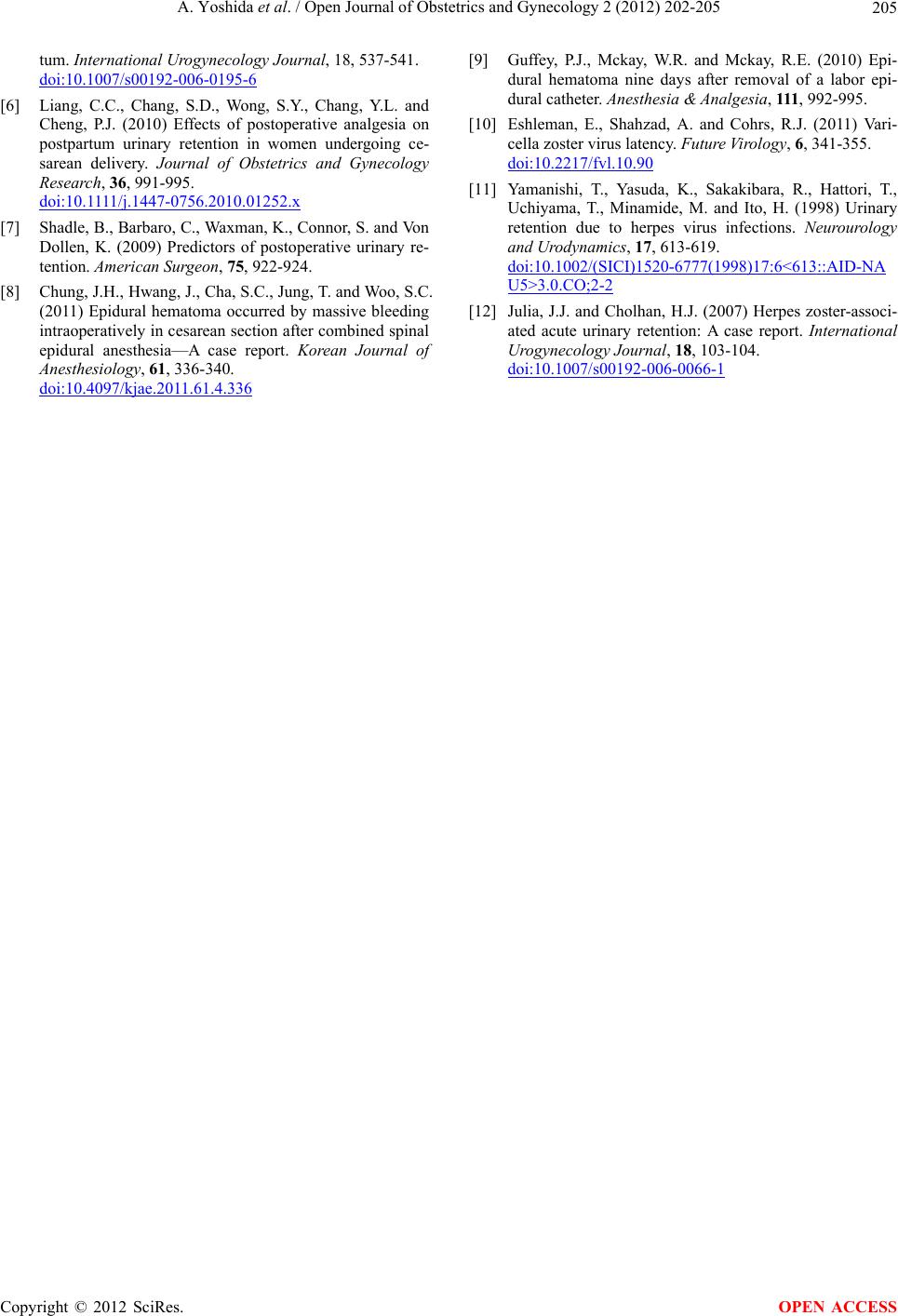
toma by the epidural catheter. Spinal MRI was obtained
immediately, but no epidural hematoma or other mass
which might be compressing the spinal nerves was noted.
Herpes zoster is an infection caused by varicella zoster
virus. The primary infection with varicella zoster virus
develops as varicella (chicken pox) and results in in-
flammatory lesion of the sensory root ganglions, menin-
ges or spinal cord. After the primary infection, the virus
enters the latent phase and remains dormant indefinitely.
The reactivation and proliferation of the virus may recur
as herpes zoster. It is reported that herpes zoster is
reactivated by various factors such as advanced age,
physical or psychological stress, general fatigue, trauma,
common cold or impaired immunity in patients on ste-
roids, malignant tumors or anticancer drugs [10]. In our
current case, the patient was suspected to be at high risk
for herpes zoster because she was in the postoperative
period with fatigue and physical and psychological
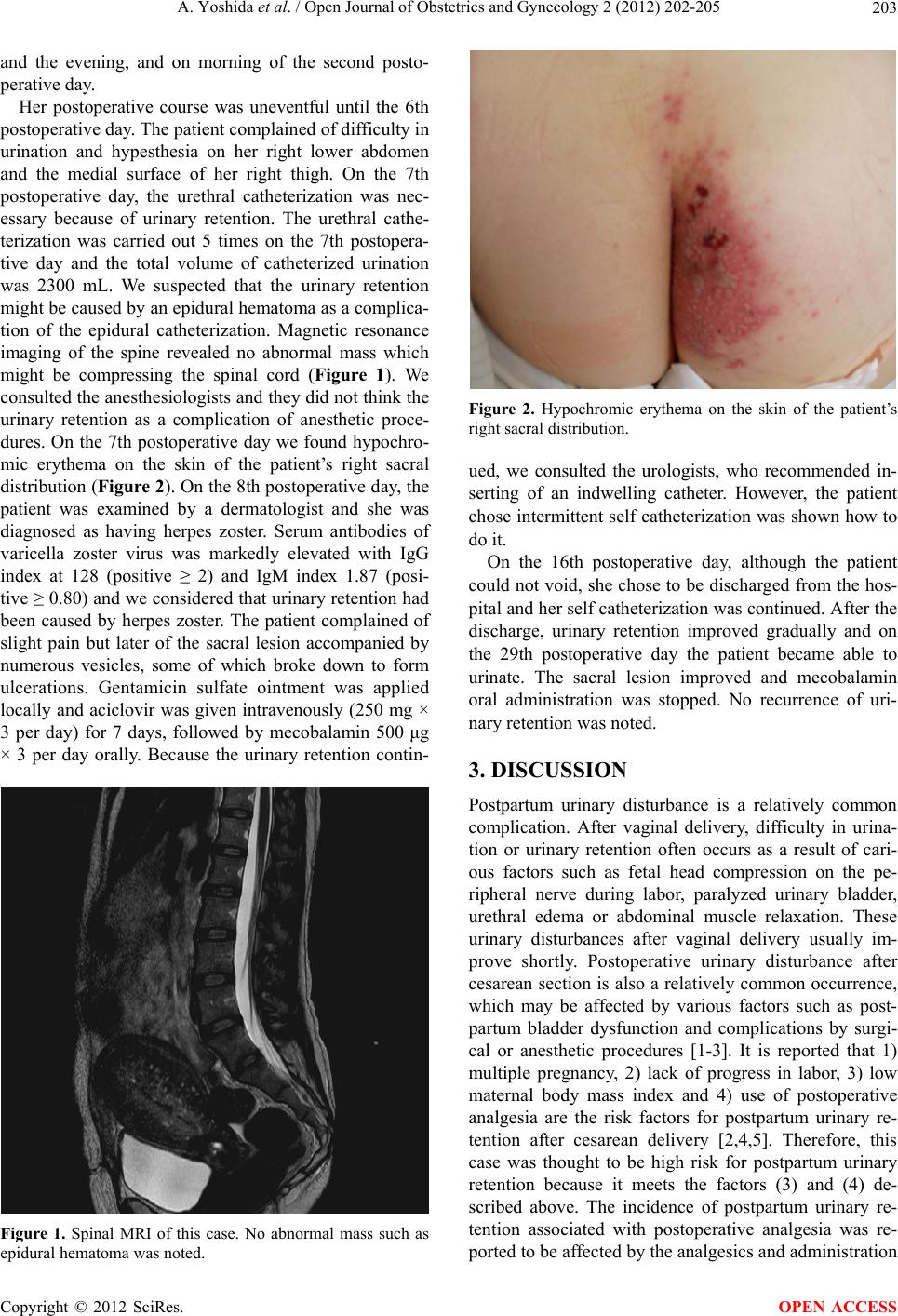
stresses. Usually herpes zoster is complicated by sever
pain along the innervations, although in this case the
patient complained little pain. Gluteal cutaneous lesion
in this case was considered to be innervation area of the
sacral nerve. Urinary retention is a common complica-
tion of zoster [11]. Sacral herpes zoster is thought to
induce detrusor areflexia by an inflammatory reaction,
which begins in the dorsal root ganglia and spreads to the
sacral segments of the spinal cord, and causes urinary
retention as the result, but it is reported that lumber or
thoracic zoster may cause urinary retention [12]. Sacral
herpes may also cause rectal disorders, but in this case
her rectal function was intact. In the therapy of zoster,
prompt use of antiviral agents is very important. It is
preferable to start antiviral agents within 72 hours of
cutaneous-lesion outbreak. In this case, accurate time of
onset of the erythema was unclear, but we could start
aciclovir within two days of urinary retention, which was
thought to be relatively early initiation of antiviral
therapy. In the drug package insert (in this case we used
VICCLOX I.V. Infusion 250 mg by Kobayashi Kako Co.
Ltd. Japan), concerning the use of aciclovir during the
lactation period, it is written that “nursing mothers should
discontinue breast feeding during treatment (transfer of
this drug into breast milk has been reported).” However,
Japan Drug Information Institute in Pregnancy (JDIP) in
National Center for Child Health and Development
announces that use of aciclovir is thought to be safe
during nursing period. In our case, we explained to the
patient the product document and the announcement by
JDIP. After obtaining the informed consent, nursing was
continued and no particular problems were noted.
4. ACKNOWLEDGEMENTS
I am deeply grateful to Dr. Mitsunao Kobayashi who provided helpful
comments and suggestions.
REFERENCES
[1] Kermans, G., Wyndaele, J.J., Thiery, M. and DeSy, W.
(1986) Puerperal urinary retention. Acta Urologica Bel-
gica, 54, 376-385.
[2] Evron, S., Samueloff, A., Simon, A., Drenger, B. and
Magora, F. (1985) Urinary function during epidural anal-
gesia with methadone and morphine in post-cesarean sec-
tion patients. Pain, 23, 135-144.
doi:10.1016/0304-3959(85)90055-7
[3] Dray, A. and Metsch, R. (1984) Inhibition of urinary
bladder contractions by a spinal action of morphine and
other opioids. Journal of Pharmacology and Experimen-
tal Therapeutics , 231, 254-260.
[4] Chai, A.T., Wong, T., Mak, H.L.J., Cheon, C., Yip, S.K.
and Wong, A.S.M. (2008) Prevalence and associated risk
factors of retention of urine after cesarean section. Inter-
national Urogynecology Journal, 19, 537-542.
doi:10.1007/s00192-007-0470-1
[5] Liang, C.C., Tseng, L.H., Horng, S.G., Lin, I.W. and
Chang, S.D. (2007) Correlation of pelvic organ prolapse
quantification system scores with obstetric parameters
and lower urinary tract symptoms in primiparae postpar-
Copyright © 2012 SciRes. OPEN ACCESS