Vol.1, No.1, 1-4 (2012) Modern Chemotherapy
http://dx.doi.org/10.4236/mc.2012.11001
Can we achieve complete remission in locally
advanced unresectable Hepatocellular Carcinoma
(HCC) by using Sorafenib? Case report and review
of literature from Qatar
Kakil Ibrahim Rasul
National Center for Cancer Care and Research (NCCCR), Doha, Qatar; kakil954@yahoo.com
Received 7 May 2012; revised 20 June 2012; accepted 18 July 2012
ABSTRACT
Patients with HCC continue to have a dismal
prognosis, with 1-year and 3-year survival rates
of 36 and 17%, respectively. This is in part re-
lated to more than two-thirds of tumors being
diagnosed at advanced stages, as well as a sub-
stantial portion of patients with early HCC failing
to receive potentially curative treatments. Sys-
temic therapy for advanced unresectable HCC
limited until the discovery of sorafenib, we are
reporting a 53 year patient with unresectable HCC
achieved complete remission clinically, radiolo-
gically and biochemically with sorafenib which
is the first case report.
Keywords: Hepatocellular Ca; Sorafenib;
Chemoembolization
1. INTRODUCTION
Patients with HCC continue to have a dismal progno-
sis, with 1-year and 3-year survival rates of 36 and 17%,
respectively [1]. Sorafenib (Nexavar Payer-Schering) is
the only systemic therapy indicated to treat HCC, in two
Phase III studies (SHARP and Asia-Pacific). Sorafenib
significantly improved OS in patients with unresectable
HCC (uHCC) [2,3]. There is no report of complete re-
mission in all the studies used sorafenib in unresectable
HCC.
The efficacy of sorafenib has been recently investi-
gated in a phase III trial, reported in abstract form at the
2007 American Society of Clinical Oncology meeting.
LLovet and colleagues randomized 602 patients with
Child Class A cirrhosis and hepatocellular carcinoma to
sorafenib versus placebo group [4]. The overall results
were encouraging. Treatment with sorafenib significantly
improved survival (hazard ratio for all cause mortality:
0.69, P = 0.0006). Treatment was also associated with an
increased time to disease progression (5.5 mo vs 2.8 mo)
and disease control rate (43% versus 32%). But there is
no complete remission in these studies. Overall toxicity
did not differ between treatment and placebo arm (52%
versus 54%). Based on this trial, sorafenib has become
the most promising chemotherapeutic agent in the treat-
ment of hepatocellular carcinoma in patients with pre-
served liver function.
2. CASE PRESENTATION
A 53 years male Egyptian known non insulin depen-
dent diabetes mellitus (NIDDM) on Metformin 500 mg
orally twice daily since 6 years, and HCV + ve Chronic
smoker1pack/day since 35 years On December 2010 dur-
ing follow up ultrasound examination found to have fo-
cal lesion in the liver He had mild right hypochondrial
pain which dull in nature not radiating and no associated
symptoms, his ECOG (Eastern Cooperative Oncology
Group performance status) PS is 0, Child-pugh assess-
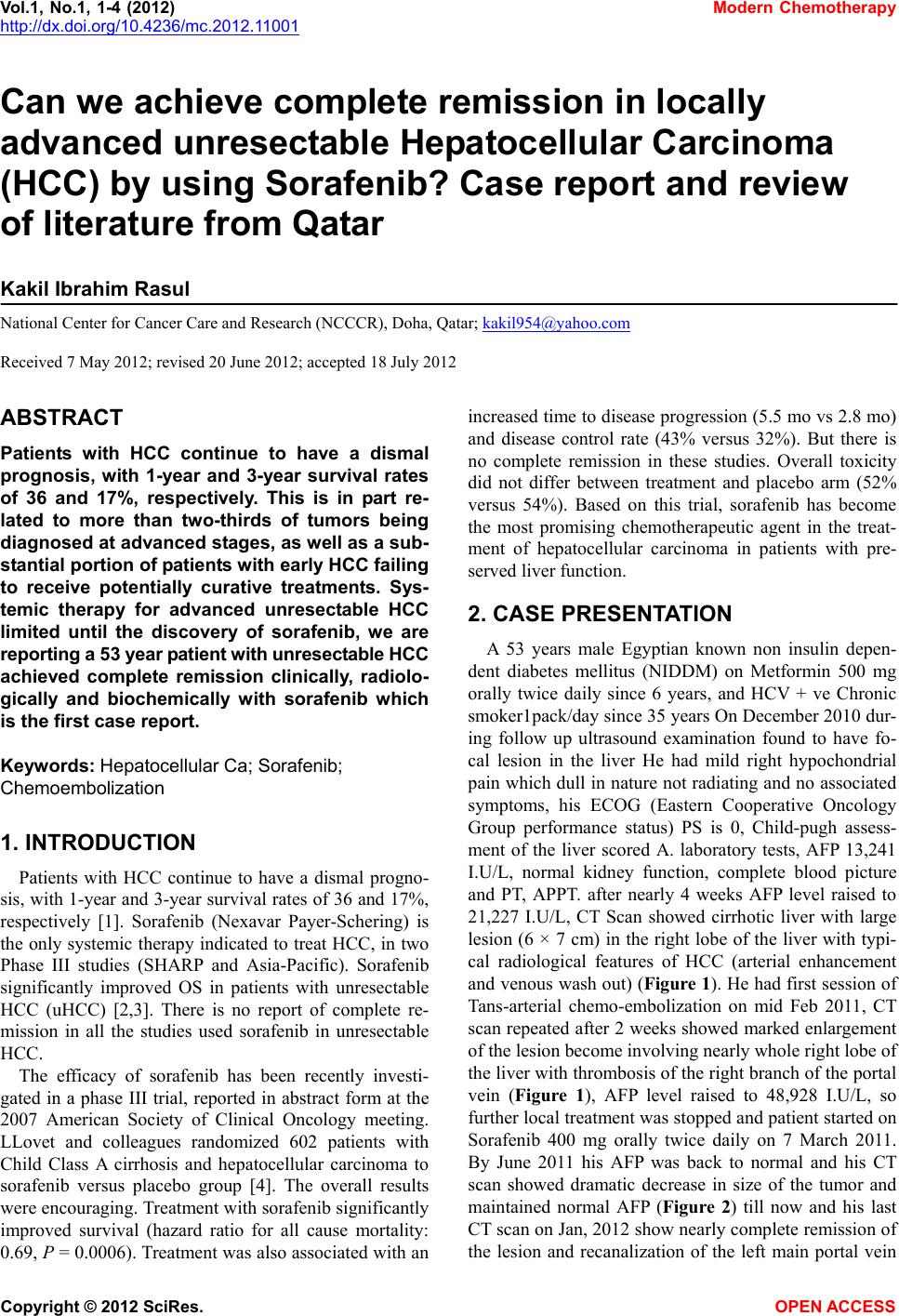
ment of the liver scored A. laboratory tests, AFP 13,241
I.U/L, normal kidney function, complete blood picture
and PT, APPT. after nearly 4 weeks AFP level raised to
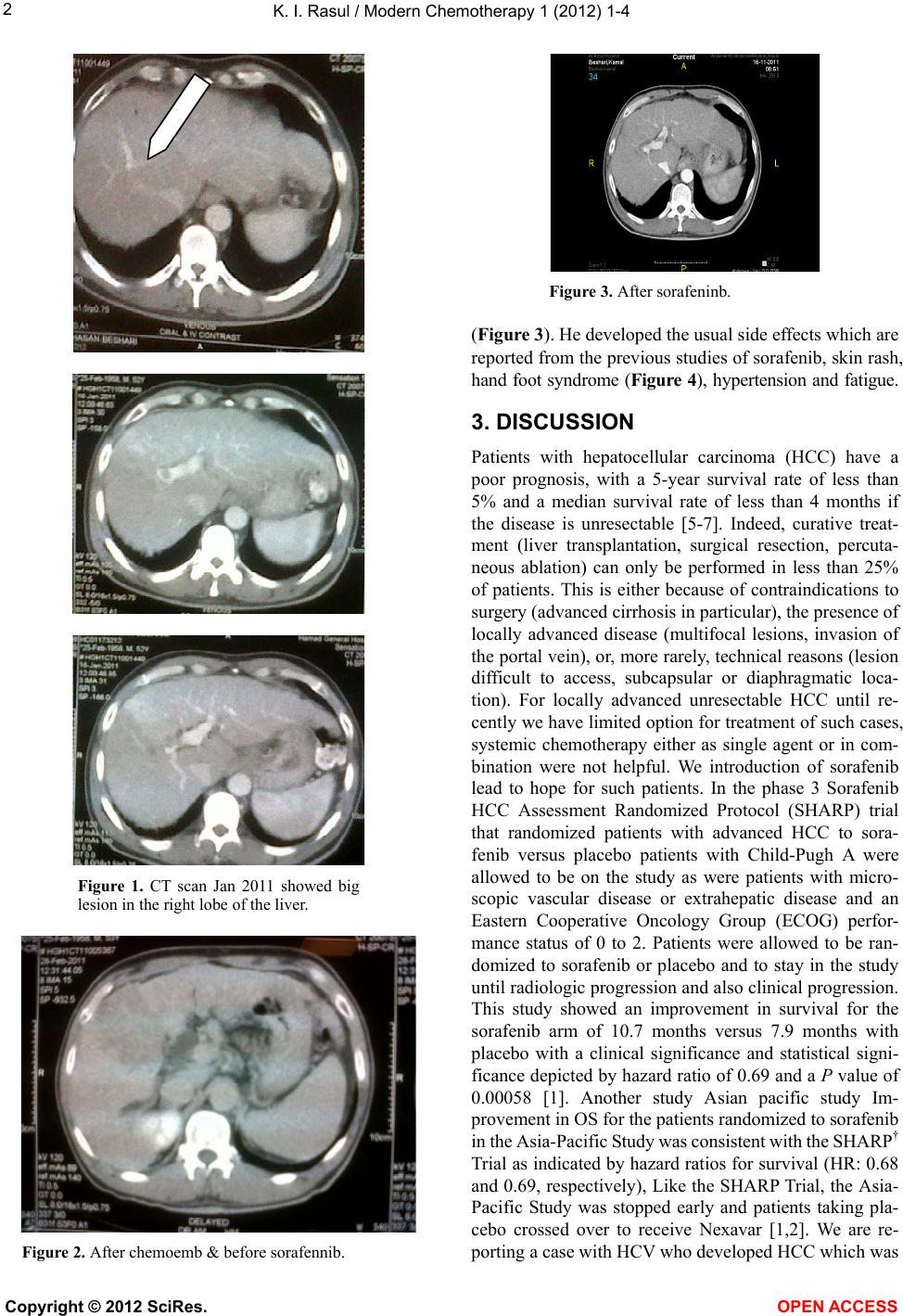
21,227 I.U/L, CT Scan showed cirrhotic liver with large
lesion (6 × 7 cm) in the right lobe of the liver with typi-
cal radiological features of HCC (arterial enhancement
and venous wash out) (Figure 1). He had first session of
Tans-arterial chemo-embolization on mid Feb 2011, CT
scan repeated after 2 weeks showed marked enlargement
of the lesion become involving nearly whole right lobe of
the liver with thrombosis of the right branch of the portal
vein (Figure 1), AFP level raised to 48,928 I.U/L, so
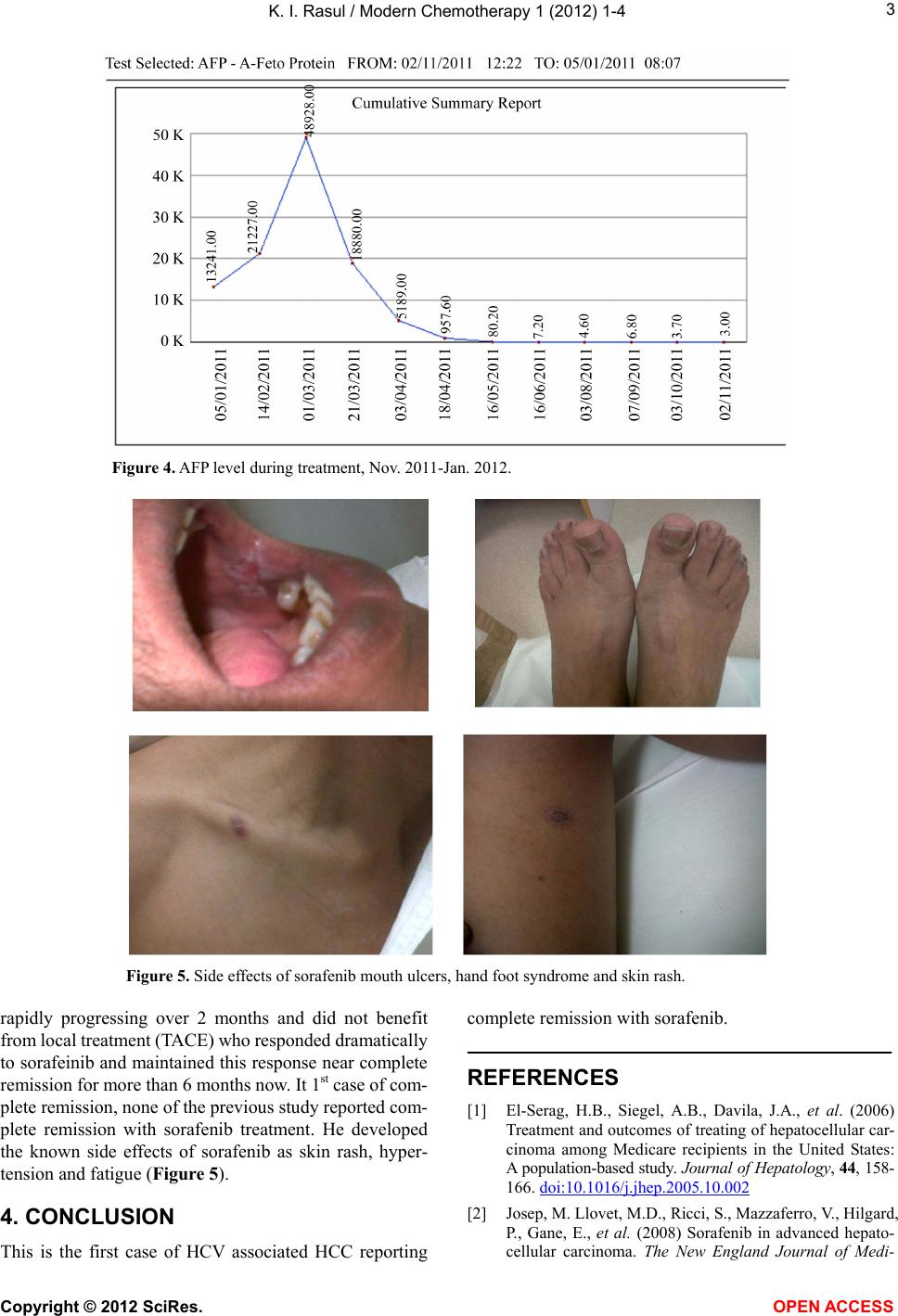
further local treatment was stopped and patient started on
Sorafenib 400 mg orally twice daily on 7 March 2011.
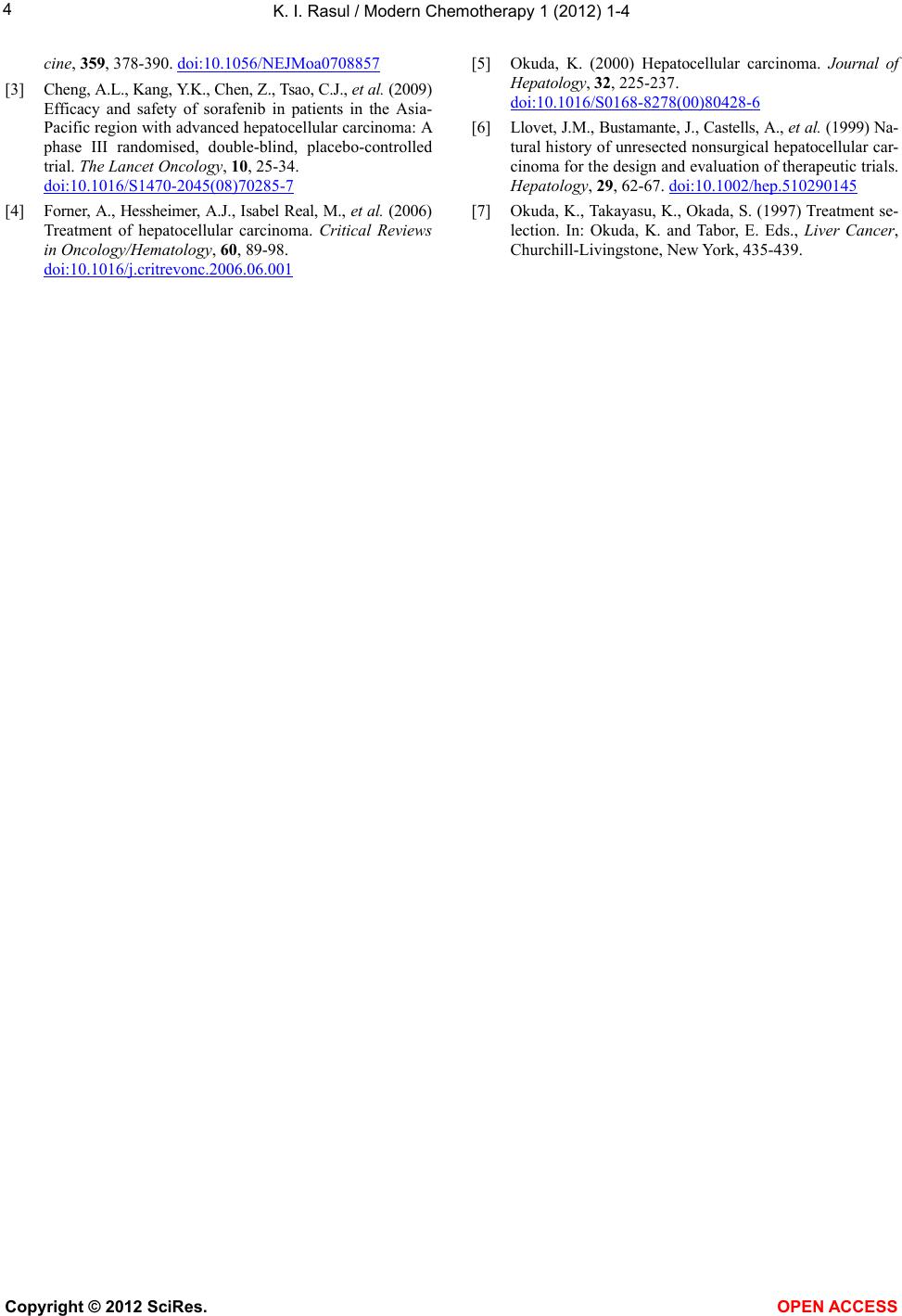
By June 2011 his AFP was back to normal and his CT
scan showed dramatic decrease in size of the tumor and
maintained normal AFP (Figure 2) till now and his last
CT scan on Jan, 2012 show nearly complete remission of
the lesion and recanalization of the left main portal vein
Copyright © 2012 SciRes. OPEN ACCESS