Health
Vol.6 No.5(2014), Article ID:43273,6 pages DOI:10.4236/health.2014.65062
Monthly admissions for heart failure (HF)— Environmental links
![]()
1Division of Cardiology, Rabin Medical Center, Petah Tiqwa, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; stoupel@inter.net.il
2Managing Information Unit, Rabin Medical Center, Petah Tiqwa, Israel
3Biostatistics M.S., New York, USA
Copyright © 2014 Eliyahu Stoupel et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property Eliyahu Stoupel et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received 30 December 2013; revised 26 January 2014; accepted 3 February 2014
KEYWORDS
Monthly; Admissions; Heart; Failure; Male; Female; Solar; Geomagnetic; Cosmic; Ray Neutron; Activity
ABSTRACT
In recent years the role of HF in the outcomes, cost of treatment in cardiology is raising. Concomitantly a number of studies were published demonstrating connections of many cardiac events with Space Weather Activity-Solar, Geomagnetic, Cosmic Ray (Neutron) activity levels. The aim of this study was to study links of timing of hospital admissions for HF with season and space weather components. Patients and Methods: monthly admissions of male and female patients for HF in two hospitals of Rabin Medical Center for years 2000-2012 were the subject of the study. 76,601 patient were included, 42,293 men, 34,308 woman. The cosmophysical data from USA, Russia and Finland were used. Results: Monthly average number of admissions for HF: 491.0 ± 82.4, 271.1 ± 46.75 for men and 219.9 ± 39.8 for woman. Gender admissions strongly correlated. Monthly admission for HF number differed by 2.2 - 2.5 times. Minimal admissions were in August, September; maximal—in January, February, December and March (according to numbers). It was a significant inverse correlation of monthly HF admissions with monthly solar activity and GMA indices and correlation with CRA (neutron) activity. Conclusion: Monthly admissions number for HF is fluctuated by season of the year, depending on gender and related to monthly solar and Cosmic Ray (Neutron) activity level. Gender differences in HF exacerbation may be a component explaining gender differences in longevity.
1. INTRODUCTION
The aging human population, progress in the treatment of Acute Cardiac Event and drop in related mortality stimulate the increase of admissions number and cost of treatment of heart failure patients. It’s also a rising group between death causes from heart diseases [1-10]. In recent years many studies were published demonstrating the links of a number of cardiovascular events (AMI, SCD, Cardiac Arrhythmia, Stroke) with environmental physical activity-solar (SA), Geomagnetic (GMA), Cosmic Ray (Neutron) (CRA) activity. The aim of this study was to check the timing of hospital admissions of heart failure (HF) patients and association of monthly distribution of admissions with season of the year and the mentioned space weather components.
Patients and Methods: The subject of the study was 76,601 admissions of 27,187 (14,457 male and 12,729 female) patients in two hospitals (Beilinson and Hasharon) of Rabin Medical Center in Petah Tiqwa, Israel, a tertiary medical facility, affiliated to Tel Aviv University. The admitted patients included 42,293 male and 34,308 female. The observation time was 13 years—2000- 2012, 156 months. Monthly admissions for patients with HF, including codes 428 - 0.1 of the IDC9 were included in this study. Statistical evaluation included monthly both gender admissions and the number comparison, average monthly admission numbers, maximal and minimal admissions monthly and monthly admission number correlation with SA, GMA, CRA (Neutron) activity monthly indices. The cosmophysical data were obtained from space science institutions in the USA, Russia and Finland [11-15].
For the obtained results Pearson correlation coefficients and their probabilities were calculated. Probabilities of 95% and higher were accepted as significant, these of 90% - 94.9%—as strong trend to statistical significance.
2. RESULTS
The number of admissions fluctuated by season, achieving the maximum in winter months—January, February, December, March, according to admission numbers, and minimal in late summer—August and September. The monthly admission range was 338 - 726 for all admissions; 180 - 410 for male and 171 - 326 for female patients monthly admissions. The average of HF patient’s admissions at the observation time was 2.82 times/per patient; 2.91 for male and 2.70 for female patients.
Figure 1 presents the monthly distribution of admissions for HF in Beilinson and Hasharon hospitals of Rabin Medical Center in years 2000-2012. The monthly average admission number was 491.0 ± 82.4; 271.1 ± 46.75 for male and 219.9 ± 39.8 for female patients.
Male admissions were significantly more, (p < 0.0001); according to the admissions range data monthly admissions differed by 2.0 - 2.5 times. Male/female admission ratio was 1.23. Male/Female patients’ ratio was 1.14. Both gender monthly admissions correlation coefficient was r = 0.8, p < 0.0001.
The correlation coefficients (r) and their probability (p) between monthly admissions number for HF (total and for both gender) and indices of cosmophysical activity are presented in Table 1.
3. DISCUSSION
Last decades are accompanied by significant reduction in cardiovascular mortality and raising population lifespan [3,5]. The results of treatment of many acute cardiac events made the older population more often survive with damaged heart muscle, heart valves, arteries and other structures [7,8]. HF, that was in previous years growing in between the representatives of the older population, in the XXI century progressed in most industrial countries and serve the basis for more admissions for HF. Long time survival of HF patients is worse than in many sorts of cancer, the great Heart Disease concurrent as the leading cause of human mortality [2-5]. The age related
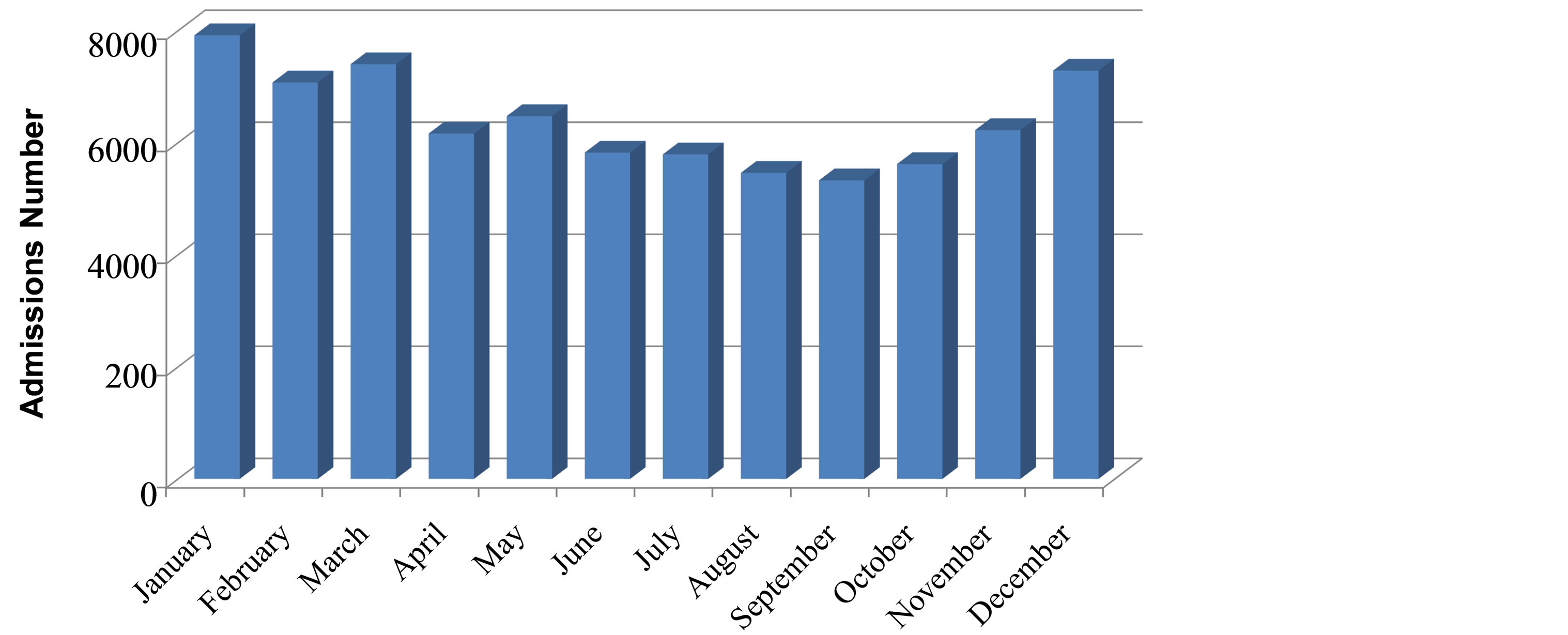
Figure 1. Monthly admissions number for heart failure (n = 76,601) Rabin Medical Center, 2000-2012.
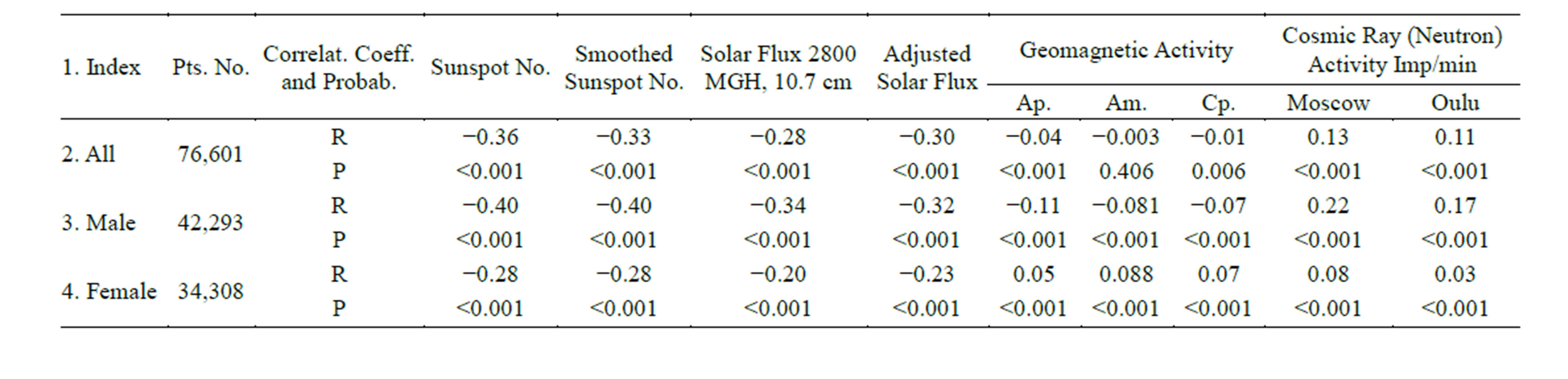
Table 1. Heart failure patients admission number monthly and space weather activity indices pearson correlation coefficients (r) and their probabilities (p).
progress in HF in the Framingham study was 8 per 1000 at age 50 - 59 for both gender, and 66 per 1000 for male and 79 for female at age 80 - 89 [5]. In a later European-Rotterdam study male patients prevailed, like in this study, and the percent of HF patients increased from 0.9% at age 55 - 64 to 17.4% in persons 85 years andolder [6]. Both American and European authors predict that in the next 7 - 10 years the percent of HF will increase by 20% - 25% [3-6]. In the latest (2013) American guidelines HF is described as affecting 20% of Americans at age ≥ 40. HF is seen in 20:1000 in the age group of 60 - 69 achieving 80:1000 at age ≥ 85 with 50% 5 years mortality after diagnosis [8-10].
The season differences of HF admissions follow the yearly rhythmicity in mortality. In our previous study it was shown that in two different countries with significant climate differences in the Northern hemisphere cardiovascular mortality is maximal in February [16]. The response of the cardiovascular system to lower temperatures, comorbidities, changes in diet, social problems are between the possible stimulators for HF exacerbation in winter months [2,3,5]. New studies confirm the positive impact of Flu vaccination on cardiovascular disease natural history [17].
Special attention was put on links between admission time (month) and associated space weather activity indices. It follows a number of publications describing such links between SA, GMA, CRA (Neutron) activity and such cardiovascular emergencies like SCD, AMI, life threatening cardiac arrhythmia’s, blood coagulation, inflammation markers, immunoglobulin levels, hormone production with the level of the mentioned cosmophysical parameters [18-58].
Between the mentioned risk factors for HF [2] coronary heart disease, cardiac arrhythmia, arterial hypertension exacerbation are significantly connected with such space weather parameters like SA, GMA, CRA (Neutron) activity [30-58].
Such pathogenesis factors like myocardial contractility (related to coronary perfusion and ischemia), arrhythmia —atrial fibrillation, different sorts of tachycardia, or heart conduction defects can serve as aggravating heart failure factors, changing the patients status and demanding hospital treatment [2].
The data presented in Table 1 confirm such connection between HF monthly admissions and studied physical indices.
Here it must be explained the interrelationship between the mentioned space physical activity factors: Cosmic ray origin is still a subject for active scientific discussion. The most energetic (mostly proton consisting) part of CRA are the highest known energies, reaching 1020-22 electronvolt. The accepted physical laws are built for energies up to 1019 electronvolt. If Cosmic Ray would be from our galaxy it would demand to add a special coefficient (Plank parameter) to most energy related formulas. This was discussed repeatedly in the last years [59-61]. But at this stage it’s accepted that Cosmic Ray comes to our galaxy from a “near”, but different galaxy, or from there located Supernova [62-64]. This allows remaining with the accepted energetic processes formulation. The SA and GMA are natural shields of our Planet from the super energetic parts of Cosmic Ray [59-64]. In our previous publications it was shown that in the last 10 - 20 years SA was inverse correlated with CRA by r = −0.85, p < 0.0001 and positive related to GMA, r = 0.50, p < 0.0001. GMA is also inverse related to CRA, r = −0.66, p < 0.0001. This explains the negative correlation of SA with HF admissions seen in Table 1, and positive with CRA. CRA is measured by Neutron activity (imp/min) on the Earth surface. Why Neutron? The high energy Cosmic Rays are so energetic, that many atom electrons in the surrounding space are compressed into the nuclei of the atoms and converted to Neutrons. The number of these remains of atoms arriving to the Earth’s surface is the measure of Cosmic Rayactivity [59]. Despite the multiple etiology of HF exacerbation, were the medical side is only one of many “players” in the change in the natural history, we see that the changes in this part of the process follows the time distribution of such medical events like AMI, SCD, Stroke by their connection with physical parameters of the space weather [11,15,21,46,47]. In an additional study related to circannual death distribution it was shown that this process is rhythmic and the acrophase for total deaths number, cardiac origin and stroke related deaths are in February, with small time differences by gender and each of the mentioned etiologies [16,17,21]. The male prevalence in HF admissions can be a component of causes related to higher, female longevity in most countries [65].
The relatively low, but very significant correlation coefficients in Table 1 are a consequence of number of factors: antagonistic action of the space activity factorsSA and GMA are inverse correlated to CRA and serve as a shield of our Planet from CRA. SA is at r = −0.85 related to CRA; GMA at r = −0.66 [11,46,47,57,58]. HF is provoked by many, often very different, factors that are different related with environment influences; GMA and CRA are more connected with daily than in monthly fluctuations in biological effects [11,15,21].
4. CONCLUSIONS
Monthly admissions number for HF is fluctuated by season of the year, depending on gender and related to monthly solar, Geomagnetic and Cosmic Ray (Neutron) activity level.
Gender differences in HF exacerbation can be a component explaining longevity differences in male and female longevity in most industrialized countries.
REFERENCES
- Brook, R.D., Franklin, B., Cascio, W., Hong, Y., Howard, G., Lipsett, M., Lueker, R., Mittleman, M., Samet, J., Smith Jr., S.C. and Tager, I. (2004) AHA scientific statement: Air pollution and cardiovascular disease. Circulation, 109, 2655-2659. http://dx.doi.org/10.1161/01.CIR.0000128587.30041.C8
- Cowie, M. (2013) Essentials of heart failure. Wiley, Blackwell, 115 p.
- McMurray, J.J., Adamopoulos, S., Anker, S.D., et al. (2012) ESC committee for practice guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 33, 1787-1847.
- Liao, L., Allen, L.A. and Whellan, D.J. (2008) Economic burden of heart failure in the elderly. Pharmacoeconomics, 26, 447-462. http://dx.doi.org/10.2165/00019053-200826060-00001
- Ho, K.K., Pinsky, J.L., Kannel, W.B. and Levy, D. (2004) The epidemiology of heart failure: The Framingham study. Journal of the American College of Cardiology, 22, 6- 13A. http://dx.doi.org/10.1016/0735-1097(93)90455-A
- Bleumink, G.S., Knetsch, A.M., Sturkenboom, et al. (2004) Quantifying the heart failure epidemic: Prevalence, incidence rate, lifetime risk and prognosis of heart failure. The Rotterdam Study. European Heart Journal, 25, 1614- 1619. http://dx.doi.org/10.1016/j.ehj.2004.06.038
- Mosterd, A., Hoes, A.W., Brayne, D.E., et al. (1999) Prevalence of heart failure and left ventricular dysfunction in the general population. The Rotterdam study. European Heart Journal, 20, 447-455. http://dx.doi.org/10.1053/euhj.1998.1239
- Stewart, S., MacIntyre, K., Capewell, S. and McMurray, J.J. (2003) Heart failure in the aging population: An increasing burden in the 21st century? Heart, 89, 49-53. http://dx.doi.org/10.1136/heart.89.1.49
- McMurray, J.J. and Pheffer, M.A. (2005) Heart failure. Lancet, 365, 1877-1889. http://dx.doi.org/10.1016/S0140-6736(05)66621-4
- Yancy, C.W., Jesup, M., Bozkurt, B., Butler, J., et al. (2013) 2013 ACCF/AHA guideline for the management of heart failure: A report of the american college of cardiology foundation/american heart association task force on practice guidelines. Circulation, 128, 1810-1852. http://dx.doi.org/10.1161/CIR.0b013e31829e8807
- Stoupel, E. (2012) Space weather and timing of cardiovascular events (Clinical Cosmibiology). Lambert Academic Publishing, 72 p.
- Stupelis, I. (1971) Prognosis in cardiology. Mintis Press, Vilnius, 162.
- Stoupel, E. (1980) Solar-terrestrial prediction: Aspects for preventive medicine. In: Donnelly, R.F., Ed., Solar-Terrestrial Predictions Proceedings, NOAA, Space Environment Laboratory, Boulder, G29-G40.
- Stoupel, E. (1976) Forecasting in Cardiology. John Wiley & Sons, New York, 141.
- Stoupel, E. (2013) Space weather and medical events: Medical observation for 45 years (Clinical Cosmobiology). In: Space Weather Effects on Humans in Space and on Earth. Proceedings of International Conference (Vol. 2), Space Research Institute, Russian Academy of Sciences, Moscow, 551-559.
- Stoupel, E., Petrauskiene, J., Gabbay, U., Kalediene, R., Abramson, E. and Sulkes, J. (2001) Circannual rhythmicity of deaths distribution. Acta Medica Lituanica, 6, 37- 42.
- Nichol, K.L., Kristin, L. Nichol, M.D., Nordin, J., Mullooly, J., Richard, J., Lask, R., Fillbrandt, K. and Iwane, M. (2003) Influenza vaccination and reduction in hospitalizations for cardiac disease and stroke among the Elderly. 1322-1332.
- Chizhevski, A.L. (1976) Terreastrial echos of solar storms. 2nd Edition, Misl’ Press, Moscow, 419.
- Barnothy, M.F. (1964) Biological effects of magnetic fields. Plenum Press, New York.
- Rozhdestvenskaya, E. and Novikova, K. (1969) Influence of solar activity on the blood fibrinolytic system. Klin Med (Moscow), 47, 65-69.
- Oranevski, V.N., Breus, T.K., Baevski, R.M., Rapoport, S.I., Petrov, V.M. and Barsukova, ZhV. (1998) Effect of geomagnetic activity on the functional status of the body. Biofizika, 43, 819-826.
- Stoupel, E., Kalediene, R., Petrauskiene, J., Starkuviene, S., Abramson, E., Israelevich, P. and Sulkes, J. (2011) Twenty years study of solar, geomagnetic, cosmic ray activity links with monthly deaths number (n-850304). Journal of Biomedical Science & Engineering, 4, 1-9
- Stoupel, E., Abramson, E., Domarkiene, S., Shimshoni, M. and Sulkes, J. (1997) Space proton flux and the temporal distribution of cardiovascular deaths. International Journal of Biometeorology, 40, 113-116. http://dx.doi.org/10.1007/s004840050029
- Stoupel, E., Israelevich, P., Gabbay, U., Abramson, E., Petrauskiene, J., Kalediene, R., Domarkiene, S. and Sulkes, J. (2000) Correlation of two levels of space proton flux with monthly distribution of deaths from cardiovascular disease and suicide. Journal of Basic and Clinical Physiology and Pharmacology, 1, 63-71.
- Stoupel, E. (2002) Effect of geomagnetic activity on cardiovascular parameters. Biomedicine & Pharmacother, 56, 246s-256s. http://dx.doi.org/10.1016/S0753-3322(02)00299-8
- Stoupel, E. (1980) Solar-terrestrial prediction: Aspects for preventive medicine. In: Donnelly, R.F., Ed., Solar-Terrestrial Predictions Proceedings (Vol. 4), Space Environment Laboratory, US NOAA, Boulder, G29-G 40.
- Stoupel, E. (1976) Forecasting in cardiology. John Wiley & Sons, New York, 141.
- Stoupel, E. (2012) Space weather and timing of cardiovascular events (Clinical Cosmobiology). Lambert Academic Publishing, 72 p.
- Stoupel, E. (2013) Space weather and medical events: medical observation for 45 years (Clinical Cosmobiology). In: Space Weather Effects on Humans in Space and on Earth. Proceedings of International Conference (Vol. 2), Space Research Institute, Russian Academy of Sciences, Moscow, 551-559.
- Stoupel, E., Israelevich, P., Petrauskiene, J., Kalediene, R., Abramson, E. and Sulkes, J. (2002) Cosmic ray activity and monthly number of deaths: A correlative study. Journal of Basic and Clinical Physiology and Pharmacology, 13, 23-32. http://dx.doi.org/10.1515/JBCPP.2002.13.1.23
- Stoupel, E., Joshua, H. and Lahav, J. (1996) Human blood coagulation parameters and geomagnetic activity. European Journal of Internal Medicine, 7, 217-220.
- Stoupel, E., Abramson, E., Israelevich, P., Sulkes, J. and Harell, D. (2007) Dynamics of serum C-reactive protein (CRP) and cosmophysical activity. European Journal of Internal Medicine, 18, 124-128. http://dx.doi.org/10.1016/j.ejim.2006.09.010
- Stoupel, E., Abramson, E., Gabbay, U. and Pick, A.I. (1995) Relationship between immunoglobulin levels andextremes of solar activity. International Journal of Biometeorology, 38, 89-91. http://dx.doi.org/10.1007/BF01270665
- Stoupel, E., Monselize, Y. and Lahav, J. (2006) Changes in autoimmune markers of the anti cardiolipin syndrome on days of extreme geomagnetic activity. Journal of Basic and Clinical Physiology and Pharmacology, 17, 269- 278. http://dx.doi.org/10.1515/JBCPP.2006.17.4.269
- Stoupel, E., Keret, R., Assa, S., Kaufman, H., Shimshoni, M. and Laron, Z. (1983) Secretion of growth hormone, prolactin and corticosteroids during different levels of geomagnetic activity. Neuroendocrinology Letters, 5, 365-358.
- Stoupel, E., Keret, R., Gil-Ad, I., Assa, S., Silbergeld, A., Shimshoni, M. and Laron, Z. (1980) Secretion of growth hormone and prolactin in extreme periods of solar activity in solar cycle 21 (1976-1986). Neuroendocrinology Letters, 5, 191-295.
- Stoupel, E., Zabludovsky, M., Wittenberg, C. and Boner, G. (1998) Ambulatory blood pressure monitoring in patients with hypertension on days of high and low geomagnetic activity. International Journal of Hypertension, 39, 293-294.
- Stoupel, E., Petrauskiene, J., Kalediene, R., Domarkiene, S., Abramson, E. and Sulkes, J. (1996) Distribution of deaths from ischemic heart disease and stroke: Environmental and aging influences in men and woman. Journal of Basic and Clinical Physiology and Pharmacolog, 7, 303-320. http://dx.doi.org/10.1515/JBCPP.1996.7.4.303
- Stoupel, E., Martfel, J. and Rotenberg, Z. (1994) Paroxysmal atrial fibrillation and stroke in male and female above and below age 65 on days of different geomagnetic activity levels. Journal of Basic and Clinical Physiology and Pharmacology, 5, 315-329.
- Stoupel, E., Assali, A., Teplitzky, I., Israelevich, P., Abramson, E., Sulkes, J. and Kornowski, R. (2008) The culprit artery in acute myocardial infarction in different environmental physical activity levels. International Journal of Cardiology, 126, 288-290. http://dx.doi.org/10.1016/j.ijcard.2007.05.050
- Stoupel, E., Abramson, E. and Israelevich, P. (2011) Left anterior descending/right coronary arteries as culprit arteries in acute myocardial infarction (n-2011) in changing physical environment, percutaneous coronary intervention data (2000-2010). Journal of Basic and Clinical Physiology and Pharmacolog, 22, 91-95. http://dx.doi.org/10.1515/JBCPP.2011.024
- Stoupel, E., Zhemaityte, D., Drungeliene, D., Martinkenas, A., Abramson, E. and Sulkes, J. (2002) Klaipeda emergency cardiovascular services: Links with 10 cosmophysical parameters. Journal of Clinical and Basic Cardiology, 5, 225-227.
- Stoupel, E., Israelevich, P., Petrauskiene, J., Kalediene, R., Abramson, E. and Sulkes, J. (2002) Cosmic ray activity and monthly number of deaths: A correlative study. Journal of Basic and Clinical Physiology and Pharmacolog, 13, 23-32. http://dx.doi.org/10.1515/JBCPP.2002.13.1.23
- Stoupel, E., Kalediene, R., Petrauskiene, J., Domarkiene, S., Radishauskas, R., Abramson, E., Israelevich, P. and Sulkes, J. (2004) Three kinds of cosmophysical activity: Links to temporal distribution of deaths and occurrence of acute myocardial infarction. Medical Science Monitor, 10, CR80-CR84.
- Stoupel, E., Babayev, E., Mustafa, F., Abramson, E., Israelevich, P. and Sulkes, J. (2007) Acute myocardial infarction occurrence: Environmental links-Baku 2003-2005 data. Medical Science Monitor, 13, BR175-BR179.
- Stoupel, E., Tamoshiunas, A., Radishauskas, R., Bagdoniene, G., Abramson, E., Sulkes, J. and Israelevich, P. (2010) Acute myocardial infarction (AMI) and intermediate coronary syndrome (ICS). Health, 2, 131-136. http://dx.doi.org/10.4236/health.2010.22020
- Stoupel, E., Tamoshiunas, A., Radishauskas, R., Benotiene, G., Abramson, E. and Israelevich, P. (2011) Neutrons and the plaque: AMI (n-8920) at days of zero GMA/high neutron activity (n-36) and the following days and week. Kaunas, Lithuania, 2000-2007. Clinical & Experimental Cardiology, 2, 121-125.
- Stoupel, E., Domarkiene, S., Radishauskas, R., Bernotiene, G., Abramson, E. and Israelevich, S.J. (2004) Links between monthly rates of four types of acute myocardial infarction and their corresponding cosmophysical activity parameters. Journal of Basic and Clinical Physiology and Pharmacolog, 14, 175-184.
- Stoupel, E., Tamoshiunas, A., Domarkiene, S., Radishauskas, R., Bernotiene, G. and Abramson, E. (2008) Dynamics of in-hospital cardiac arrhythmia in patients with acute myocardial infarction. Journal of Interventional Cardiac Electrophysiology, 21, 183.
- Stoupel, E. (1993) Sudden cardiac deaths and ventricular extrasystoles on days with four levels of geomagnetic activity. Journal of Basic and Clinical Physiology and Pharmacolog, 4, 357-366. http://dx.doi.org/10.1515/JBCPP.1993.4.4.357
- Stoupel, E., Domarkiene, S., Radishauskas, R., Abramson, E. and Sulkes, J. (2011) Sudden cardiac death and geomagnetic activity: Links to age, gender and agony time. Journal of Basic and Clinical Physiology and Pharmacolog, 13, 11-22. http://dx.doi.org/10.1515/JBCPP.2002.13.1.11
- Stoupel, E., Domarkiene, S., Radishauskas, R. and Abramson, E. (2002) Bastille day event and sudden cardiac death. Seminars in Cardiology, 8, 18-21.
- Stoupel, E., Babayev, E.S., Mustafa, F.R., Abramson, E., Israelevich, P. and Sulkes, J. (2006) Clinical cosmobiology—Sudden cardiac death and daily/monthly geomagnetic, cosmic ray and solar activity—The Baku study (2003-2005). Sun & Geosphere, 1, 13-16.
- Stoupel, E., Domarkiene, S., Radishauskas, R., Abramson, E., Israelevich, P. and Sulkes, J. (2006) Neutrons and sudden cardiac death (SCD)-codes 121-125 ICD 10. Journal of Basic and Clinical Physiology and Pharmacology, 17, 46-54. http://dx.doi.org/10.1515/JBCPP.2006.17.1.45
- Stoupel, E., Israelevich, P., Kusniec, J., Mazur, A., Zabarski, R., Golovchiner, G., Abramson, E. and Strasberg, B. (2006) Battler are neutrons involved in the pathogenesis of life-threatening cardiac arryhthmias? Journal of Basic and Clinical Physiology and Pharmacology, 17, 55-62. http://dx.doi.org/10.1515/JBCPP.2006.17.1.55
- Stoupel, E., Kusniec, J., Mazur, A., Abramson, E., Israelevich, P. and Strasberg, B. (2008) Timing of life-threatening arrhythmias detected by implantable cardioverter-defibrillators in relation to changes in cosmophysical factors. Cardiology Journal, 15, 437-440.
- Stoupel, E. (2002) The equilibrium paradigm in clinical cosmobiology. Journal of Basic and Clinical Physiology and Pharmacology, 13, 255-261.
- Stoupel, E. (2008) Atherothrombosis: Environmental links. Journal of Basic and Clinical Physiology and Pharmacology, 19, 37-47.
- Sigl, G. (2001) Ultra-high—Energy cosmic rays: Physics and astrophysics at extreme energies. Science, 291, 73-79.
- [61] Amelino-Camelia, G. (2002) Relativity: Special treatment. Nature, 418, 34-35.
- [62] Aharonian, F., Akhperanian, A.G., Bazer-Bachi, A.R., Belicke, M., Benbow, W., Berniohr, K., Boisson, C., et al. (2006) Discover of veryhigh-energy gamma rays from the lactic centre ridge. Nature, 439, 695-698. http://dx.doi.org/10.1038/nature04467
- [63] The Pierre Auger Collaboration (2007) Correlation of the highest-energy cosmic rays with nearby extragalactic objects. Science, 318, 938-943. http://dx.doi.org/10.1126/science.1151124
- [64] Johnston, H. (2008) Cosmic-ray mystery solved at last. 31764, 1-3. http://physicsworld.com/cws/article/news/
- [65] Cho, A. (2007) Universe’s highest-energy particles traced back to other galaxies. Science, 318, 896-897. www.sciencemag.org
- [66] Regan, J.C. and Partridge, L. (2013) Gender and longevity: Why do men die earlier than woman? Comparative and experimental evidence. Best Practice & Research Clinical Endocrinology & Metabolism, 27, 467-479. http://dx.doi.org/10.1016/j.beem.2013.05.016