Late-onset Orbital Cellulitis with Abscess Formation Caused by Klebsiella Pneumoniae 91
procedures may all expose the orbit to infection [34,35].
Therefore, patients undergoing any interventional proce-
dures should be closely monitored for signs of infection
and should be treated aggressively if evidence of an in-
fection is found [24].
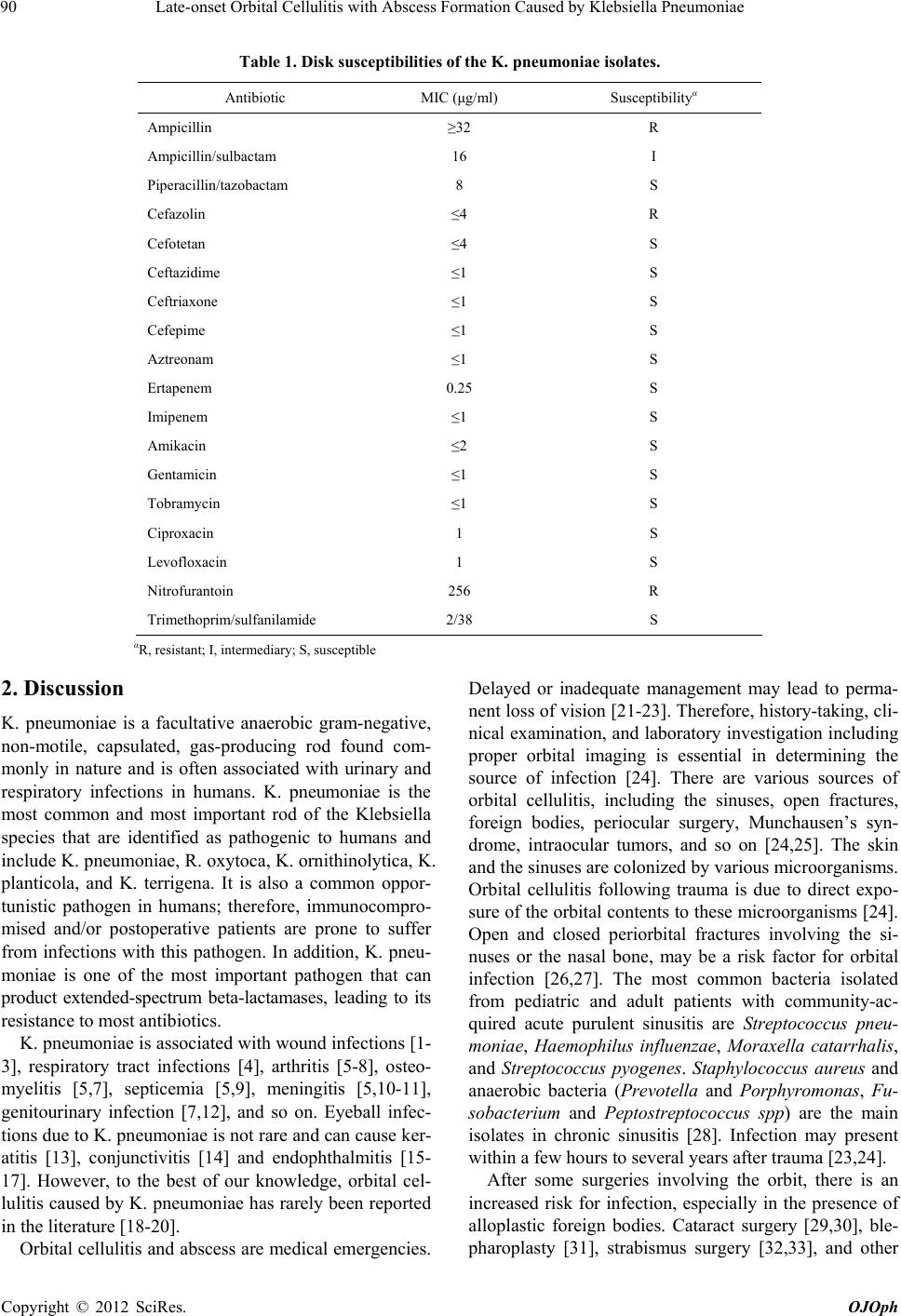
Because K. pneumoniae is almost extended-spectrum
β-lactamase-producing bacillus, it is resistant to most anti-
biotics. Susceptibility testing is necessary to help physi-
cians choose the appropriate antibiotics in clinic. In our
case, the results of the susceptibility testing showed that
piperacillin/tazobactam, cefazolin, cefotetan, ceftazidime,
ceftriaxone, cefepime, aztreonam, ertapenem, imipenem,
amikacin, gentamicin, tobramycin, ciproxacin, levoflox-
acin are all effective. However, the extended-spectrum
β-lactamase-producing bacteria, which show susceptible
to penicillins, cephalosporins and aztreonam often be-
come resistant to them. Therefore, β-lactamase inhibitors
and carbapenems are recommended in clinical practice.
Our patient was treated with intravenous piperacillin/
tazobactam for 7 days and oral imipenem for 14 days
after surgery without recurrence for 6 months.
3. Conclusion
To our knowledge, this is the first case of late-onset or-
bital cellulitis and abscess formation induced by K. pneu-
moniae after an orbital wall fracture prosthesis with hy-
droxyapatite implantation reported in the literature. Or-
bital cellulitis and abscess formation due to K. pneumo-
niae should be considered, whenever patients suffer the
orbital trauma and undergo surgery.
REFERENCES
[1] E. Rezaei, H. Safari, M. Naderinasab, et al., “Common
Pathogens in Burn Wound and Changes in Their Drug
Sensitivity,” Burns, Vol. 37, No. 5, 2011, pp. 804-806.
doi:10.1016/j.burns.2011.01.019
[2] M. I. Ahmed, “Prevalence of Nosocomial Wound Infec-
tion among Postoperative Patients and Antibiotics Pat-
terns at Teaching Hospital in Sudan,” North American
Journal of Medical Sciences, Vol. 4, No. 1, 2012, pp. 29-
34. doi:10.4103/1947-2714.92900
[3] A. K. Seth, M. R. Geringer, A. N. Gurjala, et al., “Under-
standing the Host Inflammatory Response to Wound In-
fection: An in Vivo Study of Klebsiella Pneumoniae in a
Rabbit Ear Wound Model,” Wound Repair and Regen-
eration, Vol. 20, No. 2, 2012, pp. 214-225.
doi:10.1111/j.1524-475X.2012.00764.x
[4] S. Ghafourian, Z. B. Sekawi, N. Sadeghifard, et al., “The
prevalence of ESBLs Producing Klebsiella Pneumoniae
Isolates in Some Major Hospitals, Iran,” Open Microbi-
ology Journal, Vol. 5, 2011, pp. 91-95.
doi:10.2174/1874285801105010091
[5] Z. Ghorashi, N. Nezami, H. Hoseinpour-Feizi, et al.,
“Arthritis, Osteomyelitis, Septicemia and Meningitis Cau-
sed by Klebsiella in a Low-Birth-Weight Newborn: A Ca-
se Report,” Journal of Medical Case Reports, Vol. 5,
2011, p. 241. doi:10.1186/1752-1947-5-241
[6] S. Schelenz, K. Bramham and D. Goldsmith, “Septic Ar-
thritis Due to Extended Spectrum Beta Lactamase Pro-
ducing Klebsiella Pneumoniae,” Joint Bone Spine, Vol.
74, No. 3, 2007, pp. 275-278.
doi:10.1016/j.jbspin.2006.08.007
[7] L. C. Chew, “Septic Monoarthritis and Osteomyelitis in
an Elderly Man Following Klebsiella Pneumoniae Geni-
tourinary Infection: Case Report,” Annals of the Academy
of Medicine Singapore, Vol. 35, No. 2, 2006, pp. 100-
103.
[8] J. E. Kohler, M. P. Hutchens, P. M. Sadow, et al., “Kleb-
siella Pneumoniae Necrotizing Fasciitis and Septic Ar-
thritis: An Appearance in the Western Hemisphere,” Sur-
gical Infections, Vol. 8, No. 2, 2007, pp. 227-232.
doi:10.1089/sur.2006.007
[9] N. Y. Lee, W. H. Huang, K. C. Tsui, et al., “Carbapenem
Therapy for Bacteremia Due to Extended-Spectrum (Be-
ta)-Lactamase-Producing Escherichia Coli or Klebsiella
Pneumoniae,” Diagnostic Microbiology and Infectious
Disease, Vol. 70, No. 1, 2011, pp. 150-153.
doi:10.1016/j.diagmicrobio.2010.12.008
[10] A. Stucki, M. Cottagnoud, F. Acosta, et al., “Efficacy of
Doripenem against Escherichia Coli and Klebsiella Pneu-
moniae in Experimental Meningitis,” Journal of Antim-
icrobial Chemotherapy, Vol. 67, No. 3, 2012, pp. 661-
665. doi:10.1093/jac/dkr482
[11] W. N. Chang, C. H. Lu, C. R. Huang, et al., “Clinical
Characteristics of Post-Neurosurgical Klebsiella Pneu-
moniae Meningitis in Adults and a Clinical Comparison
to the Spontaneous Form in a Taiwanese Population,”
Journal of Clinical Neuroscience, Vol. 17, No. 3, 2010,
pp. 334-338. doi:10.1016/j.jocn.2009.06.019
[12] D. A. Rosen, J. S. Pinkner, J. N. Walker, et al., “Molecu-
lar Variations in Klebsiella Pneumoniae and Escherichia
coli FimH Affect Function and Pathogenesis in the Uri-
nary Tract,” Infection and Immunity, Vol. 76, No. 7, 2008,
pp. 3346-3356. doi:10.1128/IAI.00340-08
[13] S. Zarei-Ghanavati, M. R. Sedaghat and A. Ghavami-
Shahri, “Acute Klebsiella Pneumoniae Interface Keratitis
after Deep Anterior Lamellar Keratoplasty,” Japanese
Journal of Ophthalmology, Vol. 55, No. 1, 2011, pp. 74-
76. doi:10.1007/s10384-010-0836-7
[14] T. Aung and T. K. Chan, “Nosocomial Klebsiella Pneu-
moniae Conjunctivitis Resulting in Infectious Keratitis
and Bilateral Corneal Perforation,” Cornea, Vol. 17, No.
5, 1998, pp. 558-561.
doi:10.1097/00003226-199809000-00015
[15] A. H. Kashani and D. Eliott, “Bilateral Klebsiella Pneu-
moniae (K1 Serotype) Endogenous Endophthalmitis as
the Presenting Sign of Disseminated Infection,” Ophthal-
mic Surgery, Lasers & Imaging, Vol. 42, 2011, pp. e12-
e14.
[16] L. P. Ang, H. M. Lee, K. G. Au Eong, et al., “Endoge-
nous Klebsiella Endophthalmitis,” Eye, Vol. 14, No. 6,
2000, pp. 855-860. doi:10.1038/eye.2000.236
[17] Y. J. Chen, H. K. Kuo, P. C. Wu, et al., “A 10-Year Com-
parison of Endogenous Endophthalmitis Outcomes: An
Copyright © 2012 SciRes. OJOph