Open Journal of Stomatology
Vol.2 No.4(2012), Article ID:25733,4 pages DOI:10.4236/ojst.2012.24063
Bilateral double teeth—A case report
![]()
Department of Oral Pathology, Terna Dental College, Mumbai, India
Email: sandyopath@rediffmail.com
Received 10 August 2012; revised 12 September 2012; accepted 18 September 2012
Keywords: Developmental Anomaly; Fusion; Gemination; Endodontic Treatment
ABSTRACT
Developmental anomalies can occur as a result of conjoining or twinning defects. These include fusion, gemination and concrescence. Such anomalies occur more often in the deciduous than in the permanent dentition and only a few cases involving molar and premolar teeth have been reported in the literature. Cases of bilateral double teeth are less frequent than unilateral and prevalence seems to be higher in the anterior region. The present article is a rare case report of simultaneous occurrence of double teeth in permanent dentition involving the mandibular premolar-molar teeth in a 45-year-old male patient. Clinical observation along with radiographic examination was used to arrive at a diagnosis.
1. INTRODUCTION
The terms “double tooth”, “joined teeth”, or “connoted teeth” are often used to describe fusion and gemination, both of which are primary developmental abnormalities of the teeth [1]. Fusion of teeth refers to the union of two normally separated tooth germs, and depending upon the stage of development of the teeth at the time of union, it may be either complete or incomplete [2]. Whereas, in geminated teeth, division is usually incomplete and results in a large tooth crown that has a single root and a single canal [3]. Fusion can occur between teeth of the same dentition or mixed dentitions, and between normal and supernumerary teeth [4,5]. In these cases, the number of teeth in the dental arch is also normal and differentiation from gemination is clinically difficult or impossible.
Such anatomic irregularities occur more often in the deciduous than in the permanent dentition [6]. Only a few cases of fusion involving molar and premolar teeth have been reported [6] whereas, in both dentitions, the prevalence is higher in the anterior region [4,5]. Turell and Zmener [7] have described a case of fusion involving a mandibular third molar and fourth molar (distomolar). Cases of bilateral fusion are less frequent [6] further concurrent occurrence of fusion and gemination is rarely reported in the literature.
In clinical situations, cases of conjoined teeth pose a diagnostic challenge owing to the presence of superimposed anomalies. This is especially true in cases of union between a normal tooth bud to a supernumerary tooth germ or in cases of complete fusion and the contiguous “normal” tooth being congenitally absent, resembling clinical cases of germination [8,9]. This paper reports a rare case of simultaneous occurrence of gemination and fusion involving mandibular posterior quadrants, in which one was successfully treated with nonsurgical endodontic therapy and the other required no treatment.
2. CASE REPORT
A 45-year-old male patient reported to the department with a chief complaint of decay and food lodgment in the lower left back teeth. The tooth was associated with occasional pain and abnormal sensitivity to hot and cold. His medical and dental histories were unremarkable. No other member of the family was affected with similar dental anomalies. Clinical examination revealed bilateral presence of unusually large teeth in the mandibular premolar-molar region. There appeared to be a fusion between 35 and 36 with deep occlusal caries involving the line of fusion between the two teeth (Figure 1). Also, 45 exhibited an abnormally large crown but was caries-free (Figure 2).
Radiographic evaluation of the right side revealed geminated 45 with a single root and root canal (Figure 3). On the left side, fusion between 35 and 36 was seen resulting in a single large pulp chamber, two roots and two root canals (Figure 4). 35 was missing, suggesting, it is a case of fusion and not gemination.
Patient was prescribed analgesics and antibiotic course. Treatment plan was aimed at preserving 36 through endodontic treatment and restoration. Since 45 was asymptomatic and caries free, patient was encouraged to practice strict oral hygiene and maintain periodic follow ups. On post two week recall examination, the patient was

Figure 1. Fusion between 35 and 36 with deep occlusal caries.

Figure 2. 45 with abnormally large crown.
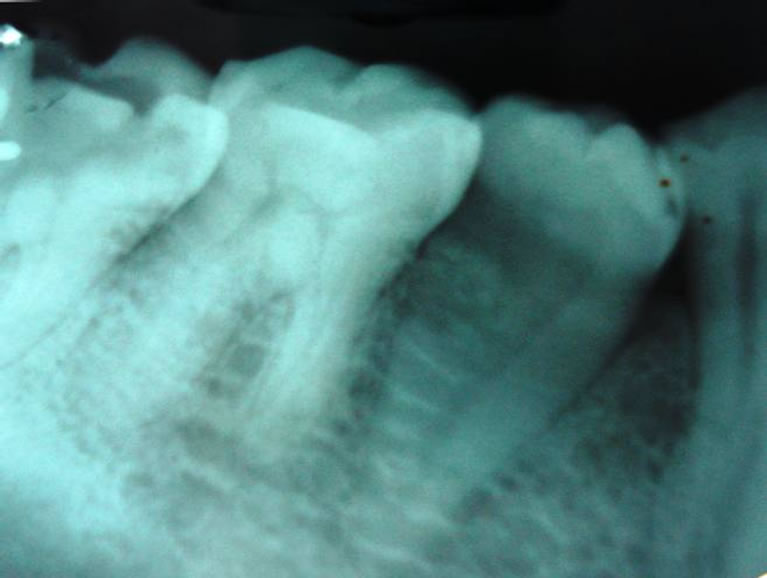
Figure 3. Geminated 45 with a single root and root canal.
asymptomatic. The case was diagnosed to be a rare incidence of bilateral double teeth, with gemination of 45

Figure 4. Fusion between 35 and 36, resulting in a single large pulp chamber, two roots and two root canals.
and fusion between 35 and 36.
3. DISCUSSION
The terminology dental fusion and gemination are used to define two different morphological dental anomalies, characterized by the formation of a clinically wide tooth. Despite the considerable number of cases reported in the literature, the differential diagnosis between these abnormalities is difficult [8]. Case history and clinical and radiographic examinations can provide the information required for the diagnosis of such abnormalities [8,10].
Fused teeth arise through union of two normally separated tooth germs, and depending upon the stage of development of the teeth at the time of union, it may be either complete or incomplete. It has been thought that some physical force or pressure produces contact between developing teeth resulting in their subsequent fusion. On some occasions, two independent pulp chambers and root canals can be seen. It can occur between normal teeth or between normal and supernumerary teeth. In gemination, division is usually incomplete and results in a large tooth crown that has a single root and a single canal [3]. While the literature on the occurrence of double teeth is extensive, there is still much discussion concerning the nomenclature. The use of Levitas’ classification to distinguish between cases of fusion and gemination seems to be very practical [11]. In clinical situations, cases of fusion have the appearance of a congenitally missing tooth, while in gemination the number of teeth in the dentition is normal, provided the double tooth is counted as one unit [8].
The differential diagnosis between fusion and gemination, based on the number of teeth present on the dental arch, is not, however, always accurate [3]. Since fusion can also be the union of a normal tooth bud to a supernumerary tooth germ, the number of teeth is also normal and differentiation from gemination may be very difficult, if not impossible. Finally, some authors simply call the phenomenon “double teeth” or “connoted teeth” to avoid confusion over their terminologies [8]. After a judicious evaluation of all information, we can report this case as a rare presentation of gemination and fusion occurring simultaneously, in mandibular posterior region.
Teeth with such abnormalities are unaesthetic due to their irregular morphology. They also present a high predisposition to caries, periodontal diseases, and spacing/ crowding problems. The periodontal complications occur due to the presence of fissures or grooves in the union between the teeth involved. If these defects are very deep and extend subgingivally, the possibility of bacterial plaque accumulation in this area is quite high. Strict oral hygiene is imperative to maintain periodontal health. Furthermore, fusion may have an adverse effect on occlusion, causing deviation and sometimes delayed eruption of other teeth. In this case, irregular morphology of 36 with deep fissures may be the reason for caries susceptibility with subsequent pulpal involvement.
Several treatment methods have been described in the literature with respect to the different types and morphological variations of fused teeth, which include endodontic, restorative, surgical, periodontal and/or orthodontic treatment [7]. However routine endodontic therapy remains the treatment of choice in cases with periapical involvement, as being planned in our case.
In some instances, one of the first procedures of endodontic therapy, rubber dam isolation, may be complicated due to the anatomical size and shape of the crown. Locating canals during access preparation can be difficult. Mesial and/or distal radiographic projections can give more information about morphological features and the relationship between the canals, making the interpretation of structures easier [11]. A multidisciplinary approach with different practitioners working together can contribute to the success of a treatment plan.
4. CONCLUSION
Fused teeth contribute to esthetic concerns, space problems, occlusal disturbances, and delayed eruption of the permanent successors. Also, they raise concerns about periapical pathologies, as was the situation occurring with this reported case. Hence, careful monitoring of the condition is recommended. Meticulous history taking, clinical and radiographic examinations can provide vital information required for the diagnosis of such abnormalities. Long term follow up of treated case is mandatory. Also, we encourage dental practitioners to consider this conservative approach before more complex or radical treatment alternatives are attempted.
REFERENCES
- Pereira, A.J., Fidel, R.A. and Fidel, S.R. (2000) Maxillary lateral incisor with two root canals: Fusion, gemination or dens invaginatus. Brazilian Dental Journal, 11, 141-146.
- Chalakkal, P. and Thomas, A.M. (2009) Bilateral fusion of mandibular primary teeth. Journal of Indian Society of Pedodontics and Preventive Dentistry, 27, 108-110. doi:10.4103/0970-4388.55336
- O’Reilly, P.M.R. (1990) Structural and radiographic evaluation of four cases of tooth fusion. Australian Dental Journal, 35, 226-229. doi:10.1111/j.1834-7819.1990.tb05398.x
- Hülsmann, M., Bahr, R. and Grohmann, U. (1997) Hemisection and vital treatment of a fused tooth—Literature review and case report. Dental Traumatology, 13, 253-258. doi:10.1111/j.1600-9657.1997.tb00051.x
- De Velasco, L.F., Araujo, F.B., Ferreira, E.S. and Velasco, L.E. (1997) Esthetic and functional treatment of a fused permanent tooth: A case report. Quintessence International, 28, 677-680.
- Nunes, E., Moraes, I.G., Novaes, P.M.O. and Sousa, S.M.G. (2002) Bilateral fusion of mandibular second molars with supernumerary teeth: Case report. Brazilian Dental Journal, 13, 137-141.
- Braz Turell, I.L. and Zmener, O. (1999) Endodontic therapy in a fused mandibular molar. Journal of Endodontics, 25, 208-209.
- Türkaslan, S., Gökçe, H.S. and Dalkız, M. (2007) Esthetic rehabilitation of bilateral geminated teeth: A case report. European Journal of Dentistry, 1, 188-191.
- Terezhalmy, G.T. and Riley, C.K. (1999) Gemination/ fusion. Quintessence International, 30, 437.
- Milano, M., Seybold, S.V., McCandless, G. and Cammarata, R. (1999) Bilateral fusion of the mandibular primary incisors: Report of case. ASDC Journal of Dentistry for Children, 66, 280-282.
- Neves, A.A., Neves, M.L.A. and Farinhas, J.A. (2002) Bilateral connation of permanent mandibular incisors: A case report. International Journal of Paediatric Dentistry, 12, 61-65. doi:10.1046/j.0960-7439.2001.00324.x