Health
Vol.4 No.11A(2012), Article ID:24966,5 pages DOI:10.4236/health.2012.431171
Non-motor signs and symptoms in Parkinson’s disease
![]()
Clinical Research Center, Osaka Health Science University, Osaka, Japan; kazuo.abe@ohsu.ac.jp
Received 20 August 2012; revised 26 September 2012; accepted 8 October 2012
Keywords: Parkinson’s Disease (PD); Non-Motor Signs and Symptoms; Activities of Daily Livings (ADL); Quality of Life (QOL)
ABSTRACT
Motor symptoms are cardinal clinical features of Parkinson’s disease (PD). Progress in drug therapy and rehabilitation has been presenting beneficial effect for motor symptoms. However, non-motor symptoms and signs in PD have been accumulated growing attentions and its amelioration may also give beneficial effect for PD patients’ and their care givers’ quality of life. In this mini-review, I overviewed non-motor symptoms and signs in PD.
1. INTRODUCTION
James Parkinson described in his historical essay, “Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported; with a propensity to bend the trunk forwards, and to pass from a walking to a running pace: the senses and intellects being uninjured” [1]. From then, Parkinson’s disease (PD) has been classified as “Movement Disorders” and its clinical diagnosis requires existences of tremor, akinesia, muscle rigidity, and loss of right reflex and has been treated mainly to improve these “motor syndromes” [1-3]. Advent of drug therapy for PD can improve motor function and activities of daily livings (ADL) from their early stages [4-7]. Recently, however, not motor syndrome but non-motor syndrome accumulated attention, because non-motor syndrome such as fatigue, sleep disorders, and dysautonomia closely relate with improvement of their quality of life (QOL) [8-12]. In addition, some researchers consider nonmotor syndrome as an initial signs and symptoms in PD [13].
In this mini-review, I overviewed non-motor symptoms and signs in PD.
2. NON-MOTOR SIGNS AND SYMPTOMS IN PD
Numbers of non-motor symptoms and signs in PD constantly increase with accumulation of information of PD clinical pathogenesis. To investigate non-motor symptoms scale for Parkinson’s disease (NMSSPD), we preliminary investigated overall frequency of non-motor symptoms and signs using questioner sheets [11,12]. We investigate neuropsychological signs (depression, apathy, anxiety, anhedonia, cognitive dysfunction, attention deficit, hallucination, delusion, dementia, delirium, panic disorder), sleep disorders (restless leg syndrome, abnormal behavioral disorders in REM period, insomnia, excessive day time sleep, sleep apnea), dysautonomia (orthostatic hypotension, dysuria, impotent), digestion disorders (drooping, incontinence, dysphagia, dysosmia, visual disorder), behavioral disorder (hypersexuality, compulsive behavior, pathological shopping, pathological gambling), and others (fatigue, weight loss, weight gain) [11-16]. Based on results [14], we found that drooping, dysosmia, dysphagia, incontinence, bowel disorder, forgetfulness, inattention, depression, sleep disorder, and abnormal sweating) in PD were significantly increased comparing with those in controls.
These foregoing investigations indicate that non-motor signs and symptoms in PD have been known to affect their motor syndromes and QOL.
2.1. Neuropsychological Syndromes
PD patients may develop neuropsychiatry syndromes such as hallucination [17,18] or depression [19], which interfere their treatment, care, ADL.
Unless hallucination affects ADL, full explanation to patients and their caregivers may lighten their burdens. If hallucination in PD needs immediate integrative treatment with psychosocial interventions, antipsychotic medication and adjustment of anti-PD medication are prescribed, however leaving an adequate L-dopa dose to prevent severe off-states [20].
For people with PD, depression is quite common. Up to 60 percent of people with PD experience mild or moderate depressive symptoms. Research suggests that PD itself causes chemical changes of dopamine, serotonin, and norepinephrine in the limbic system that may lead to depression. Dopamine and dopamine agonist are used for treatment of depression [20-23]. In addition, depression in PD has close relationship with motor dysfunction. Thus, improvement of motor syndrome is the key factor for improvement of depression in PD.
Anxiety and apathy are dependent syndromes to depression. These signs and symptoms may be found with depression, but may be found without depression unless full drug therapy for motor syndrome conducted [24,25].
James Parkinson firstly described that PD patients never developed dementia. However, we know that PD patients may develop frontal lobe dysfunction such as forgetfulness [26-28]. PD patients have difficulty planning and carrying through tasks. When facing a task or situation on their own, a person with PD may feel overwhelmed by having to make choices. They may also have difficulty remembering information, or have trouble finding the right words when speaking. To some degree, cognitive impairment affects most PD patients. The same chemical changes that lead to motor symptoms can also result in slowness in thinking [28]. Cognitive impairment in PD is different from dementia, which is a more severe loss of intellectual abilities that interferes with daily living so much that it may not be possible for a person to live independently. Causes cognitive changes in PD remain unclear, but a possible cause is a decreased level of dopamine. However, the cognitive changes associated with dopamine declines are typically mild and circumscribed. It should be noted that PD patients have deep stigma that impairs their cognitive function and increases burden of caregivers.
2.2. Sleep Disturbances
Up to 60% of PD patients have been reported to claim sleep disturbances. PD patients may have difficulty turning over in their sleep due to increased muscle tonus, may be ceased their sleep by pollakisuria, or may have depression [29]. Although non-ergotic dopamine agonists are ropinirole, pramipexole, and rotigotine which have been known to induce day time or sudden insomnia [30], PD itself induces sleep disturbances such as restless leg syndrome (RLS), abnormal behavioral disorders in REM period (RBD), insomnia, excessive day time sleep, and sleep apnea [31-35] PD patients are reported to develop RBD at high frequency up to 40% and have considered these sleep disturbances in their early stage. Thus, diagnosis and treatment of sleep disturbances is a key factor for PD treatment [9,29].
2.3. Autonomic Failure (Dysautonomia)
PD patients frequently show dysautonomia such as orthostatic hypotension [36] and bowel disorders [37]. Unlike patients with multiple systemic atrophy (MSA), PD patients rarely lose their consciousness due to orthostatic hypotension. However, light-headedness or dizziness due to orthostatic hypotension may be a risk factor for accidental falls and injuries after falls [3,8,9]. Since PD patients are tended to have disused syndrome that impairs their ADL and QOL, rehabilitation using tilt table and elastic stockings is needed [15,36]. If their environments require, reform of houses is also planned [38-41].
PD patients may show pollakisuria, dysuria, feeling of residual urine, or incontinence of urine. Even the same man may develop a wide variety of urinary disorders. PD patients may have sleep disorders due to nocturia [9,33]. These urinary signs are improved after adequate dopamine therapy, but anticholinergic agent such as oxybutynin hydrochloride can improve these [39,41].
2.4. Digestive Disorders
PD patients frequently develop incontinence without antiparkinsonian agents, but antiparkinsonian agents themselves have some effect on developing incontinence. [42,43] Braak et al. pathologically found Lewy bodies in the Auerbach neural plexus that may be result in incontinence in PD [44]. Incontinence has possibility to result in ileus and should be treated with drugs, diet and exercise [45].
PD patients increasingly show drooping with progression of disease, but patients do not have increased amount of saliva sputum but slowing of swallowing may be a cause [46]. Although some drugs can reduce amount of saliva sputum that increases decayed tooth and periodontal disease, wiping or postural drainage therapy may be useful to prevent aspiration pneumonia.
To treat dysphagia in PD, nutrition support team (NST) may be useful in daily clinic [47,48].
2.5. Sensory Disturbance
James Parkinson described that PD patients never showed sensory disturbances [1], but many of patients may experience pain or dysesthesia [49] PD patients also demonstrate dysosmia [50,51] and dysgeusia [52] in their early sages. Dopamine is an agent to modulate pain in spinal cord, thalamus, basal ganglia and cingulate gyrus. [53,54] Because of dysregulation of dopamine, PD patients show sensory disturbances. Up to 29% of PD patients complain pain that impedes their QOL [11].
2.6. Behavior Disorders
Disinhibition including hypersexuality, compulsive behavior, pathological shopping, and pathological gambling are also reported as behavior disturbances in PD [11,12]. In our study in Japan, we less frequently observed these behavior disturbances and considered this is because in Japan relatively small amount of antiparkinsonian drugs are used. Amantadine may be effective for disinhibition [54].
2.7. Fatigue
Fatigue is the most trouble but less familiar syndrome in PD [55-60]. Fatigue can be distinguished from depression. Depressions in PD have some relation with motor syndrome, but fatigue does not. Depression also troubles patients’ caregivers [57-60]. Although pathogenesis of fatigue in PD remains uncertain, we hypothesize that it may have some relation with cognitive dysfunction, especially frontal lobe dysfunction (Figure 1) [56,61].
2.8. Others
PD patients show respiratory dysfunction which results in speech disturbances, dysphagia, and aspiration pneumonia [62,63]. We develop an exercise for PD including respiratory exercise and could improve respiretory dysfunction (Figure 2).
3. CONCLUSION
Since PD patients are admitted neurological clinic be-
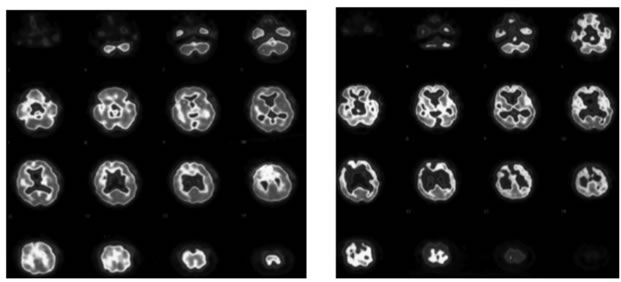
Figure 1. A single emission computed tomographic image using Tc-99m-HMPAO (hexamethyl propylamine oxime, Ceretec™) showed decreased isotope uptakes in the frontal lobe of PD patients with fatigue (right) but not in the frontal lobe of PD patients without fatigue.
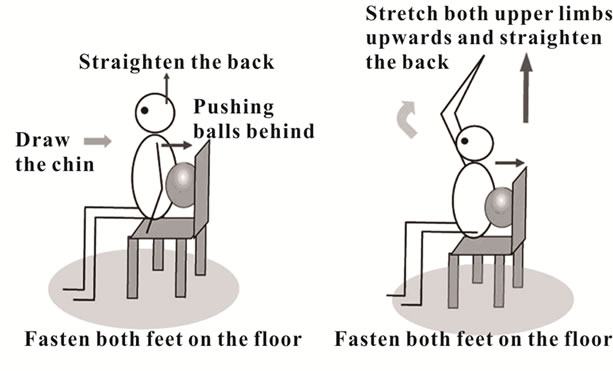
Figure 2. An exemplified exercise program for Parkinson’s disease.
cause of their motor signs and symptoms such as bradykinesia, tremor, or dystonia, we neurologists mainly pay attention to improve these motor syndrome. However, with advent of PD therapy improve, in some extent, motor syndrome, but nonmotor syndrome has increasingly known to be a crucial factor to improve patients’ and their care givers’ QOL [9,14,57,58]. Pathological examinations mainly by Braak et al. hypothesized that nonmotor syndrome might result from initial pathological changes in PD [44]. Validation of this hypothesis is open for discussion, but for their QOL we should pay more attention for nonmotor syndrome in PD.
![]()
![]()
REFERENCES
- Parkinson, J. (2002) An essay on the shaking palsy. The Journal of Neuropsychiatry and Clinical Neurosciences, 14, 223-236. doi:10.1176/appi.neuropsych.14.2.223
- Hoehn, M.M. and Yahr, M.D. (1967) Parkinsonism, onset, progression and mortality. Neurology, 17, 427-442. doi:10.1212/WNL.17.5.427
- Jankovic, J. (2008) Parkinson’s disease, clinical features and diagnosis. Journal of Neurology, Neurosurgery & Psychiatry, 79, 368-376. doi:10.1136/jnnp.2007.131045
- Duvoisin, R.C. and Sage, J. (2001) Parkinson’s disease. A guide for patient and family. 5th Edition, Lippincott Williams & Wilkins, Philadelphia, New York.
- Abe, K. (2002) Frontier in treatment. Parkinson disease— Role of rehabilitation. Brain Medicine, 14, 45-54.
- Coelho, M. and Ferreira, J.J. (2012) Late-stage Parkinson disease. Nature Reviews Neurology, 8, 435-442.
- Schenkman, M., Hall, D.A., Baron, A.E., Schwartz, R.S., Mettler, P. and Kohrt, W.M. (2012) Exercise for people in earlyor mid-stage Parkinson disease, a 16-month randomized controlled trial. Physical Therapy, 92, 1395-1410. doi:10.2522/ptj.20110472
- Gräber, S., Liepelt-Scarfone, I., Brüssel, T., Schweitzer, K., Gasser, T. and Berg, D. (2011) Self estimated quality of life in monogenetic Parkinson’s disease. Movement Disorders, 26, 187-188. doi:10.1002/mds.23209
- Chaudhuri, K.R., Healy, D.G. and Schapira, A.H.V. (2009) Non-motor symptoms of Parkinson’s disease, diagnosis and management. Lancet Neurology, 8, 464-474. doi:10.1016/S1474-4422(09)70068-7
- Abe, K., Takanashi, M. and Yanagihara, T. (2000) Fatigue in patients with Parkinson’s disease. Behavioural Neurology, 12, 103-106.
- Martinez-Martin, P., Schapira, A.H.V. and Stocchi, F. (2007) Prevalence of nonmotor symptoms in Parkinson's disease in an international setting study using nonmotor symptoms questionnaire in 545 patients. Movement Disorders, 22, 1623-1629. doi:10.1002/mds.21586
- Chaudhuri, K.R., Martinez-Martin, P., Brown, R.G., Sethi, K., Stocchi, F., Odin, P., Ondo, W., Abe, K., MacPhee, G., MacMahon, D., Barone, P., Rabey, M., Bonnuccelli, U., Forbes, A., Breen, K., Tluk, S., Naidu, Y., Olanow, C.W., Thomas, S., Rye, D., Bowron, A., Williams, A.J. and Schapira, A.H.V. (2007) The metric properties of a novel non-motor symptoms scale for Parkinson’s disease, results from an international pilot study. Movement Disorders, 22, 1901-1911. doi:10.1002/mds.21596
- Zanigni, S., Calandra-Buonaura, G., Grimaldi, D. and Cortelli, P. (2011) REM behaviour disorder and neurodegenerative diseases. Sleep Medicine, 12, S54-S58. doi:10.1016/j.sleep.2011.10.012
- Martinez-Martin, P., Rodriguez-Blazquez, C., Abe, K., Bhattacharyya, K.B., Bloem, B.R., Carod-Artal, J., Dill, B., Esselink, R., Falup-Pecurariu, C., Gallardo, M,. Mir, P., Naidu, Y., Nicoletti, A,. Sethi, K., Tsuboi, Y., van Hilten, J.J., Visser, M., Zappia, M. and Chaudhuri, K.R. (2009) International validation of the non-motor symptoms scale, comparison with the pilot study. Neurology, 73, 1584-1591. doi:10.1212/WNL.0b013e3181c0d416
- Martinez-Martin, P., Rodriguez-Blazquez, C., BKurtis, M.M., Chaudhuri, K.R. and The NMSS Validation Group (2011) The impact of non motor symptoms on health-related quality of life of patients with Parkinson’s Disease. Movement Disorders, 26, 399-406. doi:10.1002/mds.23462
- Hoehn, M.M. and Yahr, M.D. (1967) Parkinsonism, onset, progression and mortality. Neurology, 17, 427-442. doi:10.1212/WNL.17.5.427
- Fénelon, G., Mahieux, F. and Huon, R. (2000) Hallucinations in Parkinson’s Disease. Prevelance, phenomenology and risk factors. Brain, 123, 733-745. doi:10.1093/brain/123.4.733
- Jenner, J. and Laar van, T. (2012) Visual hallucinations in Parkinson’s disease. In: Stone, J.H. and Blouin, M., Eds., International Encyclopedia of Rehabilitation. http://cirrie.buffalo.edu/encyclopedia/en/article/147/
- Cummings, J.L. and Masterman, D.L. (1999) Depression in patients with Parkinson’s disease. International Journal of Geriatric Psychiatry, 14, 711-718. doi:10.1002/(SICI)1099-1166(199909)14:9<711::AID-GPS4>3.0.CO;2-1
- Remy, P., Doder, M. and Lees, A. (2005) Depression in Parkinson’s disease. Loss of dopamine and noradrenaline innervations in the limbic system. Brain, 128, 1314-1322. doi:10.1093/brain/awh445
- Rektorova, I., Rektor, I. and Bares, M. (2003) Pramipexole and pergolide in the treatment of depression in Parkinson’s disease, a national multicentre prospective randomized study. European Journal of Neurology, 10, 399- 406. doi:10.1046/j.1468-1331.2003.00612.x
- Barone, P., Scarzella, L. and Marconi, R. (2006) Pramipexole versus sertraline in the treatment of depression in Parkinson’s disease. A national multicenter parallel group randomized study. Journal of Neurology, 253, 601-607. doi:10.1007/s00415-006-0067-5
- Lemke, M.R., Brecht, H.M. and Koester, J. (2005) Anhedonia, depression and motor functioning in Parkinson’s disease during treatment with pramipexole. The Journal of Neuropsychiatry and Clinical Neurosciences, 17, 214- 220. doi:10.1176/appi.neuropsych.17.2.214
- Czernecki, V., Pillon, B. and Houeto, J.L. (2002) Motivation, reward and Parkinson’s disease, influence of dopa therapy. Neuropsychologia, 40, 2257-2267. doi:10.1016/S0028-3932(02)00108-2
- Aarsland, D., Andersen, K., Larsen, J.P., Lolk, A. and Kragh-Sørensen, P. (2003) Prevalence and characteristics of dementia in Parkinson disease. Archives of Neurology, 60, 387-392. doi:10.1001/archneur.60.3.387
- Williams-Gray, C.H., Foltynie, T. and Brayne, C.E.G. (2007) Evolution of cognitive dysfunction in an incident Parkinson’s disease cohort. Brain, 130, 1787-1798. doi:10.1093/brain/awm111
- Cooper, J.A., Sagar, H.J. and Jordan, N. (1991) Cognitive impairment in early, untreated Parkinson’s disease and its relationship to motor disability. Brain, 114, 2095-2122. doi:10.1093/brain/114.5.2095
- Fujiwara, M., Yamauchi, K. and Abe, K. (2007) Rehabilitation in Parkinson disease. Monthly Book Medical Rehabilitation, 76, 44-52.
- Chaudhuri, K.R., Pal, S. and DiMarco, A. (2002) The Parkinson’s disease sleep scale, a new instrument for assessing sleep and nocturnal disability in Parkinson’s disease. Journal of Neurology, Neurosurgery & Psychiatry, 73, 629-635. doi:10.1136/jnnp.73.6.629
- Homann, C.N., Wenzel, K., Suppan, K., Ivanic, G., Kriechbaum, N., Crevenna, R. and Ott, E. (2002) Sleep attacks in patients taking dopamine agonists, review. BMJ, 324, 1483-1487. doi:10.1136/bmj.324.7352.1483
- Diagnostic Classification Steering Committee (1990) International classification of sleep disorders, diagnostic and coding manual. American Sleep Disorders Association, Rochester.
- Abe, K., Hikita, T. and Sakoda, S. (2005) Sleep disturbances in Japanese patients with Parkinson’s diseaseComparing with patients in the UK. Journal of Neurol Science, 234, 73-78. doi:10.1016/j.jns.2005.03.036
- Abe, K., Hikita, T. and Sakoda, S. (2005) Zolpidem tartrate therapy for sleep disturbances in patients with Parkinson’s disease. Journal of the Neurological Sciences, 238, S350. doi:10.1016/S0022-510X(05)81350-4
- Goetz, C.G., Ouyang, B., Negron, A. and Stebbins, G.T. (2010) Hallucinations and sleep disorders in PD, ten-year prospective longitudinal study. Neurology, 75, 1773-1779. doi:10.1212/WNL.0b013e3181fd6158
- Abe, K. (2008) Zolpidem therapy for movement disorders. Recent Patents on CNS Drug Discovery, 3, 55-60. doi:10.2174/157488908783421519
- Medow, M.S., Stewart, J.M., Sanyal, S., Mumtaz, A., Sica, D. and Frishman, W.H. (2008) Pathophysiology, diagnosis, and treatment of orthostatic hypotension and vasovagal syncope. Cardiology in Review, 16, 4-20.
- Fitzmaurice, H., Fowler, C.J, Rickards, D., Kirby, R.S., Quinn, N.P., Marsden, C.D., Milroy, E.J. and TurnerWarwick, R.T. (1985) Micturition disturbance in Parkinson’s disease. British Journal of Urology, 57, 652-656. doi:10.1111/j.1464-410X.1985.tb07025.x
- Duncan, R.P., Leddy, A.L., Cavanaugh, J.T., Dibble, L.E., Ellis, T.D., Ford, M.P., Foreman, K.B. and Earhart, G.M. (2012) Accuracy of fall prediction in Parkinson disease, six-month and 12-month prospective analyses. Parkinson’s Disease, 237673.
- Clarke, C.E., Zobkiw, R.M. and Gullaksen, E. (1995) Quality of life and care in Parkinson’s disease. British Journal of Clinical Practice, 49, 288-293.
- Kamata, N. and Abe, K. (2008) Accidental falls and overestimation of stability limits in Parkinsonian patients. In: Murray, C.A., Ed., Accidental Falls, Causes, Prevention, and Interventions, Nova Science Publishers and Inc., New York, 200-243.
- Jain, S. and Goldstein, D.S. (2012) Cardiovascular dysautonomia in Parkinson disease, from pathophysiology to pathogenesis. Neurobiology of Disease, 46, 572-580. doi:10.1016/j.nbd.2011.10.025
- Singharam, C., Ashraf, W. and Gaummitz, E.A. (1995) Dopaminergic defect of enteric nervous system in Parkinson’s disease patients with chronic constipation. Lancet, 346, 861-864. doi:10.1016/S0140-6736(95)92707-7
- Abbott, R.D., Petrovitch, H. and White, L.R. (2001) Frequency of bowel movements and the future risk of Parkinson’s disease. Neurology, 57, 456-462. doi:10.1212/WNL.57.3.456
- Braak, H., Del Tredici, K., Rüb, U., de Vos, R.A., JansenSteur, E.N. and Braak, E. (2003) Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiology of Aging, 24, 197-211. doi:10.1016/S0197-4580(02)00065-9
- Clark, E.C., Mulder, D.W., Erickson, D.J., Clements, B.G. and Maccaty, C.S. (1957) Parkinson’s disease, therapeutic exercises in its management. Postgraduate Medicine, 21, 301-308.
- Kalf, J.G., de Swart, B.J., Borm, G.F., Bloem, B.R. and Munneke, M. (2009) Prevalence and definition of drooling in Parkinson’s disease, a systematic review. Journal of Neurology, 256, 1391-1396. doi:10.1007/s00415-009-5098-2
- Salat-Foix, D. and Suchowersky, O. (2012) The management of gastrointestinal symptoms in Parkinson’s disease. Expert Review of Neurotherapeutics, 12, 239-248. doi:10.1586/ern.11.192
- Lyons, K.E. and Pahwa, R. (2011) The impact and management of nonmotor symptoms of Parkinson’s disease. American Journal of Managed Care, 17, S308-S314.
- Quinn, N.P., Koller, W.C., Lang, A.E. and Marsden, C.D. (1986) Painful Parkinson’s disease. Lancet II, 1366-1369. doi:10.1016/S0140-6736(86)91674-0
- Shah, M., Deeb, J., Fernando, M., Noyce, A., Visentin, E., Findley, L.J. and Hawkes, C.H. (2009) Abnormality of taste and smell in Parkinson’s disease. Parkinsonism and Related Disorders, 15, 232-237. doi:10.1016/j.parkreldis.2008.05.008
- Landis, B.N. and Burkhard, P.R. (2008) Rhinorrhea and olfaction in Parkinson disease. Neurology, 71, 1041-1042. doi:10.1212/01.wnl.0000327867.15757.d0
- Chudler, E.H. and Dong, W.K. (1950) The role of the basal ganglia in nociception and pain. Pain, 60, 3-38. doi:10.1016/0304-3959(94)00172-B
- Shyu, B.C., Kititsy-Roy, J.A. and Morrow, T.J. (1992) Neurophysiological, pharmacological and behavioural evidence for medial thalamic mediation of cocaine induced dopaminergic analgesia. Brain Research, 522, 216-223. doi:10.1016/0006-8993(92)90472-L
- Weintraub, D., Sohr, M., Potenza, M.N., Siderowf, A.D., Stacy, M., Voon, V., Whetteckey, J., Wunderlich, G.R. and Lang, A.E. (2010) Amantadine use associated with impulse control disorders in Parkinson disease in cross-sectional study. Annals of Neurology, 68, 963-968. doi:10.1002/ana.22164
- Abe, K. (2006) Tiredness and fatigue. Journal of International Society of Life Information Science, 24, 60-62.
- Abe, K. (2001) Tiredness and fatigue. Brain, 21, 35-39.
- Abe, K., Takanashi, M., Yanagihara, T. and Sakoda, S. (2002) Pergolide mesilate may improve fatigue in patients with Parkinson’s disease. Behavioural Neurology, 13, 117- 121.
- Schrag, A., Jahanshahi, M. and Quinn, N. (2000) What contributes to quality of life in patients with Parkinson’s disease? Journal of Neurology Neurosurgery & Psychiatry, 69, 308-312. doi:10.1136/jnnp.69.3.308
- Martinez-Martine, P., Benito-León, J., Alonso, F., Catalán, M.J., Pondal, M., Zamarbide, I., Tobías, A., de Pedro, J. Quality of life of caregivers in Parkinson’s disease. Quality of Life Research, 14, 463-472. doi:10.1007/s11136-004-6253-y
- [61] Krupp, L.B., Coyle, P.K. and Doscher, C. (1995) Fatigue therapy in multiple svlerosis—Results of a double-blind, randomized, parallel trial of amantadine, remoline, and placebo. Neurology, 45, 1956-1961. doi:10.1212/WNL.45.11.1956
- [62] Pavese, N., Metta, V,. Bose, S.K., Chaudhuri, K.R. and Brooks, D.J. (2010) Fatigue in Parkinson’s disease is linked to striatal and limbic serotonergic dysfunction. Brain, 33, 3434-3443. doi:10.1093/brain/awq268
- [63] Tamaki, A., Matsuo, Y. and Abe, K. (2000) Influence of Thoracoabdominal movement on pulmonary function in patients with Parkinson’s disease. Comparison with healthy subjects. Neurorehabilitation and Neural Repair, 14, 43- 47. doi:10.1177/154596830001400105
- [64] Matsuo, Y., Kamata, N. and Abe, K. (2006) Thoracoabnominal movements during deep breathing in patients with Parkinson’s disease may be reduced parallel to disease progression. Clinical Neurophysiology, 117, S185. doi:10.1016/j.clinph.2006.06.334