Open Journal of Pediatrics
Vol. 3 No. 3 (2013) , Article ID: 36369 , 2 pages DOI:10.4236/ojped.2013.33048
Congenital median raphe cysts: Coexistence of cystic lesions and canal-like lesions*
![]()
1Division of Surgery, Department of Surgical Specialties, National Center for Child Health and Development, Tokyo, Japan
2Division of Pathology, Department of Pathology, National Center for Child Health and Development, Tokyo, Japan
Email: #kanamori-y@ncchd.go.jp
Copyright © 2013 Masataka Takahashi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 24 July 2013; revised 15 August 2013; accepted 21 August 2013
Keywords: Median Raphe Cyst; Perineum; Transitional Epithelium
ABSTRACT
Median raphe cyst of the perineum is a rare congenital anomaly and was first reported in 1895. We report a 9-year-old male with median raphe cysts in the perineum which had become swollen and then spontaneously ruptured several times since he was 3 years old. There were two separate lesions; one was a cystic lesion and the other was a canal-like lesion. They were completely excised and the inner layer of the cysts was composed of transitional epithelium.
1. INTRODUCTION
Median raphe cyst is a rare congenital anomaly and was first reported in 1895 by Mermet [1]. It is considered to derive from either a urethral remnant originating at urethral formation or abnormal development of paraurethral ducts in early fetal life [2-9] and usually has a good prognosis by complete resection. We report here a male pediatric patient with median raphe cysts, which were multiple skip lesions, one was a canal-like shape and the other was a cystic shape.
2. CASE
The patient was a nine-year-old boy who visited the outpatient clinic of our institute for the treatment of lesions around the anus that repeatedly became swollen. The parents thought that it was a kind of hemorrhoid and reported that the patient experienced acute swelling of the perineal skin lesion when he was three years old and soon it ruptured and seemed to heal spontaneously. Howeversince then, he experienced swelling and rupture of the perineal lesion several times. The mother of the patient presented a photograph of the skin lesion when it was swollen (Figure 1(a)). The lesions were several cystic masses that were lined in a row on the median raphe at the perineum. When the patient came to the outpatient clinic, the lesions were not swollen and the median raphe of the perineum seemed to have an almost normal shape with slight hypertrophy (Figure 1(b)). Another skip lesion was seen at the scrotal site of the median raphe and it was a very small cystic mass of about 1 mm in size (Figure 1(b)). The lesions were excised under general anesthesia. The boundary of the lesions was restricted at the skin level and never communicated to the urethra and anal canal. The pathological diagnosis was multiple median raphe cysts whose inner layer was composed of transitional epithelium (Figures 2(a) and (b)). The postoperative course was uneventful.
3. DISCUSSION
Congenital median raphe cyst is a rare anomaly that was first reported in 1895 by Mermet [1]. This lesion was sometimes recognized when it became infected or was swollen with mucinous contents and the symptomatic lesions were treated by surgical excision. Some were pediatric cases [2,4-8], while others were adult cases [3,9]. The lesion was always located on the median raphe, and some were in the penile area while others were in the perineal area. Their shape and size were variable but they never communicated to the urethra and underlying tissues. In our case, both a cystic-type lesion and a canallike, lesion coexisted in different regions and this was a characteristic feature compared to the reported cases in the past.
The etiology of median raphe cysts was considered to be one of the following: 1) the epithelial rest becomes
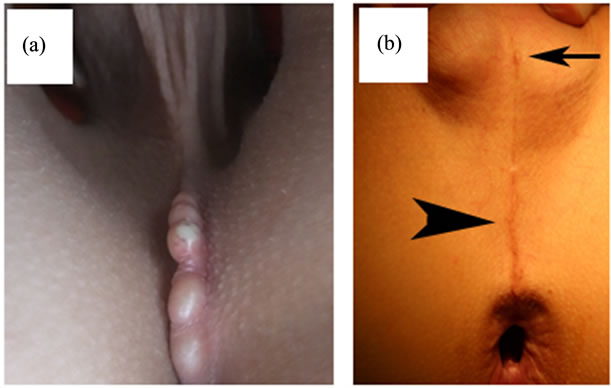
Figure 1. Macroscopic appearance of the lesions. (a) Symptomatic phase: Cystic lesions lined along the median raphe at the perineum. These swollen cysts spontaneously ruptured and healed; (b) Silent phase: There were two separate lesions; one was a very small cyst on the scrotal median raphe (arrow), and the other was a canal-like lesion lined on the perineal median raphe (arrowhead).

Figure 2. Pathological findings of the lesions (HE staining, 100×). (a) The inner layer of the small cyst was composed of transitional epithelium; (b) The inner layer of the canal-like cysts was also composed of transitional epithelium.
buried under the skin when the urethral folds form the urethra, or 2) the result of abnormal development of paraurethral ducts. The inner layer of the cysts was composed of various epithelia such as stratified squamous epithelium, pseudostratified epithelium and squamous columnar epithelium, which are epithelia of endodermal origin and the components of the male urethra. Indeed, in our case the epithelium of the inner layer of the cysts was composed of transitional epithelium, which also suggested urethral origin. The differential diagnoses of cysts in the perineal area are urethral diverticulum, dermoid cyst, epidermoid cyst [10] and pilonidal cyst, and the diagnosis should be obtained by clinical findings and results of histological analysis of the epithelium of the cysts.
This lesion often shows no symptoms and in such cases observation may be a reasonable choice but once symptoms appear, it must be excised to relieve the symptoms.
We must keep in mind that this lesion is rare but may be encountered in the outpatient clinic and should be treated properly.
![]()
![]()
REFERENCES
- Mermet, P. (1895) Congenital cysts of the genitoperineal raphe. Revue de Chirurgie, 15, 382-435.
- Little, J.S., Keating, M.A. and Rink, R.C. (1992) Median raphe cysts of the genitalia. Journal of Urology, 148, 1872-1873.
- Scelwyn, M. (1996) Median raphe cyst of the perineum presenting as a perineal polyp. Pathology, 28, 201-202. doi:10.1080/00313029600169893
- LeVasseur, M.J.G. and Perry, L.C.V.E. (1997) Perineal median raphe cyst. Pediatric Dermatology, 14, 391-392. doi:10.1111/j.1525-1470.1997.tb00990.x
- Petit, P.R.T. and Pasquier, C.J. (2002) Perineal median raphe canal: A typical image. Urology, 53, 136.
- Park, C.O., Chun, E.Y. and Lee, J.H. (2006) Median raphe cyst on the scrotum and perineum. Journal of the American Academy of Dermatology, 55, S114-S115. doi:10.1016/j.jaad.2005.07.008
- Krauel, L., Tarrado, X., Gracia-Aparicio, L., et al. (2008) Median raphe cysts of the perineum in children. Journal of Pediatric Urology, 71, 830-831.
- Verma, S.B. (2009) Canal-like median raphe cysts: An unusual presentation of an unusual condition. Clinical and Experimental Dermatology, 34, E857-E858. doi:10.1111/j.1365-2230.2009.03604.x
- Navarro, H.P., Lopez, P.C., Ruiz, J.M., et al. (2009) Median raphe cyst. Report of two cases and literature review. Archivos Españoles de Urología, 62, 585-589.
- Takano, Y., Yokokawa, K., Namiki, M., et al. (1994) Perineal epidermal cyst. Urologia Internationalis, 53, 53- 55. doi:10.1159/000282634
NOTES
*All the authors have no conflict of interest.
#Corresponding author.