Health
Vol. 4 No. 10 (2012) , Article ID: 24066 , 4 pages DOI:10.4236/health.2012.410121
Addressing the health needs of South Asians: The community perspective
![]()
Department of Prevention and Community Health, School of Public Health and Health Services, The George Washington University, Washington DC, USA; *Corresponding Author: nitasha@gwu.edu
Received 17 August 2012; revised 15 September 2012; accepted 26 September 2012
Keywords: Community Health; Health Education; Minority Health; Community Based Organizations; South Asian American Health; Community Perspective
ABSTRACT
Community based organizations play a vital role in the health of communities in the United States, particularly among immigrant and minority populations. Yet the gap between the needs of the community and the health issues that are being addressed remains quite large. This qualitative assessment provides a brief summary of community-based organizations in the US that focus on health issues specifically addressing the needs of south Asian Americans. In addition, this assessment explores the health needs of the South Asian American community living in the Washington DC metropolitan region, the fifth largest densely populated city in the US of South Asian Americans. While the report provides an array of organizations serving this population, the question of how effective can community-based organizations be if they can not prioritize their needs based on the community’s needs still remains.
1. INTRODUCTION
The south Asian community in the United States (US) includes ancestry from Afghanistan, Bangladesh, Bhutan, India, The Maldives, Nepal, Pakistan, and Sri Lanka [1]. In addition, the community includes members of the South Asian Diaspora, including past generations of South Asians who originally settled in the many areas of the world: the Caribbean (Guyana, Jamaica, Suriname, and Trinidad and Tobago); Africa (Nigeria, South Africa, and Uganda); Canada; Europe; and other parts of Asia and the Pacific Islands (Fiji, Indonesia, Malaysia, and Singapore) [2]. Today there are approximately 2.7 million South Asians living in the US and the total population of the US, increased by 13.2% from 1990 to 2000, while the Asian American population has increased by 72% [3]. The five largest groups of South Asian communities in the US include Indians, Pakistanis, Bangladeshis, Sri Lankans and Nepalis, respectively [4].
Washington DC, the fifth largest population of South Asians in the US, has seen a steady increase in persons of South Asian origin. Between 2000 and 2007, the DC, metropolitan area has seen an increase of 25% in Asian Americans [5]. South Asians of Indian descent are amongst the highest (57.4%), and in smaller proportions Pakistani, Bangladeshi, Nepali, and Sri Lankan [5]. South Asians in this region reside in parts of DC, Maryland and Virginia, and more than half are naturalized American citizens. Forty-one percent of South Asians in the Washington DC metropolitan area earn incomes of more than $100,000, while about 11% have incomes of less than $29,000 despite high levels of educational attainment from their home country [5].
South Asian Americans have generally been viewed as an exceptionally successful immigrant group and have been perceived to be “wealthy and healthy”, resulting in the characterization of the “model minority” community. This misperception and characterization of the “Model Minority” myth has led to neglect of major health and social concerns, and resources. In addition, the reality that South Asian Americans are living under the poverty line, do not have access to care, and have limited English proficiency are overlooked. The “model minority” myth has resulted in less funding for programs and research. Further, is the lack of disaggregated data, which has frustrated attempts of community leaders and researchers to study this population’s health and well-being.
2. IMPORTANCE OF COMMUNITY BASED ORGANIZATIONS
Community based organizations (CBOs) are charged with the mission to involve community members, organizational representatives, and researchers in all aspects to enhance understanding of a given phenomenon and integrate the knowledge gained with action to benefit the community involved. This process involves research; practice; examination of culture, lifestyle, behavior and environment; and understanding major challenges and implications of facilitating change [6].
These organizations play a vital role in strengthening and empowering communities. Over the last decade there has been a surge of CBOs focused on the South Asian community in the US. A recent study, Community Based Organizations Addressing South Asian American Health, focused on understanding how CBOs throughout the US have begun to address the health of South Asian Americans. Through this exploratory effort, it was illustrated that CBOs are a mechanism for positively addressing the health and well being of South Asians. This study looked at: 1) Organization structure; 2) Funding resources; 3) Types of services; 4) Outreach Strategies; 5) Success and Challenges of the CBO and 6) Recommendations [7,8]. Moreover, organizational leaders provided a summary of what specific health issues are they found to be critical in their communities.
Leaders of these organizations identified a myriad of activities they focus on. In many cases, organizations provide activities for community members to promote a healthy lifestyle (i.e., HIV testing, blood pressure screenings, educational materials). Figure 1 below illustrates the panoply of health topics/services that were offered at CBOs across the nation.
Interestingly enough, when leaders were asked what health issues warrant the most attention amongst the South Asian American population, leaders identified high blood pressure, diabetes and obesity—programs that were being offered at less than 40% of the sites [7]. Although, they did specifically state the degree to which CBOs assist in these additional programs, multiple organizational leaders indicated the need to address these concerns as they are barriers for low-income families in understanding and overcoming mortality.
As it became more and more evident that the needs of the community needed a better understanding, it was
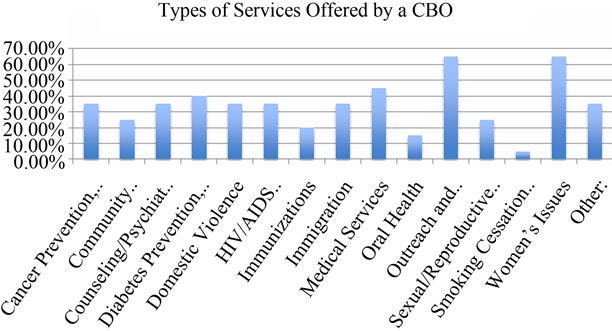
Figure 1. Types of services offered by a CBO.
equally critical to understand the needs and health priorities as seen from the community members. Project SAHNA, or the South Asian Health Needs Assessment, was subsequently conducted to identify perceptions of health needs from individual community members. The study specifically examined the health needs of South Asian American living in the Washington DC metropolitan area. Through this effort, over 700 South Asians living in the Washington DC region were recruited to participate in a self-administered anonymous survey online and in-person. Information was collected on: 1) Attitudes/Perceptions on health status; 2) Physical activity and nutrition habits; 3) Health status; 4) Health care access; 5) Social support; 6) Acculturation; and 7) Demographic information.
Not surprisingly, the study found that community members were consistent with CBO leaders from the previous study and ranked heart disease, blood pressure and diabetes as most important amongst all health issues. As shown in Table 1, Heart Disease (mean = 4.59); Blood pressure (mean = 4.58); Cholesterol (mean = 4.56); and Diabetes (mean = 4.53) had the highest overall mean scores representing “very important” health issues in the community. Furthermore, the means scores did not vary significantly by gender or socio-economic status, adding to the importance of these health issues across groups of South Asian Americans.
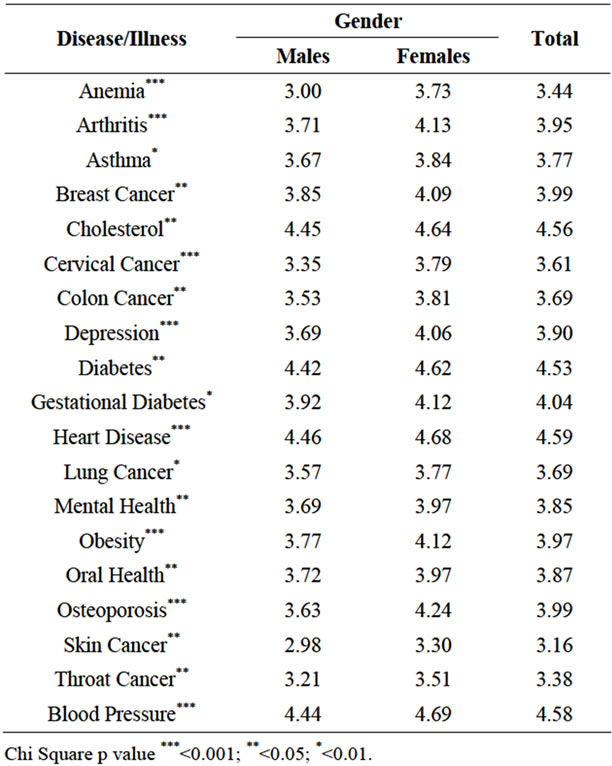
Table 1. Important health risks in the south Asian community (overall means by gender).
While it has been found that cardiovascular disease, diabetes, and cancer are the most commonly cited health concerns among South Asian immigrants, data from this same study found that most Asian American communities perceive a variety of lifestyle factors that increase the risk for these chronic diseases. These lifestyle factors include high stress, lack of physical exercise, and inadequate diet [9]. This was further validated in the findings from the SAHNA report. Only 29.1% of South Asians living in the Washington, DC metropolitan area reported engaging in physical activity four to six times a week for 30 minutes, while 28% reported that they rarely participate in physical activity [8].
So then why the gap between the services being offered by CBOs and the needs and priorities of the community? Historically, CBOs were developed for the South Asian American population due to the discerning rise of domestic violence. However, in the past two decades the nature of health priorities has changed within this population. With cardiovascular disease and Type II diabetes on the rise, it is critical for CBOs to adapt to these growing and significant health needs and priorities.
In light of the growing landscape of CBOs that address health issues, organizations must take into account cultural, spiritual and psycho-social factors that influence these health issues. The majority of health studies, including Project SAHNA and Community Based Organizations Addressing South Asian American Health, highlight how culture and social factors, acculturation, immigration and gender affect diabetes, heart disease, and cancer, among many others. Further, a recent poll conducted by Greenberg Quinlan Rosner Research and Public Opinion Strategies from May 7 to 12, 2009 for the Trust for America’s Health and the Robert Wood Johnson Foundation indicated that “three-quarters of Americans believe the country should invest more in keeping people healthier, and by a nearly four-to-one ratio, they support putting more emphasis on preventing disease rather than treating people after they become sick” [10].
In addition, a number of challenges exist with CBOs— funding being one of the largest. Due to the heterogeneity nature of the population, CBOs spend a lot of time and effort translating materials into various languages, overcoming cultural barriers, and reducing social stigma. These efforts, although extremely critical for this population, take a lot of time and resources away from direct service programs that can be offered. Lastly, the South Asian population in the US continues to be characterized as a “model minority” and this perception has led to a neglect of health concerns, resulting in less funding for programs and research for this ethnic population.
3. RECOMMENDATION FOR ACTION
CBOs play an active role in research and practice of health and wellness programs, and can influence the community through preventive services. Given this notion, CBOs can implement the following recommendations to further expand their mission to accommodate the needs of the community.
• It is essential CBOs to examine the gender roles, nutrition and dietary practices, lifestyle and cultural practices and how these factors influence health. Given the risks of type II diabetes and cardiovascular disease in this community, future research efforts should further explore the relationship of these factors to better understand why the South Asian population is genetically and environmentally more likely inclined certain chronic diseases.
• It is imperative that community based organizations collaborate with one another. Previous studies have found that coalition building and collaboration results in increased education of health programs, preventative programs, and trust within the community. Further solidifying partnerships has resulted in costsharing and resource sharing.
• There is a need to challenge CBOs and community leaders to better understand the community they are serving. This is a growing and diverse community and therefore, health needs and priorities have evolved over time and will continue to do so. It is only makes sense to continually have CBO leaders reach out to the community members understand their concerns and help alleviate the various issues.
By implementing these recommendations, not only will the level of awareness of health issues be raised, there will also be a change of attitude, lifestyle and behavior within this minority group. Benefits in understanding and implementing these initiatives allows for CBOs to be an integral asset in understanding and empowering communities through education and health promotion.
REFERENCES
- BBC World News (2012) Country profile website. http://news.bbc.co.uk/1/hi/world/south_asia/country_profiles/1154019.stm
- South Asian Americans Leading Together (SAALT) (2007) Building community strength: A report about community-based organizations serving south Asians in the United States.
- US Census Bureau (2010) The Asian population: 2000. http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf
- SAALT (2010) About the south Asian community. http://www.saalt.org/pages/About-the-South-Asian-Community.html
- South Asian Americans Leading Together (SAALT) (2009) Washington DeSI: South Asians in the Nation’s capital. Takoma Park.
- Gailbraith, M. (2011) Community based organizations and the delivery of lifelong learning opportunities. Florida Atlantic University, Boca Raton. http://www.ed.gov/pubs/PLLIConf95/comm.html
- Chaudhary, N., Vyas, A. and Parrish, B. (2010) Community based organizations addressing south Asian American health. Journal of Community Health, 35, 384-391. doi:10.1007/s10900-010-9256-3
- Vyas, A., Chaudhary, N., Ramiah, K. and Abbasi, S. (2010) SAHNA 2010: A south Asian health needs assessment of the Washington DC Region. http://sphhs.gwumc.edu/staticfile/SPHHS/SAHNA%202010.pdf
- Joshi, P., Islam, S., Pais, P., et al. (2007) Risk factor for early myocardial infraction in south Asians compared with individuals in other countries. Journal of American Medical Association, 297, 286-294. doi:10.1001/jama.297.3.286
- Trust for America’s Health & the Robert Wood Johnson Foundation (2010) Americans rank prevention as most important health reform priority. http://healthyamericans.org/pages/?id=265