Paper Menu >>
Journal Menu >>
 Vol.2, No.6, 575-581 (2010) Health doi:10.4236/health.2010.26085 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ Knowledge and health seeking behavior for malaria among the local inhabitants in an endemic area of Ethiopia: implications for control Kaliyaperumal Karunamoorthi1,2*, Abdi Kumera1 1Unit of Vector Biology & Control, Department of Environmental Health Science, College of Public Health and Medical Sciences, Jimma University, Jimma, Ethiopia 2University Research and Development Center, Bharathiar University, Coimbatore, Tamil Nadu, India; *Corresponding Author: k_karunamoorthi@yahoo.com Received 24 October 2009; revised 10 December 2009; accepted 14 December 2009. ABSTRACT This cross-sectional study was conducted to assess the knowledge and health seeking be- havior for malaria among the local inhabitants in an endemic area of Ethiopia: Implications for control. 98.6% and 80.7% of respondents had awareness about malaria and the cause (‘mos- quito bite’) of malaria, respectively. 186 (81.6%) respondents seek treatment for a febrile disease from health care facilities. Chi-square analysis revealed a strong association between the edu- cational status of respondents and the meas- ures they take to prevent malaria (Х2 = 58.7; df = 16; p < 0.001). The findings clearly suggest that the majority of the respondents had adequate knowledge and enviable health seeking behav- iour. However, still a sizable faction had mis- conception and undesirable health seeking be- haviour. It’s a major barrier to implement effec- tive malaria control strategies in the resource- limited settings particularly in country like Ethiopia. In this context, appropriate communi- cation strategies apparently inevitable. Therefore, appropriate communication strategies should be designed to promote the knowledge and health seeking behaviour of vulnerable section of the society in this vicinity. Keywords: Malaria; Knowledge; Health seeking behaviour; Ethiopia 1. INTRODUCTION Malaria remains a major cause of morbidity and mortal- ity in tropical and subtropical regions of the world, de- spite decades of malaria control efforts. There are ap- proximately 300-500 million clinical cases and about one million deaths due to malaria globally, and Africa south of the Sahara accounts for over 90% of the disease burden [1]. Most of the infections and deaths in highly endemic areas occur in children and pregnant women, who have little access to health systems [2-4]. 109 countries were endemic for malaria in 2008, 45 within the WHO African region. Ethiopia had approxi- mately 6% of malaria cases in the African Region in 2006. Malaria is present everywhere except in the cen- tral highlands. A total of 1.2 million cases were reported in 2007, the lowest number in the period 2001-2007 [5]. Over the past years, the disease has been consistently reported as the leading cause of outpatient visits, hospi- talization and death in health facilities across the country. The diverse eco-climatic condition in the country makes the malaria transmission pattern seasonal and unstable usually characterized by frequent focal and cyclic wide- spread epidemics [6]. Except for southern Africa, many countries in the con- tinent do not have successful malaria control pro- grammes due to the magnitude of the problem com- pounded by lack of adequate health infrastructure, as well as financial and human resources [7]. Vector-borne disease control programs mostly rely on controlling the parasite and/or vector and have often overlooked the importance of the target population’s knowledge, beliefs and behavior in the transmission and control of disease [8]. Malaria control programs must consider the broad, complex and interrelated factors that influence human behavior, especially now that malaria control is theo- retically within reach of even the poorest countries through the availability of insecticide treated bednets and highly effective antimalarial drug combinations [9]. Malaria protective measures are related to knowledge and beliefs of people; when they think malaria risk is low, it is more difficult to implement protective meas-  K. Karunamoorthi et al. / HEALTH 2 (2010) 575-581 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 576 ures [10]. The poor and vulnerable populations are dis- proportionately affected by malaria and the severe con- sequences of malaria are borne more by the poorest [11]. Studies on knowledge, attitudes and practices are be- coming more important to design and improve malaria control activities, to establish epidemiological and be- havioral baselines and to identify indicators for moni- toring programs [12]. Poor knowledge about malaria was significant factor for death from malaria among the household members in Sudan [13]. Thus, there is an urgent call for updated in- formation on key sociocultural, socio-economic indictors and human understanding about malaria to apply appro- priate control strategies. Therefore, the purpose of this study was to assess the knowledge and health seeking behavior for malaria among the local inhabitants in an endemic area of Ethiopia: Implications for control. The present study findings could provide baseline informa- tion to design effective and sustainable malaria control strategies suited to local conditions in the near future. 2. MATERIALS AND METHODS 2.1. Study Settings The study was conducted in Serbo town, which is lo- cated 345km south-west of the capital Addis Ababa in Oromia Regional State, south-western Ethiopia. It’s lo- cated between latitudes 7º35-8º00 N, and between lon- gitudes 36º46-37º14 E, at altitudes between 1,740-2,660 m above sea level and has a mean annual temperature of 19°C. According to the 2005 census, the study area had a total population of 6,115 and 511 households. Malaria is the major health problem in the Serbo town. As the six consecutive years data (2002-2007) from Serbo Health Center showed, the number of malaria cases ranged be- tween 3,925 and 22,938, with the peak being during 2004/5. The prevalence seems decreasing although the number of cases per year is still high [14]. The main socio-economic activities of the local communities are small business, subsistence mixed farming involving the cultivation of staple crops (maize, teff and sorghum), and cattle and small stock raising. 2.2. Study Design The study was a descriptive cross-sectional survey. A structured questionnaire was designed and administered by trained field workers. The first part of the question- naire included sociodemographic characteristics, whereas the second part had questions on, adult residents' know- ledge and perceptions about malaria transmission, cause, treatment seeking patterns, preventive measures and practices. To improve the quality of the data, pre-testing of the questionnaire was carried out prior to the actual data collection. The questionnaire was tested on ten re- spondents by the enumerators, in an area different from the study area, but with a similar socio-demographic pattern. 2.3. Data Collection The questionnaire was administered to 228 randomly selected households between January and March 2009. The head of household or a responsible adult was inter- viewed. Only one person per household was interviewed. To minimize bias information and variables the ques- tionnaire prepared in English language was translated into native local language Amharic to make it easy to understand and to administer by interviewers and inter- viewees. 2.4. Ethical Considerations The study was approved by the ethical clearance com- mittee of the Jimma University, Jimma, Ethiopia. Before the commencement of the survey, meetings with com- munity health workers, community leaders and members of the neighborhood associations were held in which the objectives of the survey were clearly explained. Written consent was obtained from each study participant. Every participant was assured to withdraw the interview at any phase if they wish to do so. However, all the informants actively involved and no one declined to finish the inter- view. 2.5. Statistical Analysis Statistical analysis was carried out using SPSS, version 9.0. Range and mean were analysed and appropriate ta- bles, graphs and percentage were displayed. Level of significance also determined by using 95% of confi- dence intervals and p-value. 3. RESULTS 3.1. Characteristics of Study Population The socio-demographic characteristics of respondents are presented in Table 1. The study participants consisted of 46.5% males and 53.5% females. Majority of the re- spondents (44.3%) were in between 20-29 years old. 33.5% of the study population had no formal education. About 34.7% of the participants monthly income was 20-30 USD (Table 1). 3.2. Knowledge and Perceptions of Respondents about Malaria Cause, Transmission and Mosquitoes Breeding Sites Tables 2 presents respondents awareness about malaria 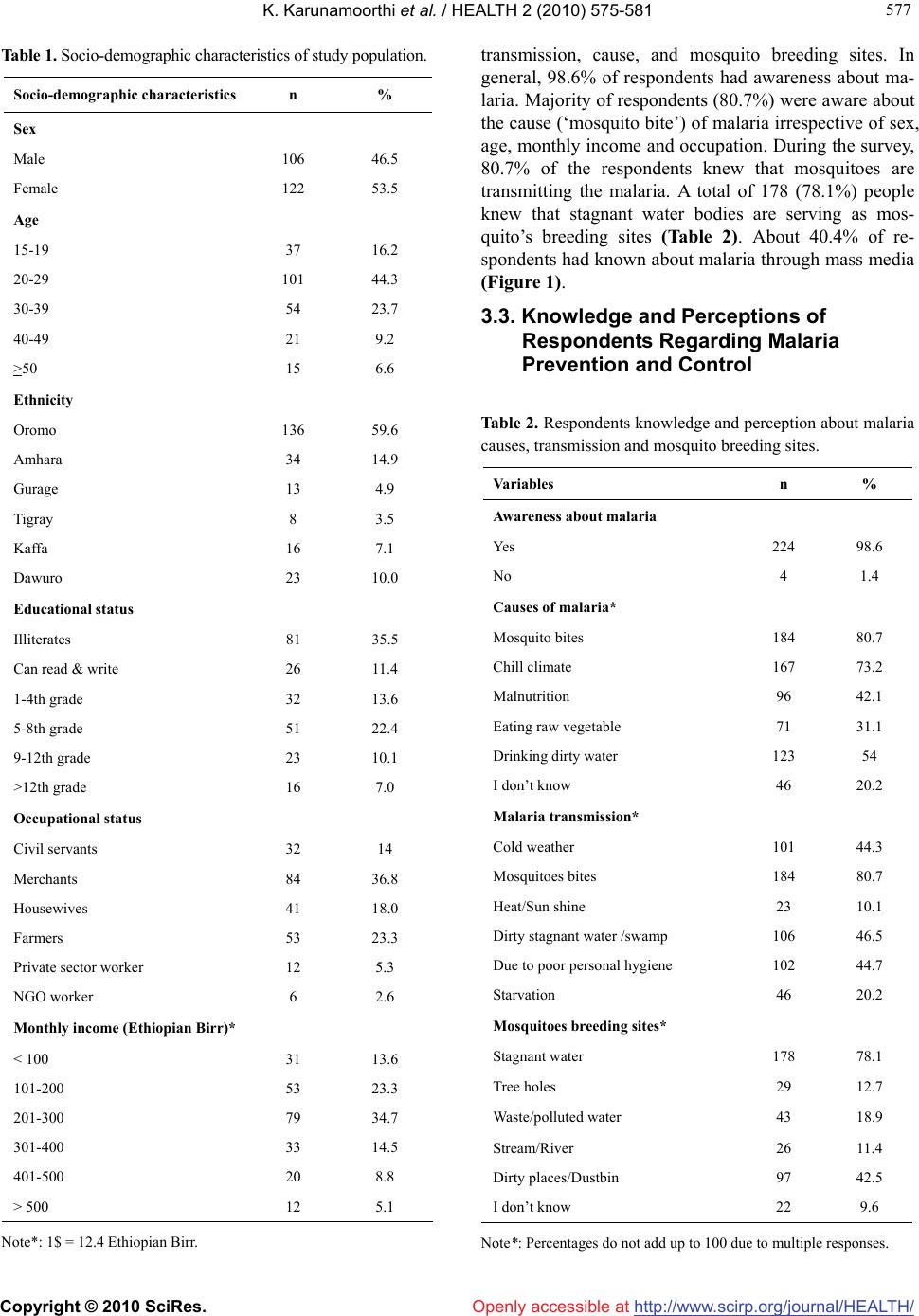 K. Karunamoorthi et al. / HEALTH 2 (2010) 575-581 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 577 577 Table 1. Socio-demographic characteristics of study population. Socio-demographic characteristicsn % Sex Male 106 46.5 Female 122 53.5 Age 15-19 37 16.2 20-29 101 44.3 30-39 54 23.7 40-49 21 9.2 >50 15 6.6 Ethnicity Oromo 136 59.6 Amhara 34 14.9 Gurage 13 4.9 Tigray 8 3.5 Kaffa 16 7.1 Dawuro 23 10.0 Educational status Illiterates 81 35.5 Can read & write 26 11.4 1-4th grade 32 13.6 5-8th grade 51 22.4 9-12th grade 23 10.1 >12th grade 16 7.0 Occupational status Civil servants 32 14 Merchants 84 36.8 Housewives 41 18.0 Farmers 53 23.3 Private sector worker 12 5.3 NGO worker 6 2.6 Monthly income (Ethiopian Birr)* < 100 31 13.6 101-200 53 23.3 201-300 79 34.7 301-400 33 14.5 401-500 20 8.8 > 500 12 5.1 Note*: 1$ = 12.4 Ethiopian Birr. transmission, cause, and mosquito breeding sites. In general, 98.6% of respondents had awareness about ma- laria. Majority of respondents (80.7%) were aware about the cause (‘mosquito bite’) of malaria irrespective of sex, age, monthly income and occupation. During the survey, 80.7% of the respondents knew that mosquitoes are transmitting the malaria. A total of 178 (78.1%) people knew that stagnant water bodies are serving as mos- quito’s breeding sites (Table 2). About 40.4% of re- spondents had known about malaria through mass media (Figure 1). 3.3. Knowledge and Perceptions of Respondents Regarding Malaria Prevention and Control Table 2. Respondents knowledge and perception about malaria causes, transmission and mosquito breeding sites. Variables n % Awareness about malaria Yes 224 98.6 No 4 1.4 Causes of malaria* Mosquito bites 184 80.7 Chill climate 167 73.2 Malnutrition 96 42.1 Eating raw vegetable 71 31.1 Drinking dirty water 123 54 I don’t know 46 20.2 Malaria transmission* Cold weather 101 44.3 Mosquitoes bites 184 80.7 Heat/Sun shine 23 10.1 Dirty stagnant water /swamp 106 46.5 Due to poor personal hygiene 102 44.7 Starvation 46 20.2 Mosquitoes breeding sites* Stagnant water 178 78.1 Tree holes 29 12.7 Waste/polluted water 43 18.9 Stream/River 26 11.4 Dirty places/Dustbin 97 42.5 I don’t know 22 9.6 Note*: Percentages do not add up to 100 due to multiple responses. 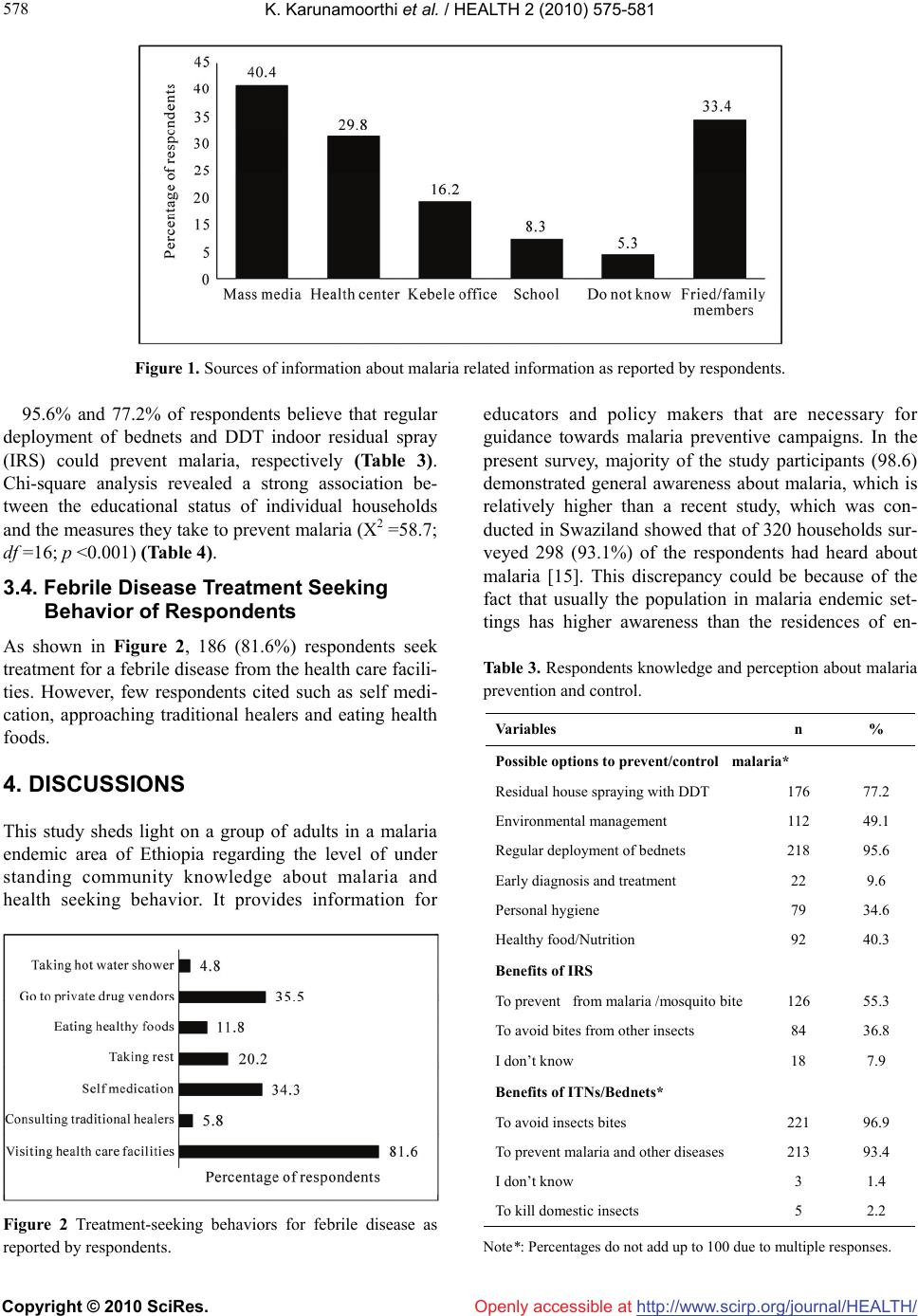 K. Karunamoorthi et al. / HEALTH 2 (2010) 575-581 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 578 Figure 1. Sources of information about malaria related information as reported by respondents. 95.6% and 77.2% of respondents believe that regular deployment of bednets and DDT indoor residual spray (IRS) could prevent malaria, respectively (Table 3). Chi-square analysis revealed a strong association be- tween the educational status of individual households and the measures they take to prevent malaria (Х2 =58.7; df =16; p <0.001) (Table 4). 3.4. Febrile Disease Treatment Seeking Behavior of Respondents As shown in Figure 2, 186 (81.6%) respondents seek treatment for a febrile disease from the health care facili- ties. However, few respondents cited such as self medi- cation, approaching traditional healers and eating health foods. 4. DISCUSSIONS This study sheds light on a group of adults in a malaria endemic area of Ethiopia regarding the level of under standing community knowledge about malaria and health seeking behavior. It provides information for Figure 2 Treatment-seeking behaviors for febrile disease as reported by respondents. educators and policy makers that are necessary for guidance towards malaria preventive campaigns. In the present survey, majority of the study participants (98.6) demonstrated general awareness about malaria, which is relatively higher than a recent study, which was con- ducted in Swaziland showed that of 320 households sur- veyed 298 (93.1%) of the respondents had heard about malaria [15]. This discrepancy could be because of the fact that usually the population in malaria endemic set- tings has higher awareness than the residences of en- Table 3. Respondents knowledge and perception about malaria prevention and control. Variables n % Possible options to prevent/control malaria* Residual house spraying with DDT 176 77.2 Environmental management 112 49.1 Regular deployment of bednets 218 95.6 Early diagnosis and treatment 22 9.6 Personal hygiene 79 34.6 Healthy food/Nutrition 92 40.3 Benefits of IRS To prevent from malaria /mosquito bite 126 55.3 To avoid bites from other insects 84 36.8 I don’t know 18 7.9 Benefits of ITNs/Bednets* To avoid insects bites 221 96.9 To prevent malaria and other diseases 213 93.4 I don’t know 3 1.4 To kill domestic insects 5 2.2 Note*: Percentages do not add up to 100 due to multiple responses.  K. Karunamoorthi et al. / HEALTH 2 (2010) 575-581 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 579 579 Table 4. Association between mosquito preventive measures and educational status of the respondents. Educational level of the respondents Types of prevention measures Total respondents IlliteratesCan read & write1-8th grade9-12th grade >12th grade p-value Mosquito net 57 16 9 13 10 9 DDT spraying 52 3 12 22 8 7 Х2 = 58.7 Draining stagnant water 93 41 19 28 5 0 df = 16 Don’t use 13 13 0 0 0 0 p < 0.001* Burning repellent plants 13 8 4 1 0 0 Total 228 81 44 64 23 16 Note*: p<0.05 statistically significant demic/nonendemic area. In addition this study was con- ducted in urban area too. 80.7% of the respondents knew the role of mosquitoes in malaria transmission (‘mosquito bite’). The respon- dents’ level of awareness about mode of malaria trans- mission was very low when compared to the findings in previous studies carried out in Ethiopia which reported awareness levels of up to 93% [16,17]. However, it’s relatively higher than that reported in other studies 55% of the surveyed population in a nationwide study in Ma- lawi (Ziba et al., 1994) [18], 67% in Turkey [19], and 17.3% in Ethiopia [20,21]. However, many people had not known the real cause of malaria. Such misconceptions have also been reported from other studies in Ethiopia and other countries [22-24]. The present study findings were comparable with previ- ous studies in India [25] and in Ethiopia [17] although the association of malaria with mosquitoes is widespread in these communities, other causal factors of malaria such as traditional beliefs like eating maize stalks, con- tact with malaria patients, exposure to rains and cold weather, bad smell and dirty water were frequently sug- gested. The correction of such misconceptions about the relationship between mosquito bite and malaria through health education messages is very critical for the success of malaria prevention and control using ITNs [26]. 78.1% of respondents indicated that stagnant water bodies serving as potential mosquito breeding sites. Pre- vious studies in Ethiopia have also confirmed similar findings [17,27]. However, the level of awareness re- garding mosquito breeding site was relatively lower than earlier studies. Most of the respondents knew about ma- laria related information through mass media and friends/family members. Findings were consistent with a study in Ethiopia [17]. The most common source of in- formation about malaria was from relatives. Radio was ranked third after medical personnel as a major informa- tion source [28]. The great majority of the respondents believe that regular deployment of bednets and DDT indoor residual spray (IRS) could prevent insect’s bites and malaria. The findings comparable with an earlier study in Mozam- bique demonstrated that the majority of respondents as- sociate malaria with mosquitoes and are aware of vari- ous methods to prevent illness, including IRS and bed nets [29]. Table 4 Chi-square analysis suggest an asso- ciation between the educational status of individual households and the measures they take to prevent ma- laria (Х2 =58.7; df =16; p <0.001). Results consistent with an earlier study, which was conducted in Swaziland, found that most respondents believed that malaria is preventable, and mentioned clinic, spraying and the use of bed nets as key malaria preventive measures. Despite these positive responses a substantial number of them (43.4%) did not take any personal protective measures against malaria infection [15]. Indeed, several studies across the globe particularly in Africa evidently suggest that Bednets/Insecticide-treated nets are regarded as one of the most effective prevention methods and sleeping under the protection of bednets could substantially re- duce the malaria burden. Another interesting finding was that the majority of the respondents preferred to seek treatment in the health facilities rather than approaching traditional healers and self medication. This may be due to the fact that the Serbo health center is located within the study area as result accessibility is extremely high among the local inhabitants. In addition, it’s providing services free of charge. The present study findings are comparable with few earlier studies. In Ethiopia, 98% respondents had their first visit to health care facilities including public and private health services as well as malaria control laboratories, drug venders/pharmacy and CHWs seeking treatment for malaria [17]. Another study in Swaziland found that almost 90% of the respondents seek treatment in the health facilities [15]. The scope of malaria control is changing worldwide. With less emphasis being placed on insecticide use, in- 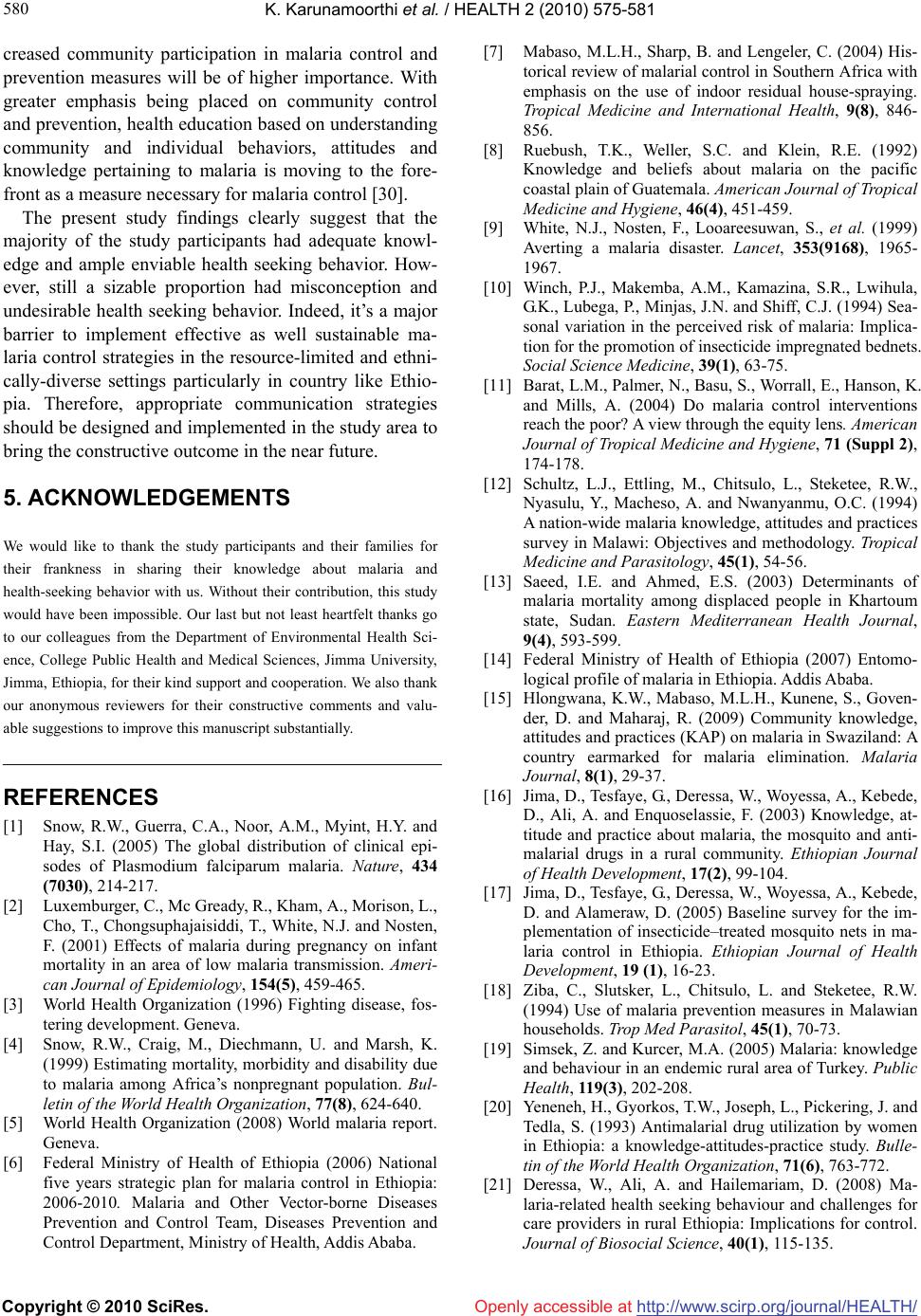 K. Karunamoorthi et al. / HEALTH 2 (2010) 575-581 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 580 creased community participation in malaria control and prevention measures will be of higher importance. With greater emphasis being placed on community control and prevention, health education based on understanding community and individual behaviors, attitudes and knowledge pertaining to malaria is moving to the fore- front as a measure necessary for malaria control [30]. The present study findings clearly suggest that the majority of the study participants had adequate knowl- edge and ample enviable health seeking behavior. How- ever, still a sizable proportion had misconception and undesirable health seeking behavior. Indeed, it’s a major barrier to implement effective as well sustainable ma- laria control strategies in the resource-limited and ethni- cally-diverse settings particularly in country like Ethio- pia. Therefore, appropriate communication strategies should be designed and implemented in the study area to bring the constructive outcome in the near future. 5. ACKNOWLEDGEMENTS We would like to thank the study participants and their families for their frankness in sharing their knowledge about malaria and health-seeking behavior with us. Without their contribution, this study would have been impossible. Our last but not least heartfelt thanks go to our colleagues from the Department of Environmental Health Sci- ence, College Public Health and Medical Sciences, Jimma University, Jimma, Ethiopia, for their kind support and cooperation. We also thank our anonymous reviewers for their constructive comments and valu- able suggestions to improve this manuscript substantially. REFERENCES [1] Snow, R.W., Guerra, C.A., Noor, A.M., Myint, H.Y. and Hay, S.I. (2005) The global distribution of clinical epi- sodes of Plasmodium falciparum malaria. Nature, 434 (7030), 214-217. [2] Luxemburger, C., Mc Gready, R., Kham, A., Morison, L., Cho, T., Chongsuphajaisiddi, T., White, N.J. and Nosten, F. (2001) Effects of malaria during pregnancy on infant mortality in an area of low malaria transmission. Ameri- can Journal of Epidemiology, 154(5), 459-465. [3] World Health Organization (1996) Fighting disease, fos- tering development. Geneva. [4] Snow, R.W., Craig, M., Diechmann, U. and Marsh, K. (1999) Estimating mortality, morbidity and disability due to malaria among Africa’s nonpregnant population. Bul- letin of the World Health Organization, 77(8), 624-640. [5] World Health Organization (2008) World malaria report. Geneva. [6] Federal Ministry of Health of Ethiopia (2006) National five years strategic plan for malaria control in Ethiopia: 2006-2010. Malaria and Other Vector-borne Diseases Prevention and Control Team, Diseases Prevention and Control Department, Ministry of Health, Addis Ababa. [7] Mabaso, M.L.H., Sharp, B. and Lengeler, C. (2004) His- torical review of malarial control in Southern Africa with emphasis on the use of indoor residual house-spraying. Tropical Medicine and International Health, 9(8), 846- 856. [8] Ruebush, T.K., Weller, S.C. and Klein, R.E. (1992) Knowledge and beliefs about malaria on the pacific coastal plain of Guatemala. American Journal of Tropical Medicine and Hygiene, 46(4), 451-459. [9] White, N.J., Nosten, F., Looareesuwan, S., et al. (1999) Averting a malaria disaster. Lancet, 353(9168), 1965- 1967. [10] Winch, P.J., Makemba, A.M., Kamazina, S.R., Lwihula, G.K., Lubega, P., Minjas, J.N. and Shiff, C.J. (1994) Sea- sonal variation in the perceived risk of malaria: Implica- tion for the promotion of insecticide impregnated bednets. Social Science Medicine, 39(1), 63-75. [11] Barat, L.M., Palmer, N., Basu, S., Worrall, E., Hanson, K. and Mills, A. (2004) Do malaria control interventions reach the poor? A view through the equity lens. American Journal of Tropical Medicine and Hygiene, 71 (Suppl 2), 174-178. [12] Schultz, L.J., Ettling, M., Chitsulo, L., Steketee, R.W., Nyasulu, Y., Macheso, A. and Nwanyanmu, O.C. (1994) A nation-wide malaria knowledge, attitudes and practices survey in Malawi: Objectives and methodology. Tropical Medicine and Parasitology, 45(1), 54-56. [13] Saeed, I.E. and Ahmed, E.S. (2003) Determinants of malaria mortality among displaced people in Khartoum state, Sudan. Eastern Mediterranean Health Journal, 9(4), 593-599. [14] Federal Ministry of Health of Ethiopia (2007) Entomo- logical profile of malaria in Ethiopia. Addis Ababa. [15] Hlongwana, K.W., Mabaso, M.L.H., Kunene, S., Goven- der, D. and Maharaj, R. (2009) Community knowledge, attitudes and practices (KAP) on malaria in Swaziland: A country earmarked for malaria elimination. Malaria Journal, 8(1), 29-37. [16] Jima, D., Tesfaye, G., Deressa, W., Woyessa, A., Kebede, D., Ali, A. and Enquoselassie, F. (2003) Knowledge, at- titude and practice about malaria, the mosquito and anti- malarial drugs in a rural community. Ethiopian Journal of Health Development, 17(2), 99-104. [17] Jima, D., Tesfaye, G., Deressa, W., Woyessa, A., Kebede, D. and Alameraw, D. (2005) Baseline survey for the im- plementation of insecticide–treated mosquito nets in ma- laria control in Ethiopia. Ethiopian Journal of Health Development, 19 (1), 16-23. [18] Ziba, C., Slutsker, L., Chitsulo, L. and Steketee, R.W. (1994) Use of malaria prevention measures in Malawian households. Trop Med Parasitol, 45(1), 70-73. [19] Simsek, Z. and Kurcer, M.A. (2005) Malaria: knowledge and behaviour in an endemic rural area of Turkey. Public Health, 119(3), 202-208. [20] Yeneneh, H., Gyorkos, T.W., Joseph, L., Pickering, J. and Tedla, S. (1993) Antimalarial drug utilization by women in Ethiopia: a knowledge-attitudes-practice study. Bulle- tin of the World Health Organization, 71(6), 763-772. [21] Deressa, W., Ali, A. and Hailemariam, D. (2008) Ma- laria-related health seeking behaviour and challenges for care providers in rural Ethiopia: Implications for control. Journal of Biosocial Science, 40(1), 115-135. 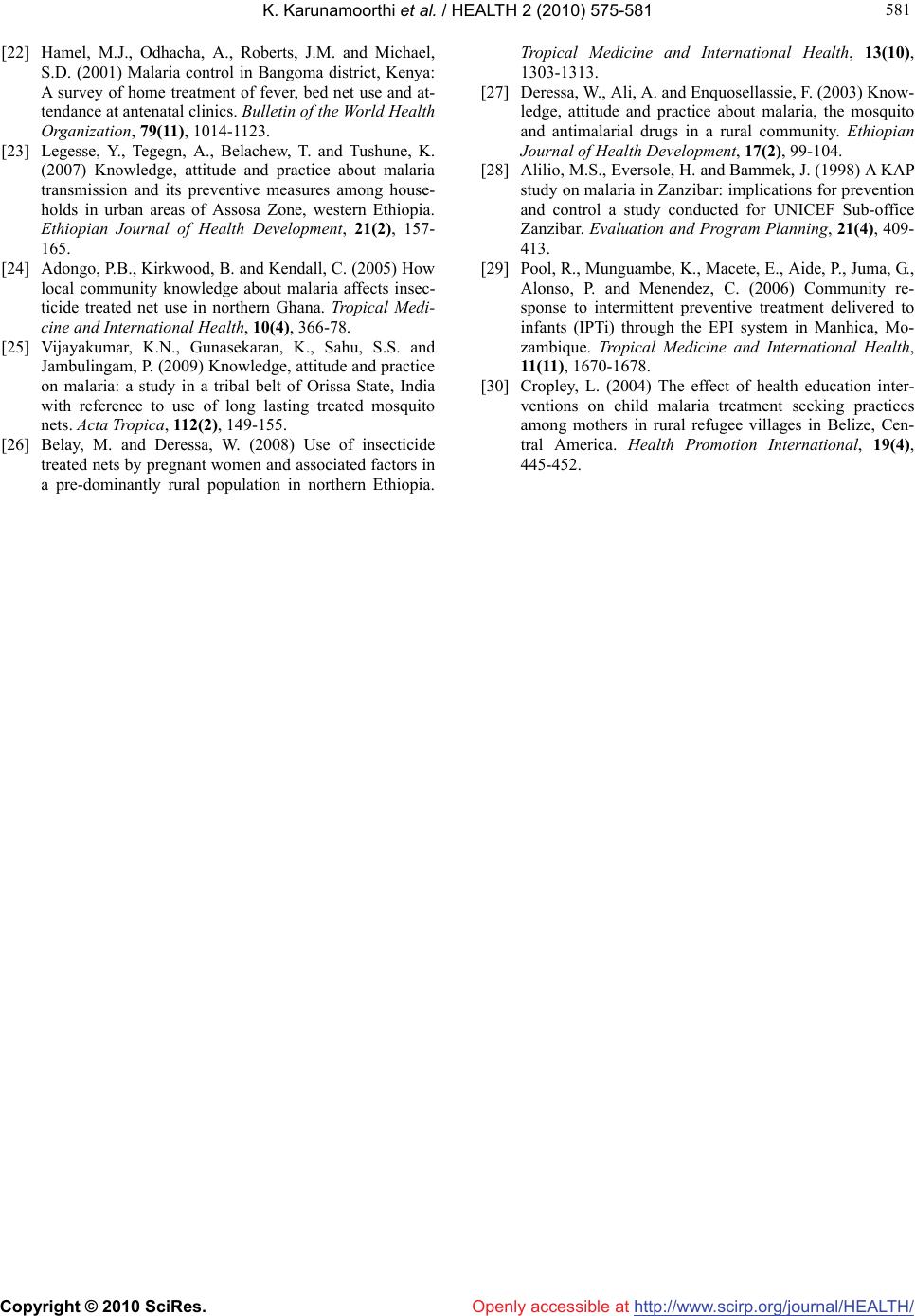 K. Karunamoorthi et al. / HEALTH 2 (2010) 575-581 Copyright © 2010 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/ 581 581 [22] Hamel, M.J., Odhacha, A., Roberts, J.M. and Michael, S.D. (2001) Malaria control in Bangoma district, Kenya: A survey of home treatment of fever, bed net use and at- tendance at antenatal clinics. Bulletin of the World Health Organization, 79(11), 1014-1123. [23] Legesse, Y., Tegegn, A., Belachew, T. and Tushune, K. (2007) Knowledge, attitude and practice about malaria transmission and its preventive measures among house- holds in urban areas of Assosa Zone, western Ethiopia. Ethiopian Journal of Health Development, 21(2), 157- 165. [24] Adongo, P.B., Kirkwood, B. and Kendall, C. (2005) How local community knowledge about malaria affects insec- ticide treated net use in northern Ghana. Tropical Medi- cine and International Health, 10(4), 366-78. [25] Vijayakumar, K.N., Gunasekaran, K., Sahu, S.S. and Jambulingam, P. (2009) Knowledge, attitude and practice on malaria: a study in a tribal belt of Orissa State, India with reference to use of long lasting treated mosquito nets. Acta Tropica, 112(2), 149-155. [26] Belay, M. and Deressa, W. (2008) Use of insecticide treated nets by pregnant women and associated factors in a pre-dominantly rural population in northern Ethiopia. Tropical Medicine and International Health, 13(10), 1303-1313. [27] Deressa, W., Ali, A. and Enquosellassie, F. (2003) Know- ledge, attitude and practice about malaria, the mosquito and antimalarial drugs in a rural community. Ethiopian Journal of Health Development, 17(2), 99-104. [28] Alilio, M.S., Eversole, H. and Bammek, J. (1998) A KAP study on malaria in Zanzibar: implications for prevention and control a study conducted for UNICEF Sub-office Zanzibar. Evaluation and Program Planning, 21(4), 409- 413. [29] Pool, R., Munguambe, K., Macete, E., Aide, P., Juma, G., Alonso, P. and Menendez, C. (2006) Community re- sponse to intermittent preventive treatment delivered to infants (IPTi) through the EPI system in Manhica, Mo- zambique. Tropical Medicine and International Health, 11(11), 1670-1678. [30] Cropley, L. (2004) The effect of health education inter- ventions on child malaria treatment seeking practices among mothers in rural refugee villages in Belize, Cen- tral America. Health Promotion International, 19(4), 445-452. |