Paper Menu >>
Journal Menu >>
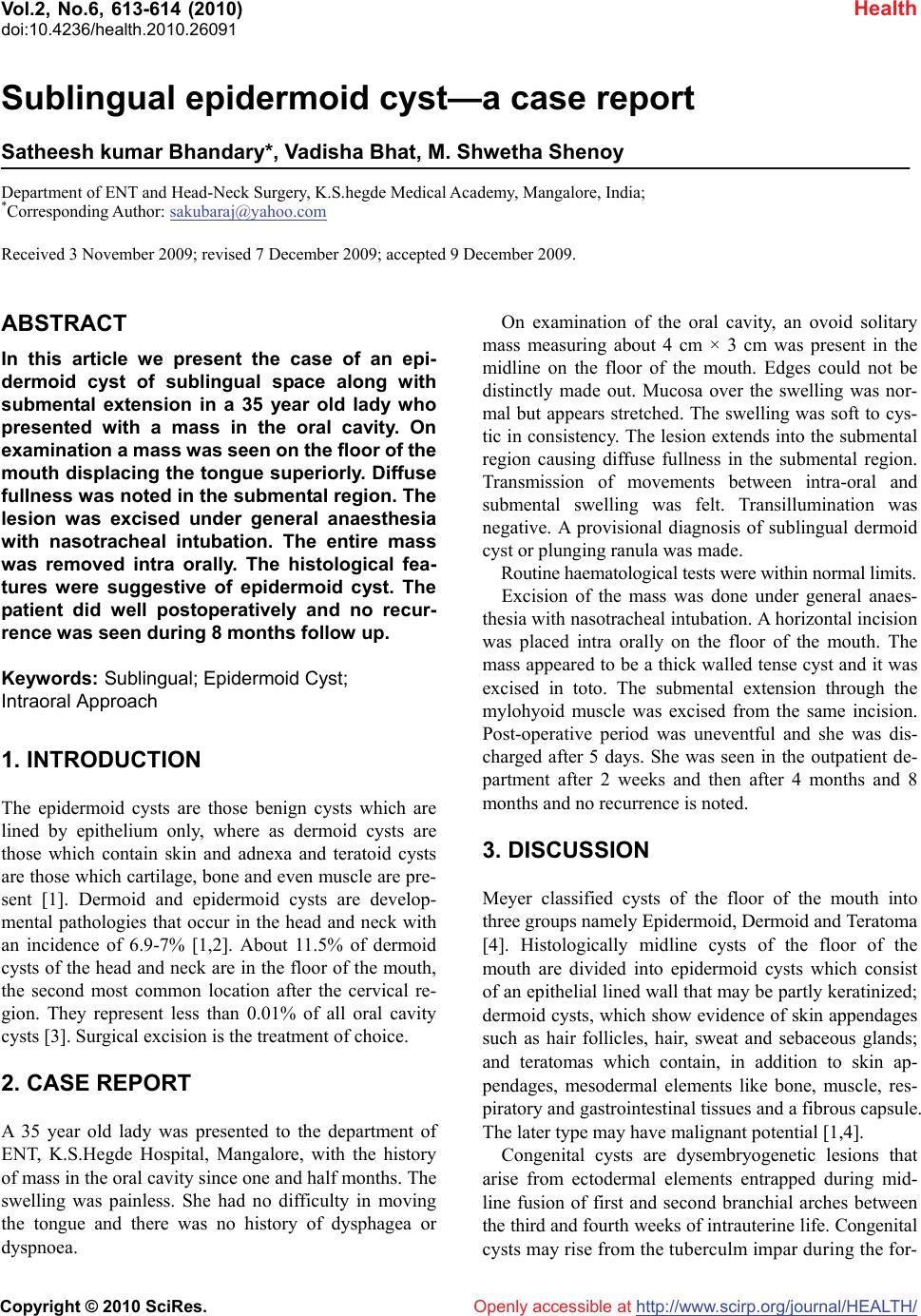 Vol.2, No.6, 613-614 (2010) Health doi:10.4236/health.2010.26091 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ Sublingual epidermoid cyst—a case report Satheesh kumar Bhandary*, Vadisha Bhat, M. Shwetha Shenoy Department of ENT and Head-Neck Surgery, K.S.hegde Medical Academy, Mangalore, India; *Corresponding Author: sakubaraj@yahoo.com Received 3 November 2009; revised 7 December 2009; accepted 9 December 2009. ABSTRACT In this article we present the case of an epi- dermoid cyst of sublingual space along with submental extension in a 35 year old lady who presented with a mass in the oral cavity. On examination a mass was seen on the floor of the mouth displacing the tongue superiorly. Diffuse fullness was noted in the submental region. The lesion was excised under general anaesthesia with nasotracheal intubation. The entire mass was removed intra orally. The histological fea- tures were suggestive of epidermoid cyst. The patient did well postoperatively and no recur- rence was seen during 8 months follow up. Keywords: Sublingual; Epidermoid Cyst; Intraoral Approach 1. INTRODUCTION The epidermoid cysts are those benign cysts which are lined by epithelium only, where as dermoid cysts are those which contain skin and adnexa and teratoid cysts are those which cartilage, bone and even muscle are pre- sent [1]. Dermoid and epidermoid cysts are develop- mental pathologies that occur in the head and neck with an incidence of 6.9-7% [1,2]. About 11.5% of dermoid cysts of the head and neck are in the floor of the mouth, the second most common location after the cervical re- gion. They represent less than 0.01% of all oral cavity cysts [3]. Surgical excision is the treatment of choice. 2. CASE REPORT A 35 year old lady was presented to the department of ENT, K.S.Hegde Hospital, Mangalore, with the history of mass in the oral cavity since one and half months. The swelling was painless. She had no difficulty in moving the tongue and there was no history of dysphagea or dyspnoea. On examination of the oral cavity, an ovoid solitary mass measuring about 4 cm × 3 cm was present in the midline on the floor of the mouth. Edges could not be distinctly made out. Mucosa over the swelling was nor- mal but appears stretched. The swelling was soft to cys- tic in consistency. The lesion extends into the submental region causing diffuse fullness in the submental region. Transmission of movements between intra-oral and submental swelling was felt. Transillumination was negative. A provisional diagnosis of sublingual dermoid cyst or plunging ranula was made. Routine haematological tests were within normal limits. Excision of the mass was done under general anaes- thesia with nasotracheal intubation. A horizontal incision was placed intra orally on the floor of the mouth. The mass appeared to be a thick walled tense cyst and it was excised in toto. The submental extension through the mylohyoid muscle was excised from the same incision. Post-operative period was uneventful and she was dis- charged after 5 days. She was seen in the outpatient de- partment after 2 weeks and then after 4 months and 8 months and no recurrence is noted. 3. DISCUSSION Meyer classified cysts of the floor of the mouth into three groups namely Epidermoid, Dermoid and Teratoma [4]. Histologically midline cysts of the floor of the mouth are divided into epidermoid cysts which consist of an epithelial lined wall that may be partly keratinized; dermoid cysts, which show evidence of skin appendages such as hair follicles, hair, sweat and sebaceous glands; and teratomas which contain, in addition to skin ap- pendages, mesodermal elements like bone, muscle, res- piratory and gastrointestinal tissues and a fibrous capsule. The later type may have malignant potential [1,4]. Congenital cysts are dysembryogenetic lesions that arise from ectodermal elements entrapped during mid- line fusion of first and second branchial arches between the third and fourth weeks of intrauterine life. Congenital cysts may rise from the tuberculm impar during the for-  S. K. Bhandary et al. / HEALTH 2 (2010) 613-614 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 614 Figure 1. Excision of the cyst by Intraoral Approach. mation of the floor of the mouth [5,6]. Epidermoid cysts have thin squamous lining because of lack of dermal appendages, which rarely contains calcifications. These cysts contain debris from the des- quamation of the epithelial lining. The debris contain mainly keratin, a proteinaceous material and some cho- lesterol. These are often described as pearly tumours because of the shiny smooth waxy character of the “dry keratin” on gross inspection [1]. Dermoid cysts are well circumscribed lesions most commonly seen at the lateral canthus of the eye. They are typically lined by squamous epithelium and contain skin appendages but unlike epidermoid cyst they have a thicker lining and may contain dystrophic calcification [7]. Ultrasonographically the solid and cystic structures within a heterogenous mass and calcifications are seen Treatment is by surgical excision of intra oral cysts in the floor of the mouth to relieve symptoms caused by the cyst and possible infection. Usually intra oral incision is placed for small cysts but large ones require an external approach. Post operative complications are rare and are reduced by closely following the capsule and its com- plete removal [8]. 4. CONCLUSIONS We report a case of epidermoid cyst in the sublingual region with extension into submental region through the mylohyoid muscle, presenting as an intraoral and sub- mental swelling. The cyst was completely excised through intraoral incision without any complications and without any evidence of recurrence in 8 months follows up. REFERENCES [1] Koeller, K.K., et al. (1999) Congenital cystic masses of the neck: Radiological-Pathologic correlation. Radio- graphics, 19(1), 121-146. [2] Dimov, Z.H., et al. (2000) Dermoid, epidermoid and teratoma cysts of the tongue and oral cavity. Sofiia, 56(2), 30-32. [3] Saverio, D.P.F., et al. (2002) Sublingual Epidermoid Cyst. Journal of Craniofacial Surgery, 13(2), 308-310. [4] Calderon, S. (1993) Concomitant Sublingual and Sub- mental Epidermoid cyst of the floor of the mouth. Jour- nal of Oral and Maxillofacial Surgery, 51(7), 790-792. [5] Longo, F., et al. (2003) Midline Dermoid cysts of the floor of the mouth: Report of 16 cases and review of sur- gical techniques. Plastic and Reconstructive Surgery, 112 (6), 1560-1565. [6] De Ponte, F.S., et al. (2002) Sublingual epidermoid cyst. Journal of Craniofacial Surgery, 13(2), 308-310. [7] Smirinitopolus, J., Chiechi, M., et al. (2005) Tertomas, Dermoids and Epidermoids of the head and neck. Radio- graphics, 25(4), 931-948. [8] Leveque, H., et al. (1979) Dermoid Cyst of the floor of the mouth and lateral neck. Laryngoscope, 89(2 Pt 1), 296-305. |