Paper Menu >>
Journal Menu >>
 Creative Education, 2010, 1, 51-57 doi:10.4236/ce.2010.11008 Published Online June 2010 (http://www.SciRP.org/journal/ce) Copyright © 2010 SciRes. CE 51 Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of Using Animated and DVD Formats for Nurse Instruction Ivan Beale1, Vivien Lane2 1School of Psychology, University of New South Wales, Sydney, Australia; 2Information Technology, University of Sydney, Sydney, Australia. Email: ibeale@bigpond.com, Vivien@it.usyd.edu.au Received December 21st, 2009; revised April 20th, 2010; accepted May 20th, 2010. ABSTRACT This study explored the perceptions of oncology nurses about the usefulness of a video-game or an animated DVD in- tervention designed to teach young patients about self care. The study also measured the effects of these interventions on nurses’ cancer knowledge and perceived self-efficacy to communicate with patients about self-care. Twenty-two on- cology nurses were randomly assigned either to use a video game “Re-Mission” or to view instructional animations from the game on DVD. They completed tests and rating scales before and after, then rated the acceptability of the game or DVD. Only ten participants completed the study. For these ten, ratings of the acceptability and credibility of the game or DVD were moderately positive, regardless of age or nursing experience. Self-efficacy for communicating to patients about self-care increased following use of the game or DVD. Cancer knowledge was not affected. It was con- cluded that oncology nurses in Australia are not generally enthusiastic about the concept of instruction via video game and animated DVD formats, although those who participated rated the experience positively. Keywords: Digital-Based Learning, Nurse Instruction, Video Game, Media Acceptability 1. Introduction Currently, patients diagnosed with cancer are likely to receive a range of information about their disease and its treatment, but there has been surprisingly little research on what that information should be, or when or how it is best to provide it [1-2]. A recent survey found that cancer patients in general regard specialist nurses as their pre- ferred source of quality information, as opposed to other sources [3], so it is important that nurses are capable as providers and communicators. 1.1 Self Care Cancer patients may experience many adverse symptoms arising directly from the disease itself or as side effects of treatment, especially chemotherapy or radiotherapy. To a large extent, patients’ quality of life reflects their ability to learn certain strategies, which used either as preventive or reactive measures, can reduce the potential impact of these adverse symptoms. Such symptoms might range from psychological or cosmetic issues such as hair loss or deviations from normal appearance to se- vere pain and life-threatening infections. A patient’s in- tentional use of actions to improve or maintain health and well-being is referred to as “self care”, a concept that has a central place in nursing theory [4-5] and has been sub- ject to considerable research. There is evidence that the learning and effective practice of self care skills during treatment of cancer can improve both psychosocial and physical outcomes [6-8]. But patients’ behaviour is also influenced by individual educational factors such as knowledge about self care skills, the source of such knowledge, the modality by which the knowledge is im- parted [2], and training in the use of the skills [1]. For adults being treated for cancer, there is evidence that self care skills most used are typically self-taught and based on commonsense rather than on professional advice and that these self care measures often are ineffective [9]. 1.2 Nurse Training in Patient Self-Care Instruction It appears that good self care improves treatment out- comes, and that oncology nurses are the preferred pro- viders (by patients) of self-care information. There is evidence that nurses are in general consistent in the can- cer information [10] and the self-care information [11]  Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of 52 Using Animated and DVD Formats for Nurse Instruction they believe is important to provide to patients. However, there is little research published on alternative methods of teaching nurses about patients’ self-care needs, or how to communicate effectively with patients about self-care issues. A survey of oncology nurses in the U.S. indicates that they are amenable to receiving professional informa- tion through electronic media such as CD-ROM and the Internet [12]. There are some recent indications that nurses generally are becoming more game-oriented (board games) in their educational preferences [13,14], as well as more internet-oriented [15]. Also, a greater use of internet and other digital technology for nursing educa- tion is being strongly promoted. What seems to be lack- ing though, are empirical studies of how nurses respond when asked to engage with these new initiatives in digi- tally-based education. In particular, there seem to be no published studies of nurses’ views of interactive video game or animated DVD formats as conduits for profes- sional information or interaction with patients about treatment issues. Since younger patients appear to be receptive to the idea of using these types of media as part of their treatment, it is desirable to know the views of nurses also. If nurses are positive about the potential of these media for their own education and for their interac- tions with patients, the use of the media with patients is more likely to have beneficial outcomes than would be the case if nurses take a negative view. Nurses’ percep- tion aside, it would be useful to know whether nurses benefit directly from using these digital media either in knowledge gains or in greater confidence to carry out nursing tasks. 1.3 This Study This research investigates the credibility/acceptability of two alternative interventions involving presenting educa- tional material about cancer and patient self-care to on- cology nurses. The research also examines the effects of these two interventions on nurses’ knowledge about can- cer treatment and on their perceived efficacy to commu- nicate with young patients about self-care during treat- ment. One of the interventions is an interactive video game called Re-Mission [16], designed primarily to as- sist young cancer patients (15-30 years old) to under- stand and practise self-care during treatment. The other intervention is a series of non-interactive video anima- tions that discuss the self-care issues central to the Re- Mission game. A major objective for the Re-Mission game was to fa- cilitate communication about cancer and self care be- tween patients and their treating health professionals. However, Re-Mission might also assist nurses to under- stand cancer and the self-care issues experienced by pa- tients. Also, experience with Re-Mission might assist nurses to communicate effectively with patients about their treatment and self-care issues, especially if patients are themselves using Re-Mission. Players of the Re-Mission game are exposed to its edu- cational content throughout a series of game-play mis- sions which may take 10 hours or more to complete. While this time commitment might be appropriate for patients undergoing treatment, it may be an unrealistic expectation for many nurses who already have heavy demands on their time. However, much of the educa- tional content of Re-Mission exists in the game as non- interactive animated sequences that can be presented outside the game in DVD format of about one hour’s duration. While lacking possible educational advantages of interactivity associated with game-play, this Re-Mission DVD may have advantages of its own. For example, it may be played on equipment that most nurses would have ready access to and does not require computer or video-game literacy, whereas the Re-Mission game re- quires a computer with advanced graphics capability and a degree of computer confidence. Also, the shorter play- ing time of the DVD potentially is an attractive feature for nurses with busy lives. 1.4 Re-Mission—A Brief Description Re-Mission is a 3-D video game which can be played on a computer by a player using a hand-held game controller. The game comprises 20 “missions”, in which the player can enter alternative 3-D virtual environments represent- ing selected locations inside the bodies of “virtual cancer patients”. Examples are lymph vessels, bone marrow, spinal cord, blood vessels, lungs and brain. Within these environments, the player pursues the goal of the chosen mission by controlling an avatar, in this case a humanoid character called a “nanobot”, ostensibly specialized to fight cancer. The environments contain features with which the nanobot can interact. For example, a lymph vessel, com- prising several sections connected by valves, contains animated characters which are realistic representations of various cells that might be found in the lymph system of a lymphoma patient. Game-play consists of guiding the nanobot to complete a mission to destroy cancer cells or bacteria while avoiding injury or weakness. Cells are destroyed using weapons powered by chemotherapy. Bacteria are destroyed using antibiotic. The nanobot must prompt the patient to comply with the prescribed drug regime, in order for the nanobot to have ammuni- tion for weapons. Also, the patient must be prompted to eat or drink to maintain a sufficient level of health. The characteristics of the “virtual patients”, cancer di- agnoses and treatment issues represented in Re-Mission have been selected to maximize the relevance of the game to the issues experienced by young people with cancer. The efficacy of Re-Mission as a psychoeduca- Copyright © 2010 SciRes. CE  Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of 53 Using Animated and DVD Formats for Nurse Instruction tional intervention for self-care and adherence which has been evaluated in an international multi-site trial and other more-focused studies conducted with cancer pa- tients [17-19]. Re-Mission is available free to patients and clinicians from the developers, a non-profit research institute (available at www.hopelab.org). According to the developers, Re-Mission has been distributed on re- quest to more than 200,000 patients and health providers worldwide, indicating that it might be widely used by young cancer patients. 1.5 Re-Mission as a Communication Tool To the extent that Re-Mission is popular with young cancer patients, it could provide a useful context for dis- cussion of treatment issues between patients and their families or friends, and between patients and their treat- ment providers. Patients might find it relatively easy to bring up treatment issues with others if they can do so by discussing game-play scenarios, as opposed to talking directly about their own problems. In particular, discus- sions between patients and nurses, about adherence and self-care generally, might be assisted by using Re-Mis- sion scenarios. Such discussions would require that the nurses, as well as the patients, have experience with Re-Mission content. However, the acceptability to nurses of this approach is unknown and requires investigation. The current study explored this acceptability issue by giving nurses experience with Re-Mission content, either as a game or DVD, then administering a questionnaire about their perceptions of the likely value of that experi- ence in their work with patients undergoing treatment. Additionally, the study measured resulting changes in cancer knowledge and perceived self-efficacy to com- municate with patients about self care. 1.6 Re-Mission as an Education Aid in Oncology Nursing The scenarios in the content of Re-Mission portray a number of self-care issues that have been rated as impor- tant issues by oncology professionals and patients [10, 11]. Both the game and the videos incorporated in it also provide extensive information about cancer and its treatment that is informed by recent surveys of health professionals and patients regarding patients’ information needs. It is possible that nurses using the Re-Mission game or video will have their knowledge and under- standing reinforced or extended by this experience. There is substantial evidence that these sorts of learning ex- perience help the consolidation, generalization and abil- ity to apply knowledge previously gained from other sources, such as reading and lectures [1,2]. 2. Method 2.1 Participants The participants were nurses currently work in or receiv- ing training related to oncology nursing at two hospitals in a large metropolitan city in Australia. 2.2 Design Randomized groups were used in a so-called “mixed effects” design that included a within subjects condition and a between subjects condition. The within subjects condition (repeated measures) consisted of two levels, pre-intervention (Pre) and post-intervention (Post). The between subjects condition consisted of two levels, Re-Mission game (G) and Re-Mission DVD (V). Condi- tion “G” consisted of unrestricted access for one month to the Re-Mission video game loaded on a minicomputer. Condition “V” consisted of unrestricted access to a DVD containing all the animated informational video excerpts contained in the Re-Mission game. Sample size (N = 22) was based on Cohen’s method of using standardized ef- fect sizes as a basis for calculating the required sample size [20]. Power calculations indicate that 10 participants in each of the two conditions would be sufficient to de- tect contrasts representing large effect sizes (at alpha = 0.05 and power = 0.8) in the proposed analyses. Given the practical rationale for this study, only large effect sizes on any dependent measure are likely to be of inter- est. 2.3 Procedure Ethics approval for the project was sought and obtained from the ethics review committees at both hospitals where nurses were recruited. The study was certified as meeting consensual ethics criteria for safety, possible conflicts of interest, confidentiality and informed consent. Nurses were informed about the project by the research- ers, and the project was also advertised on a website used for postgraduate nurse education (www.swahs.health.nsw. gov.au/NMPD/index). One of the researchers, a senior nurse educator, recruited participants singly or in small groups over a 2-year period. Participants were told that the minimum duration of their direct involvement in the project would be about one month. They were sequen- tially allocated to either the G or V conditions using a randomization sequence generated by a computer algo- rithm in BASIC. 1) Pre-test: All participants completed the following: Self-care knowledge test. This was an 18-item multi-choice test of knowledge related to self-care during treatment for cancer. The items in this test were based on previously published data from surveys of oncology nurses about the relative importance of different self care Copyright © 2010 SciRes. CE 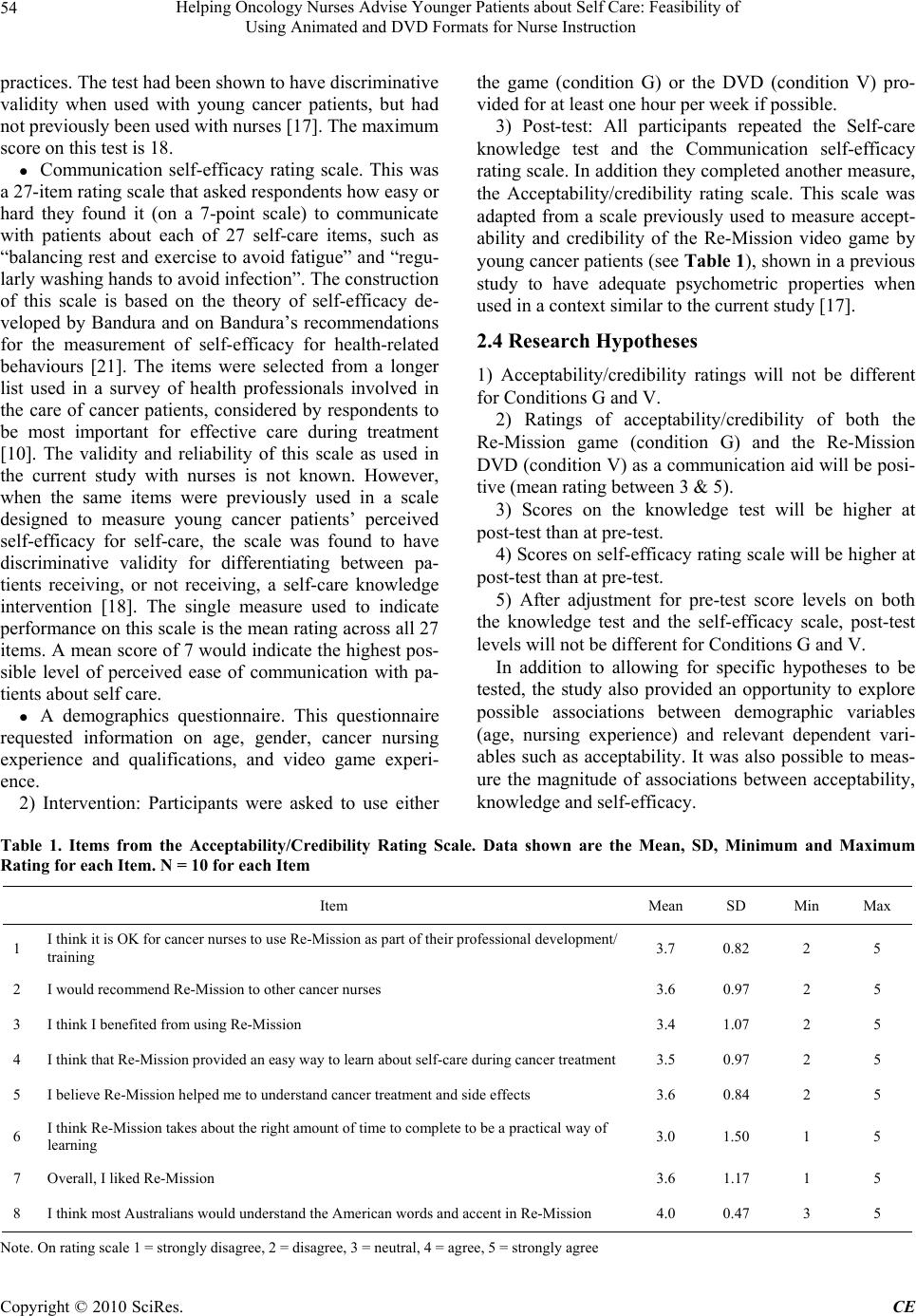 Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of Using Animated and DVD Formats for Nurse Instruction Copyright © 2010 SciRes. CE 54 practices. The test had been shown to have discriminative validity when used with young cancer patients, but had not previously been used with nurses [17]. The maximum score on this test is 18. Communication self-efficacy rating scale. This was a 27-item rating scale that asked respondents how easy or hard they found it (on a 7-point scale) to communicate with patients about each of 27 self-care items, such as “balancing rest and exercise to avoid fatigue” and “regu- larly washing hands to avoid infection”. The construction of this scale is based on the theory of self-efficacy de- veloped by Bandura and on Bandura’s recommendations for the measurement of self-efficacy for health-related behaviours [21]. The items were selected from a longer list used in a survey of health professionals involved in the care of cancer patients, considered by respondents to be most important for effective care during treatment [10]. The validity and reliability of this scale as used in the current study with nurses is not known. However, when the same items were previously used in a scale designed to measure young cancer patients’ perceived self-efficacy for self-care, the scale was found to have discriminative validity for differentiating between pa- tients receiving, or not receiving, a self-care knowledge intervention [18]. The single measure used to indicate performance on this scale is the mean rating across all 27 items. A mean score of 7 would indicate the highest pos- sible level of perceived ease of communication with pa- tients about self care. A demographics questionnaire. This questionnaire requested information on age, gender, cancer nursing experience and qualifications, and video game experi- ence. 2) Intervention: Participants were asked to use either the game (condition G) or the DVD (condition V) pro- vided for at least one hour per week if possible. 3) Post-test: All participants repeated the Self-care knowledge test and the Communication self-efficacy rating scale. In addition they completed another measure, the Acceptability/credibility rating scale. This scale was adapted from a scale previously used to measure accept- ability and credibility of the Re-Mission video game by young cancer patients (see Table 1), shown in a previous study to have adequate psychometric properties when used in a context similar to the current study [17]. 2.4 Research Hypotheses 1) Acceptability/credibility ratings will not be different for Conditions G and V. 2) Ratings of acceptability/credibility of both the Re-Mission game (condition G) and the Re-Mission DVD (condition V) as a communication aid will be posi- tive (mean rating between 3 & 5). 3) Scores on the knowledge test will be higher at post-test than at pre-test. 4) Scores on self-efficacy rating scale will be higher at post-test than at pre-test. 5) After adjustment for pre-test score levels on both the knowledge test and the self-efficacy scale, post-test levels will not be different for Conditions G and V. In addition to allowing for specific hypotheses to be tested, the study also provided an opportunity to explore possible associations between demographic variables (age, nursing experience) and relevant dependent vari- ables such as acceptability. It was also possible to meas- ure the magnitude of associations between acceptability, knowledge and self-efficacy. Table 1. Items from the Acceptability/Credibility Rating Scale. Data shown are the Mean, SD, Minimum and Maximum Rating for each Item. N = 10 for each Item Item Mean SD Min Max 1 I think it is OK for cancer nurses to use Re-Mission as part of their professional development/ training 3.7 0.82 2 5 2 I would recommend Re-Mission to other cancer nurses 3.6 0.97 2 5 3 I think I benefited from using Re-Mission 3.4 1.07 2 5 4 I think that Re-Mission provided an easy way to learn about self-care during cancer treatment3.5 0.97 2 5 5 I believe Re-Mission helped me to understand cancer treatment and side effects 3.6 0.84 2 5 6 I think Re-Mission takes about the right amount of time to complete to be a practical way of learning 3.0 1.50 1 5 7 Overall, I liked Re-Mission 3.6 1.17 1 5 8 I think most Australians would understand the American words and accent in Re-Mission 4.0 0.47 3 5 N ote. On rating scale 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree  Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of 55 Using Animated and DVD Formats for Nurse Instruction 3. Results Twenty-two participants were recruited over two years. Of these, only ten (five in each condition) returned both the pre- and post-test questionnaires and tests. The char- acteristics of those completing the study were: age (M = 39.30y, SD = 11.49, range 23-53y); nursing experience (M = 6.60y, SD = 6.90, range 0.1-20y). 3.1 Data Analysis Hypotheses 1 & 2. On the Acceptability/credibility rating scale, the maximum possible rating on each item was 5. A rating of 5 would indicate strong agreement with a positive statement about the acceptability or credibility of the game or DVD. Table 1 shows the wording of the items and the mean rating and SD, across conditions G and V, for each item in the rating scale. The mean ratings vary between 3.0 (item 6) and 4.0 (item 8). Apart from item 3, which indicates a neutral position, the means for items indicate an overall weak positive rating of the Re-Mission game or video. The mean across all items was 3.55 (SD = 0.80). The difference between means on any item for conditions G and V was non-significant by independent t-test (p > 0.05). Hypotheses 3 & 5: On the Self-care knowledge test, the maximum possible score was 18. Across conditions G and V, the mean score at Pre-test was 15.2 (SD = 2.35) and at Post-test was 15.8 (SD = 1.69). The difference between Pre- and Post-test means was not significant by correlated t-test (p > 0.05). The difference between means for conditions G and V at either Pre-test or Post-test was non-significant by independent t-test (p > 0.05). A repeated measures ANOVA with condition (G vs. V) as a between-subjects factor showed that the dif- ference between Pre- and Post-test means was not sig- nificantly different for the G and V conditions (p > 0.05). Hypotheses 4 & 5: On the Communication Self-effi- cacy rating scale, the maximum possible rating on each item was 7. The score analyzed for each participant was the mean rating across all 27 items. Across conditions G and V, the mean rating at Pre-test was 5.34 (SD = 0.87) and at Post-test was 5.83 (SD = 0.88). The difference between Pre- and Post-test means was significant by correlated t-test (t(9) = –3.59, p = 0.006). The difference between means for conditions G and V at either Pre-test or Post-test was non-significant by independent t-test (p > 0.05). A repeated measures ANOVA with condition (G vs. V) as a between-subjects factor showed that the dif- ference between Pre- and Post-test means was not sig- nificantly different for the G and V conditions (p > 0.05). Associations between variables: Exploratory correla- tional analyses were conducted, using appropriate para- metric or nonparametric procedures, to test for signifi- cant associations between variables. Of particular interest was whether ratings on the acceptability/credibility scale were significantly influenced by variables such as age, nursing experience, self-care knowledge, self-care effi- cacy, or Pre-Post changes in knowledge or self-efficacy. The only significant correlations found were a set of negative correlations between scores on the knowledge test and ratings on most items of the acceptability/credi- bility rating scale, especially at Post-test. The higher the knowledge score, the lower the rating given on all items except item 7, where the correlation was not significant. Correlations at Post-test (Pearson r) were item 1, –0.61; item 2, –0.67; item 3, –0.75; item 4, –0.75; item 5, –0.69; item 6, –0.71; item 8, –0.56 (all p < 0.05). 4. Discussion Hypotheses 1 & 2 relate to the nurses’ perceptions of acceptability/credibility of the intervention they received (condition G or V) as an aid to communicating with pa- tients about self care. Relevant to these hypotheses is the great difficulty experienced by the researchers in recruit- ing participants, and the high attrition rate of those re- cruited (over 50%). Those who did complete the study mostly did not provide very positive ratings of Re-Mis- sion’s acceptability/credibility, either as a game (condi- tion G) or video (condition V). The test for Hypothesis 1, that the acceptability/credibility ratings for condition G and condition V would not be different, was weaker than was planned. This is because the low numbers of partici- pants completing the study severely reduced the statisti- cal power of the study to detect even medium-sized dif- ferences between conditions G and V on any of the de- pendent measures. It therefore remains possible that there are real differences between these two conditions that could not be detected in this study. Hypothesis 2, that participants’ ratings of acceptabil- ity/credibility of Re-Mission as a communication aid will be positive, is only weakly confirmed by the evidence. Although those completing the study mostly gave posi- tive ratings on the acceptability/credibility items (< 3), the low recruitment and completion rates suggests that most nurses approached were disinclined to get involved or to maintain their involvement. The conditions of the ethics approval for this study did not permit the re- searchers to ask nurses why they were disinclined, but some volunteered comments that suggested widespread disinterest in computer games and animated videos amongst this group. Had it been possible to use incen- tives to encourage participation in the study, it is likely that more nurses would have participated in and com- pleted the study. Hypothesis 3, that scores on the self-care knowledge test will be higher at post-test than at pre-test, was dis- confirmed, indicating that neither intervention could be said to lead to an increase in knowledge. Hypothesis 4, Copyright © 2010 SciRes. CE  Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of 56 Using Animated and DVD Formats for Nurse Instruction that scores on self-efficacy rating scale will be higher at post-test than at pre-test, was confirmed. This effect was of moderate size, representing a mean Pre-Post increase in self-efficacy ratings of about 0.5 of a scale unit. While this effect is consistent with a positive influence of Re- Mission content on perceived self-efficacy, the absence of a control for extraneous influences on self-efficacy means that other explanations of the increase in self-ef- ficacy are equally plausible. Hypothesis 5, that conditions G and V would not have different effects on either knowledge or self-efficacy, are consistent with the non-significant values obtained in the analyses conducted. Although the statistical power of the tests conducted was low consequent to the low comple- tion rate, this result is at least consistent with the conclu- sion that neither condition had more effect than the other on either knowledge or self-efficacy. An additional finding from exploratory analyses was that acceptability/credibility ratings were not positively correlated with post-test self-efficacy scores. However, participants with higher knowledge scores, especially at the Post-test, tended to rate their intervention lower on the acceptability/credibility rating scale. Essentially, those with better knowledge about self-care were less positive about the value of the intervention in this context. This effect was specific to knowledge as measured in this study, and was not associated with age, oncology nursing experience, or perceived self-efficacy to communicate about self care. We conclude that the Re-Mission game and Re-Mission videos are found to be moderately acceptable/credible to the small proportion of oncology nurses who are willing to try them, especially to those whose knowledge about self care is limited. Using the game or video may result in significant improvement in perceived self-efficacy to communicate with patients about self care. However, our results indicate that nurse educators may find substantial resistance amongst nurses to educational initiatives in- volving the use of animated games or videos. This is in contrast to the positive view of digital and game-based education strategies prevalent in the nursing education literature [13,15]. It may reflect the difference between stated and revealed preferences, for example, asking nurses their preferences between hypothetical alterna- tives, versus requesting them to participate in actual educational activities. Alternatively, the findings of the current study may be specific to the Australian context, for example, Australian nurses might be less “digitally literate” than their North American counterparts. 5. Acknowledgements This research was supported in part by HopeLab, Red- wood City, California. HopeLab gave permission for the use Re-Mission materials in this study. REFERENCES [1] I. L. Beale, A. S. Bradlyn and P. M. Kato, “Psychoeduca- tional Interventions with Pediatric Cancer Patients: Part II. Effects of Information and Skills Training on Health-Re- lated Outcomes,” Journal of Child and Family Studies, Vol. 12, No. 4, 2003, pp. 385-397. [2] A. S. Bradlyn, I. L. Beale and P. M. Kato, “Psychoeduca- tional Interventions with Pediatric Cancer Patients: Part I. Patient Information and Knowledge,” Journal of Child and Family Studies, Vol. 12, No. 3, 2003, pp. 257-277. [3] M. E. Mills and K. Sullivan, “The Importance of Infor- mation Giving for Patients Newly Diagnosed with Cancer: A Review of The Literature,” Journal of Clinical Nursing, Vol. 8, No. 6, 1999, pp. 631-642. [4] L. Levin, A. Katz and E. Holst, “Self-Care: Lay Initia- tives in Health,” Prodist, New York, 1979. [5] D. Orem, “Nursing Concepts of Practice,” 5th Edition, Mosby-Year Book, Inc, St. Louis, 1995. [6] C. Miaskowski, et al., “Self-Care Intervention to Control Cancer Pain,” Funded by NIH, National Cancer Institute, RO1 CA64734 (1996-2000), Unpublished data, 2000. [7] M. J. Dodd, P. Larson and S. L. Dibble, “Randomized Clinical Trial of Chlorhexidine Versus Placebo for Pre- vention of Oral Mucositis in Patients Receiving Chemo- therapy,” Oncology Nursing Forum, Vol. 23, No. 6, 1996, pp. 921-927. [8] M. J. Dodd and C. Miaskowski, “The Pro-Self Program: A Self-Care Intervention Program for Patients Receiving Cancer Treatment,” Seminars in Oncology Nursing, Vol. 16, 2000, pp. 300-308. [9] A. Richardson and E. K. Ream, “Self-Care Behaviours Initiated by Chemotherapy Patients in Response to Fa- tigue,” International Journal of Nursing Studies, Vol. 34, No. 1, 1997, pp. 35-43. [10] A. S. Bradlyn, et al., “Pediatric Oncology Professionals’ Perceptions of Information Needs of Adolescent Patients with Cancer,” Journal of Pediatric Oncology Nursing, Vol. 22, 2004, pp. 1-8. [11] C. Baggott, et al., “A Survey of Self-Care and Depend- ent-Care Advice Given by Pediatric Oncology Nurses,” Journal of Pediatric Oncology Nursing, Vol. 21, 2003, pp. 1-9. [12] S. C. Cobb, “Comparison of Oncology Nurse and Physi- cian Use of the Internet for Continuing...” The Journal of Continuing Education in Nursing, Vol. 34, No. 4, 2003, pp. 184-188. [13] M. A. Royse and S. E. Newton, “How Gaming is Used as an Innovative Strategy for Nursing Education,” Nursing Education Perspectives, Vol. 28, No. 5, 2007, pp. 263- 267. [14] R. J. Alpers, et al., “That’s Edu-Tainment! Using Games to Engage, Excite, and Educate,” Teaching and Learning in Nursing, Vol. 2, No. 4, 2007, pp. 144-145. [15] L. H. Neuman, “Creating New Futures in Nursing Educa- Copyright © 2010 SciRes. CE  Helping Oncology Nurses Advise Younger Patients about Self Care: Feasibility of Using Animated and DVD Formats for Nurse Instruction Copyright © 2010 SciRes. CE 57 tion: Envisioning the Evolution of E-Nursing Education,” Nursing Education Perspectives, Vol. 27, No. 1, 2006, pp. 12-15. [16] HopeLab, Re-Mission (video game). HopeLab Foundation Inc: Redwood, CA, 2006, [17] I. L. Beale, et al., “Improvement in Cancer-Related Know- ledge Following Use of a Psychoeducational Video Game for Adolescents and Young Adults with Cancer,” Journal of Adolescent Health, Vol. 41, No. 3, 2007, pp. 263-270. [18] P. M. Kato, S. W. Cole, A. S. Bradlyn and B. H. Pollock, “A Video Game Improves Behavioral Outcomes in Ado- lescents and Young Adults with Cancer: A Randomized Trial,” Pediatrics, Vol. 122, No. 2, 2008, pp. e305-e317. [19] I. L. Beale, et al., “Young Cancer Patients’ Perceptions of a Video Game Used to Promote Self Care,” International Electronic Journal of Health Education, Vol. 9, 2006, pp. 102-112. [20] J. Cohen, “Statistical Power Analysis for the Behavioral Sciences,” 2nd Edition, Erlbaum, Hillsdale, NJ, 1988. [21] A. Bandura, “Self-Efficacy: The Exercise of Control,” WH Freeman, New York, 1997. |