Advances in Sexual Medicine
Vol.3 No.3A(2013), Article ID:34958,9 pages DOI:10.4236/asm.2013.33A002
Testosterone and Its Analogs as a Male Contraceptive
Centre for Advanced Studies, Department of Zoology, University of Rajasthan, Jaipur, India
Email: *lohiyank@hotmail.com; *lohiyank@gmail.com
Copyright © 2013 Abdul S. Ansari et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received May 14, 2013; revised June 14, 2013; accepted June 22, 2013
Keywords: Hormonal Contraception; Suppression of Spermatogenesis; Testosterone; Androgen-Progestin Combination
ABSTRACT
Male contraception by means of hormonal approach was initiated more than 60 years ago when men became azoospermic with administration of testosterone. The basic principle of male hormonal contraception is suppression of spermatogenesis. Exogenous testosterone/testosterone analogs alone or in combination with progestin have been tested for contraceptive efficacy by inhibiting gonadotropins release from pituitary gland. In this review article, advancement in different testosterone preparation tested alone or in combination for contraceptive efficacy has been focused. Administration of testosterone or testosterone analogs alone failed to provide uniform azoospermia or severe oligospermia (<1 million/ml sperm count) at lower doses regimens whereas higher doses causes side effects. Newer, androgen-progestin combination has proved better contraceptive efficacy than testosterone alone. Further, long term studies with hormonal regimens and other alternative approaches are required with fewer side effects for development of safe and reversible contraceptive.
1. Introduction
Contraception is considered as a main key in controlling increasing population growth. Today, much of our current population growth is unintended. Approximately half of unplanned and unintended pregnancies are due to contraceptive failure, largely owing to inconsistent or incorrect use [1,2]. Men in most countries have shown their willingness, ready to share the benefits and burden of family planning. A contraceptive with cent percent sterility and reversibility is the desire of the community. At present, two methods for male contraception are available (1) condoms and (2) vasectomy. However, both suffer limitation in compliance (condoms) and reversibility (vasectomy). Hormonal approach to contraception was established more than 60 years ago when men became azoospermic with administration of testosterone [3,4]. The main principle of male hormonal contraception is to suppress spermatogenesis by means of diminishing the luteinizing hormone (LH) and follicular stimulating hormone (FSH) production in pituitary gland. The FSH and LH production is under the control of hypothalamic regions and intratesticular testosterone act as inducer and inhibitor (through feedback mechanism) [5]. It has been reported that LH pulse is suppressed more when exogenous testosterone was administered [6]. FSH acts directly on Sertoli cells whereas LH exerts its effect through Leydig cells and plays a role in synthesis of interstitial testosterone levels. Decrease in interstitial testosterone along with suppression of FSH results in alternation in Sertoli cell function required for germ cell maturation [7]. According to Weimer manifesto, goal of an effective male hormonal contraceptive method is to provide azoospermia or at least severe oligospermia (<1 million/ml sperm count) [8]. Several male hormonal preparations such as testosterone enanthate (TE), testosterone undecanoate (TU), etc. have been tested at various regimens for contraceptive efficacy. Administration of TE regimen (200 mg TE i.m. weekly for 3 months followed by every 3rd week for 9 months) leads to azoospermia or severe oligospermia in two-third of the tested population [9]. Of these, a number of testosterone preparations have provided alteration in serum levels/unfavorable pharmacokinetic profile and lead to development of new androgen progestin formulations that have paved the way for developing future male hormonal contraception with a regime of safety, efficacy and reversibility. In the present review, recent advances in male hormonal contraception have been discussed with emphasis on the contraceptive efficacy of testosterone and testosterone analogs.
2. Hormonal Regulation of Spermatogenesis
The process of spermatogenesis is under the control of hypothalamo-hypophysial-gonadal axis. Biosynthesis as well as the secretion of FSH and LH from the anterior pituitary gland is regulated by gonadotropins releasing hormones (GnRH) produced from the hypothalamus. [5, 10]. FSH acts directly on Sertoli cells, whereas LH regulates the testosterone synthesis through Leydig cells. LH stimulates the Leydig cells to secrete testosterone. Testosterone diffuses from the testicular interstitial space through the basement membrane and into the seminiferous tubules, where it enters the Sertoli cells. In Sertoli cells, testosterone is converted to dihydrotestosterone (DHT). Testosterone and DHT both leaves the Sertoli cells and gets accumulated around the germ cells. Both FSH and intratesticular testosterone, synergistically play a crucial role in normal spermatogenesis (Figure 1). Interstitial testosterone through feedback mechanism regulates FSH and LH secretion by influencing GnRH release from hypothalamus [5]. Exogenous testosterone administration inhibits gonadotropic secretion through feedback mechanism and parallely blocks both exocrine and endocrine testicular function (i.e. sperm production and testosterone production) [6]. Orchidectomized men exhibit abnormally high levels of FSH and LH in their blood suggesting that testicular substances have negative feedback effect on gonadotropins secretion from adeno-hypophysis [11]. Under normal condition, when testosterone levels drops, LH levels rise and stimulates the Leydig cells to secrete more testosterone. Opposite action occurs when testosterone level rises. In the light of this mechanism, several anti-gonadotropic agents (androgens, progestins etc.) have been used for therapeutic approaches in sexual disorders such as hypogonadism and development of contraceptive dose, etc. [3,4,12-15].
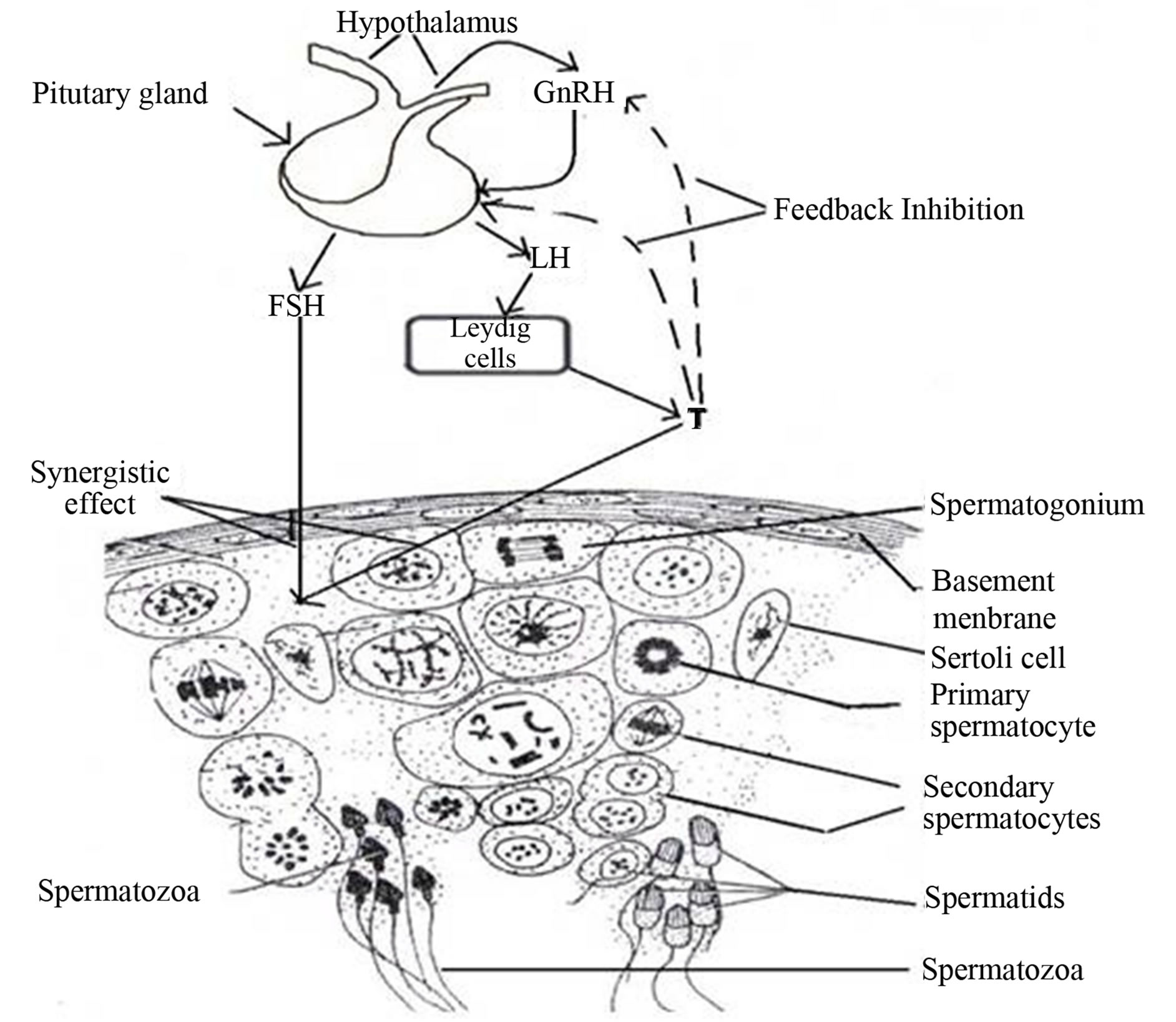
Figure 1. Hormonal regulation of spermatogenesis.
3. Testosterone Analogs as Contraceptive Agents
In the last sixty years, several testosterone and its analog preparations alone or in combination have been tested for contraceptive efficacy, while some of them are currently under clinical trials in combination with other agents have been described below.
3.1. Testosterone Enanthate
Testosterone enanthate (TE) is an ester of testosterone (Figure 2) and was earlier used for the treatment of hypogonadism [12]. Several studies on rats, rabbits and preclinical trials have suggested the potential use of TE as long lasting contraceptive without producing significant side effects [16-18]. Administration of testosterone enanthate (2 mg/kg b.wt/15 day; i.m.) was able to induce azoospermia in 4 out of 5 langur monkeys with mild side effects and recovery after 75 - 90 days of discontinuation of treatment [19]. In 1979, the intramuscular preparation of esterified TE was tested which has shown potential for male contraception [9]. However, the 200 mg TE i.m. weekly for 3 months followed by every 3rd week for 9 months regimen failed to achieve cent percent azoospermia in one third of the tested population. Based on above finding, an efficacy trial with 200 mg TE was initiated by WHO involving healthy fertile subjects at 10 centers in four continents. About 60% of men became azoospermic while remaining reached to severe oligospermia (<3 million count/ml) [20]. The efficacy of this study was high due to inclusion of only men who became azoospermic. Seeing shortcoming of this study a second world wide WHO trial was conducted on 357 couples [21]. The pregnancy rate was 0% as compared to 0.8% in azoospermic men in the first trial. The combined pregnancy rate in both studies was 1.4 pregnancies per 100 person/ year [20,21]. Both WHO trials have demonstrated that hormonal suppression of spermatogenesis may be effective contraception method for men. However, weekly intramuscular injection, side effects and short acting testosterone preparations are few drawbacks that would affect acceptability of this approach for long-term contraceptive use.
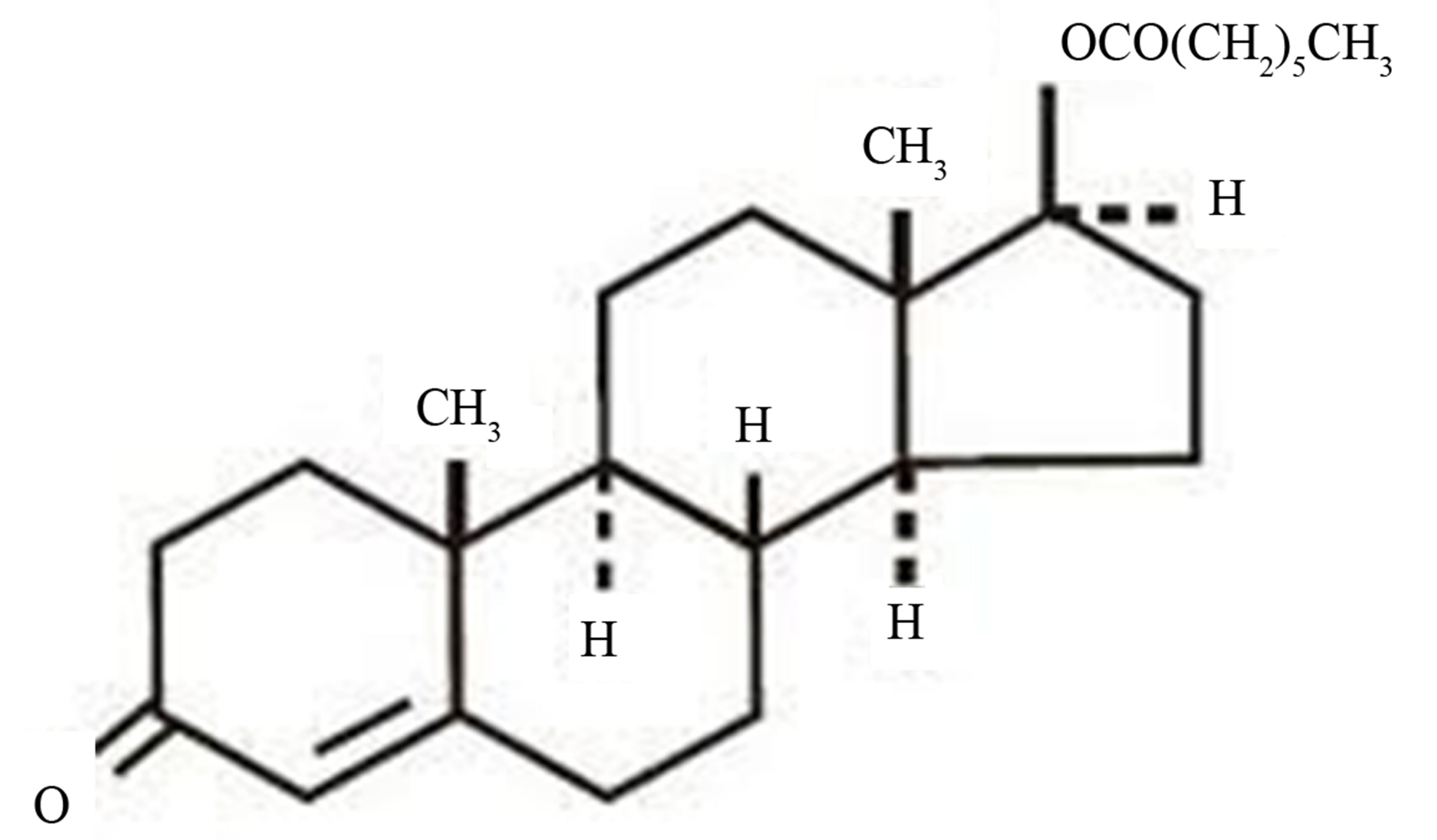
Figure 2. Chemical structure of testosterone enanthate.
3.2. Testosterone Undecanoate
To overcome weekly administration of TE, another testosterone ester, viz., testosterone undecanoate (TU) was tested. TU has long aliphatic-hydrophobic fatty acid side chain which renders its high fat solubility (Figure 3). It is available in both oral and injectable preparations. However, injectable testosterone showed promising results compared to oral preparation. Its two formulations namely TU in tea seed oil (125 mg/ml) in China and TU in castor oil (NebidoTM 250 mg/ml) in Germany showed long acting effect on monthly intramuscular injections. In China, TU (500 mg/ml monthly; i.m.) was able to induce azoospermia or oligospermia (<3 million/ml) in 97% of Chinese subjects with high contraceptive efficacy. However, reappearance of sperm occurred in six men during the efficacy and one pregnancy was attributed to sperm rebound [13]. Another study conducted in China with TU, with a loading dose of 1000 mg followed by 500 mg TU monthly injection. In this phase III study, a total of 1045 men were enrolled around 10 centers in China and 898 couples entered the efficacy phase without using other contraception method efficacy rate was 1.1 per 100 person/year. These studies provide the proof of safe, effective and reversible contraceptive potential with monthly injection of TU. A new and more concentrated formulation of TU in soybean oil (250 mg/ml) is under consideration for clinical trials [22].
3.3. Other Testosterone Preparations
Repeated intramuscular injections limited the participation of more men in clinical trials due to painful procedure. Men have shown their willingness to participate if different mode of delivery is available in the market [23]. To increase the acceptability and make the procedure less painful, following alternative delivery systems were investigated.
3.3.1. Testosterone Pellets
Testosterone pellets were used for treatment of hypogonadism and have also been tested for contraceptive efficacy through surgical insertion into subcutaneous tissue of abdominal wall (Figure 4). A single implantation of 1200 mg (six pellets) testosterone pellets was able to

Figure 3. Chemical structure of testosterone undecanoate.
induce as well as maintain oligospermia-azoospermia for 16 weeks [24]. Testosterone pellets in combination with etonorgestrol implants demonstrated suppress spermatogenesis in 85% of men [25]. Another study, where testosterone pellets were implanted sub-dermally every 4 - 6 months along with intramuscular administration of medroxy progesterone acetate achieved sperm count less that 1 million/ml in 53 out of 55 men and entered the efficacy phase [26].
3.3.2. Transdermal Testosterone
Transdermal T-patches were earlier used for treatment of hypogonadism and have also been tested for contraceptive efficacy (Figure 5). However, the approach did not appear to be effective as it lowers serum testosterone levels which results into suboptimal suppression of spermatogenesis and the patches resulted into dermatitis [27]. As an alternative to transdermal testosterone patches, testosterone gels have been used to treat hypogonadism [28]. T-gels in combination with depot medroxy progesterone acetate (DMPA) also act as potential contraceptive agents by providing severe oligospermia to azoospermia [29]. T-gels have indicated better serum testosterone levels and less irritation as compared to T-patches.
4. Factors Affecting Development of Testosterone Based Contraception
4.1. Degree of Suppression/Duration of Exposure
Different dose regimens of TE and TU have been tested for the contraceptive efficacy. Lower doses (200 mg TE

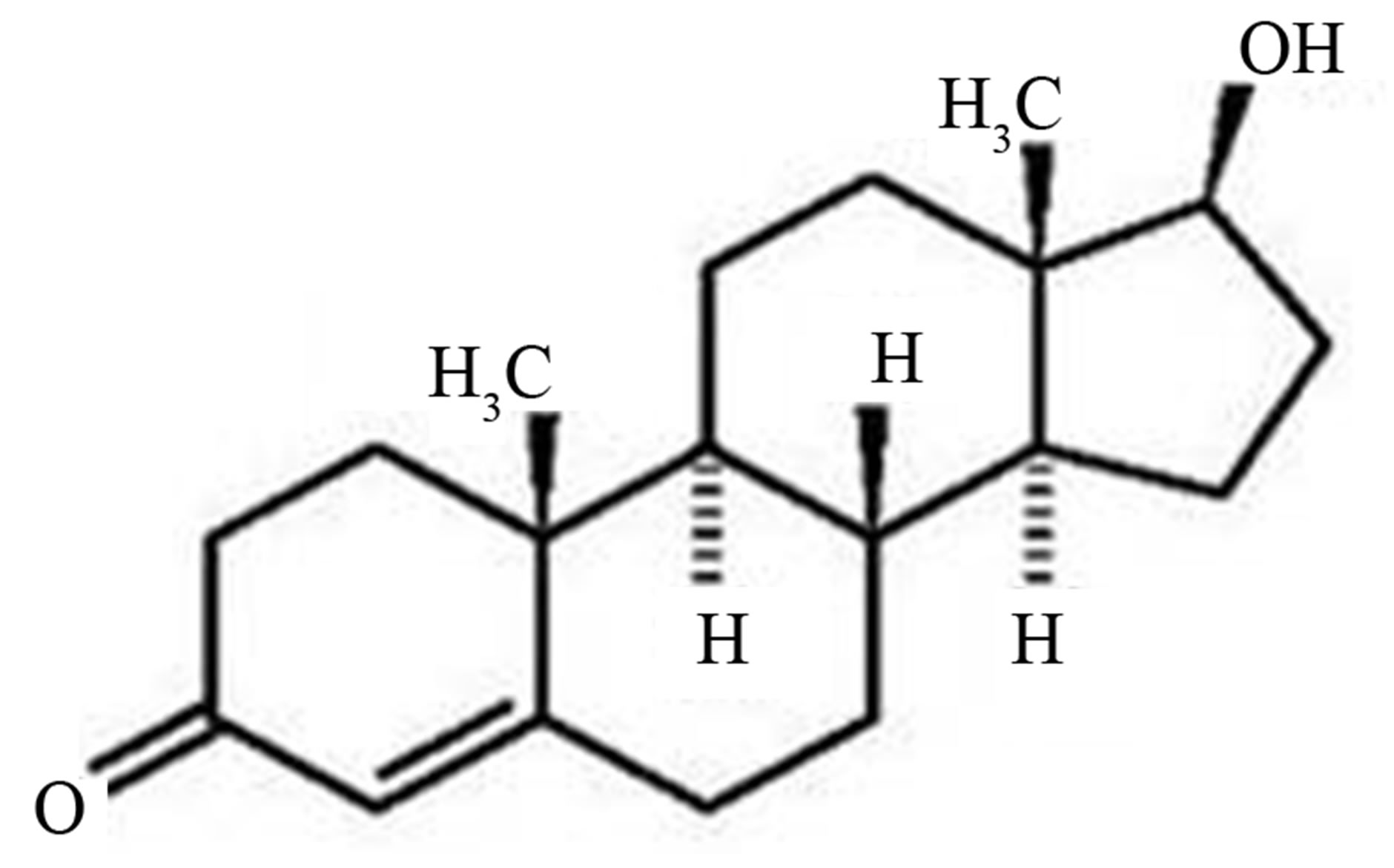
Figure 4. Structure of testosterone and testosterone pellets.

Figure 5. Transdermal testosterone patches.
and 125 mg TU) have failed to provide uniform azoospermia compared to higher dose (1000 mg TU) regimens while higher doses have been reported to cause androgen related side effects. Long duration of exposure has resulted in more profound side effects. To overcome these limitations other progestin such as depot-medroxyprogesterone acetate (DMPA), levonorgestrel (LNG), cyproterone acetate (CPA), 19-norethisterone (NETE) etc. have been synergistically used in combination with testosterone preparations (TE and TU).
4.2. Acceptability
Non-injectable androgen preparations like T-patches, Tgels and oral TU failed to provide uniform azoospermia as compared to intramuscular testosterone preparations such as TE and TU. To overcome these adverse effects, transdermal testosterone patches have also been tested for contraceptive efficacy. However, weekly intramuscular injections and related side effects during long term administration are few drawbacks of testosterone enanthate that affect its acceptability as contraceptive use. The application of T-patches had side effects like, irritation, dermatitis etc., and all these drawbacks further lead to their unacceptability as effective contraceptive regimen. To overcome these limitations, new combination approaches have been evaluated for contraceptive efficacy.
4.3. Side Effects
Exogenous testosterone administration has profound effects on circulating androgen levels, viz., suppression of androgen levels, elevated levels of estrogens etc. Androgen related side effects include acne, weight gain, decrease in HDL-cholesterol and increased haemopoeisis.
4.4. Ethnic Variations
Ethnic variations in the suppression of spermatogenesis have been experienced with administration of exogenous testosterone [20,21]. Following exogenous testosterone administration, LH pulses were found to be more suppressed in Asian men compared to Caucasians [6]. A higher rate of azoospermia (90% - 100%) has been reported in Asian men compared to Caucasians [20,21]. Similarly, male germ cell production was higher in Asian men versus non-Asian men [7]. The potential explanation may be the subtle differences in genetic makeup/gene involved in synthesis/metabolism of steroid hormones [30].
4.5. Pharmaceutical Support
In recent years, various pharmaceutical companies have extended financial support for development of new hormonal contraceptive in clinical trials using TU in combination with etonorgestral [31]. Earlier, to overcome the short acting effect of TE, a new preparation Testosterone bucciclate (TB) has been developed, however fails to reach clinical trials as no industrial partner was available for further productions.
5. Testosterone Analogs and Progestin Combination as Contraceptive Agents
It is obvious from clinical trials that androgen preparations such as TE and TU have resulted into azoospermia and severe oligospermia (<3 million count/ml) in >90% subjects at lower dose regimens (200 mg TE i.m. weekly and 500 mg TU monthly injection) [13,20]. However, higher doses have resulted into androgen related side effects. To overcome the side effects, co-administration of androgen-progestin regimen has been investigated for contraceptive efficacy. In early 1970’s progestins have been widely tested for female contraception and known to act as both anti-androgen and anti-gonadotropic. Addition of progestin to androgen preparations reduced androgen related side effects due to anti-androgenic action, while suppression of spermatogenesis achieved by anti-gonadotropic effects. With this rationale several androgenprogestin regimens have been tested for contraceptive efficacy and few are currently in phased III clinical trials.
5.1. Cyproterone Acetate
The synthetic steroid cyproterone acetate (6α-chloro-1, 2 α-methylene-17 α hydroxy-pregn-4,6-diene-3,20-dione- 17 acetate; CPA) (Figure 6) has been shown to be effective anti-androgen by inhibiting the release of gonadotropins from pituitary [14]. Cyproterone acetate is also a promising progestin studied for contraceptive efficacy in combination with TE [32]. The CPA act through both anti-gonadotropic and anti-androgenic action. The CPA in combination with TE has provided a rapid suppression of spermatogenesis. Administration of combination regimen of CPA (daily oral 1 mg/kg b.w.) and TE (2 mg/kg b.w./15 days; i.m.) to adult male langur monkeys over a period of 90 days caused a gradual decrease in the sperm count and motility without altering androgenicity and without
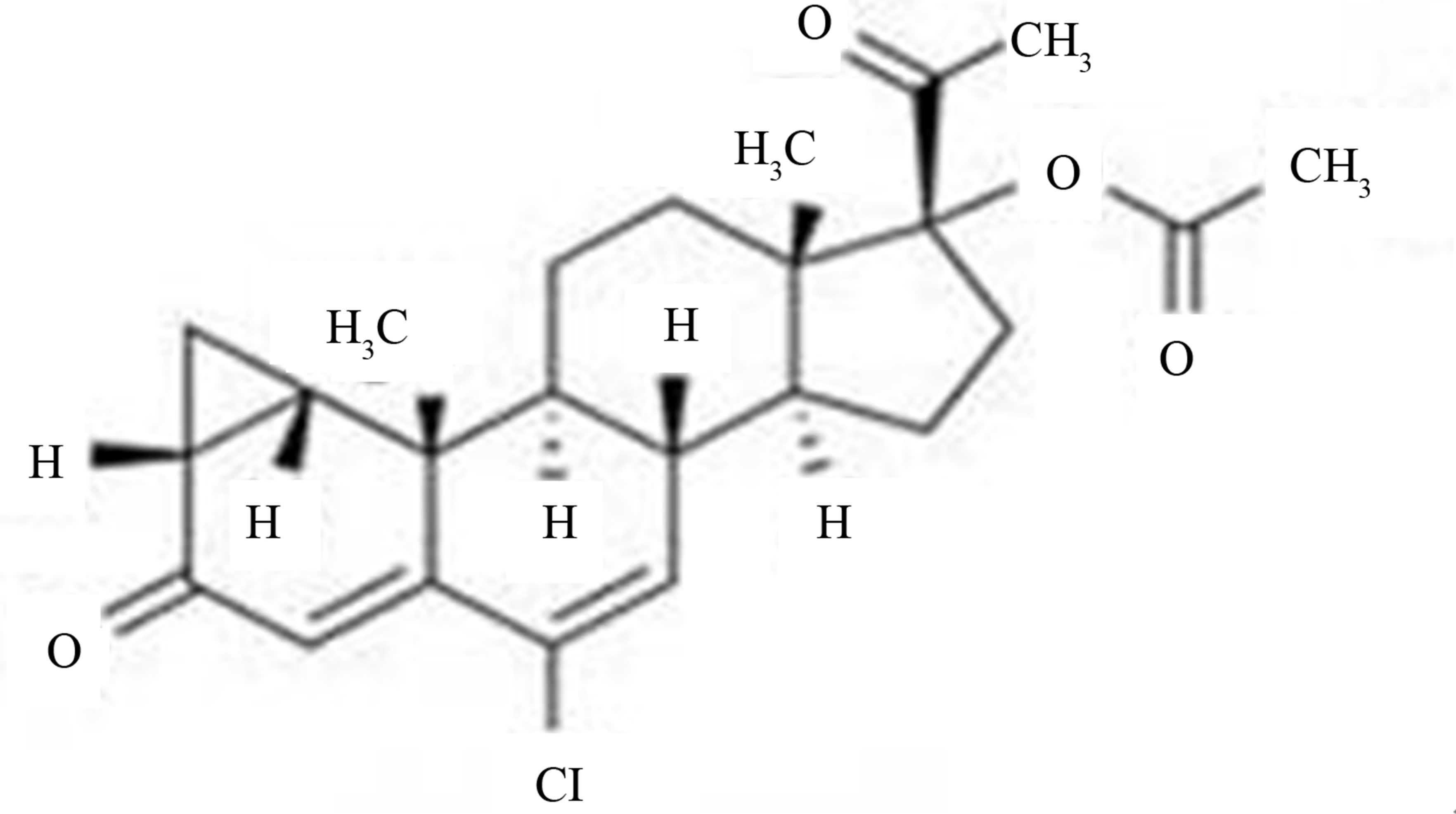
Figure 6. Chemical structure of cyproterone acetate.
affecting libido [32,33]. A dose dependent suppression of spermatogenesis has been reported when CPA administered in combination of 100 mg TE weekly as compared to 100 mg TE alone [34,35]. Low doses of CPA at a dose of 25 mg/day (CPA-25; n = 5) or 12.5 mg/day (CPA-12.5; n = 5) plus TE 100 mg/week, for 16 weeks have also been tested for contraceptive efficacy. All five men in group CPA-25 and three men in group CPA-12.5 achieved azoospermia. No appreciable changes in testosterone levels and biochemical parameters were reported. Thus, suggest a combination hormonal regimen as an effective, safe and reversible male contraceptive [36]. However, decrease in hemoglobin, body weight and hepatic dysfunction lead to discontinuation of CPA plus TE combination from clinical trials.
5.2. Depot Medroxyprogesterone Acetate
Depot-medroxyprogesterone acetate (DMPA) is a longacting form of the synthetic progestin having weak androgenic property (Figure 7). DMPA is administered as a single 150 mg intramuscular (i.m.) injection every 3 months and appears to be a potent inhibitor of gonadotropins [15]. The spermatogenesis was rapidly and completely suppressed after the administration of 500 mg TU in tea seed oil every 6 weeks in combination with 250 mg DMPA every 12 weeks in Indonesian men [37]. An 8- week regimen of TU plus DMPA at both tested (1000 mg TU plus 150 mg DMPA v/s 1000 mg TU plus 300 mg DMPA) combination doses effectively suppressed spermatogenesis to azoospermia in Chinese men. No serious adverse effects were reported [38]. The lower-dose combination was recommended for further testing in an expanded clinical trial or contraceptive efficacy study.
5.3. Desogestrel and Etonogestrel
Desogestrel (DSG) is a third generation synthetic progestin with potent progestogenic but lesser androgenecity (Figure 8(a)). Desogestrel oral regimens (50, 100, 150
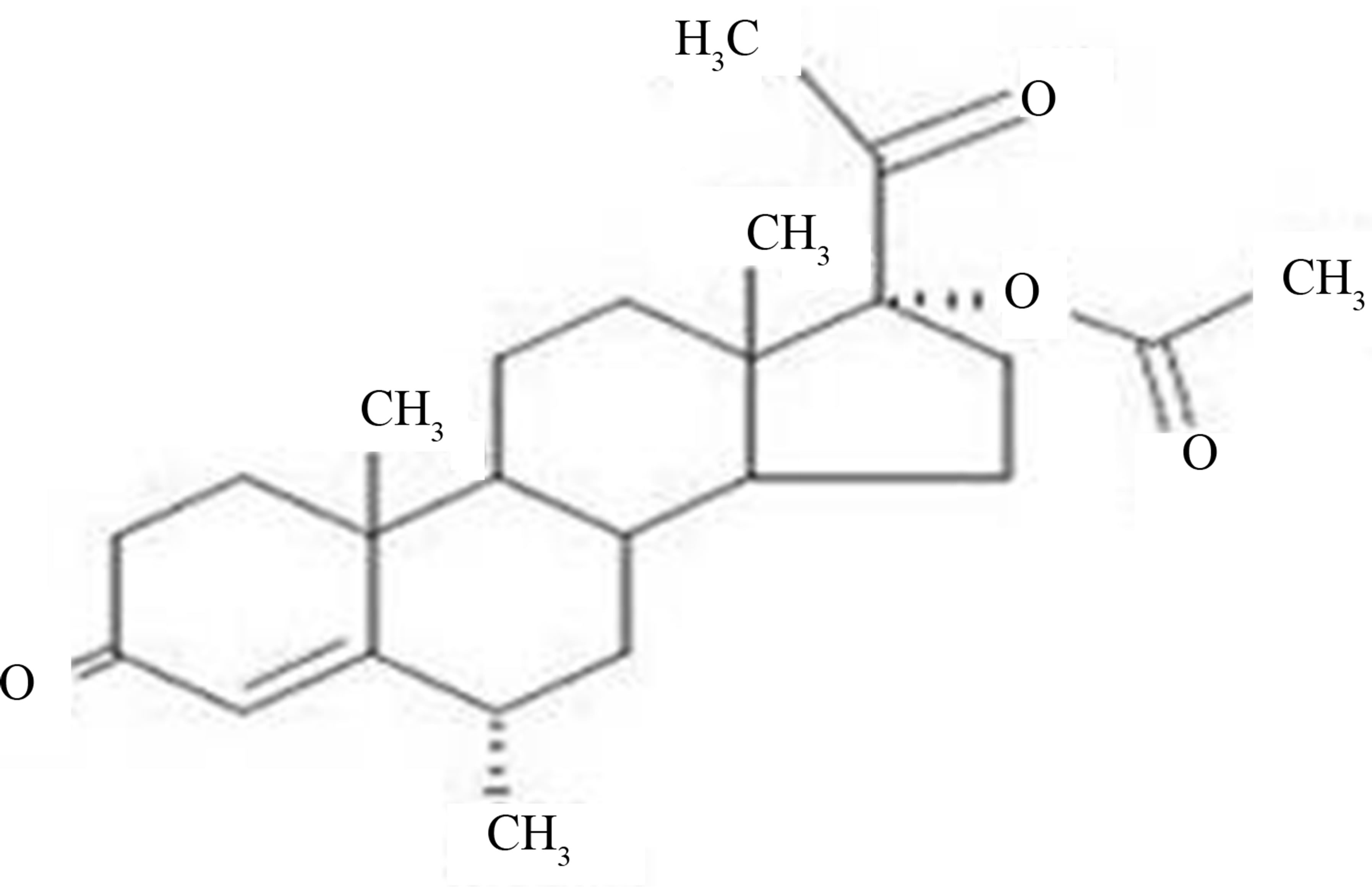
Figure 7. Chemical structure of depot-medroxyprogesterone acetate.
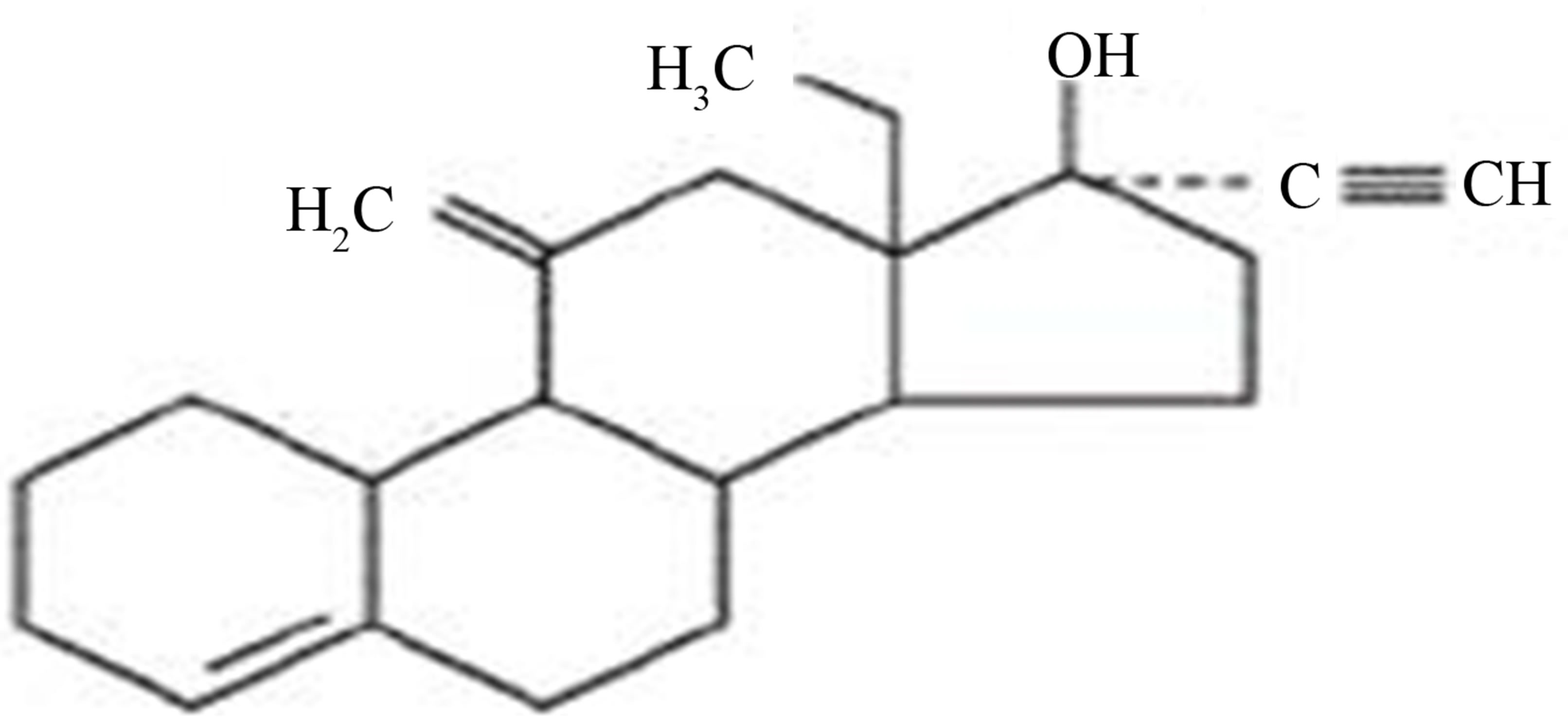 (a)
(a)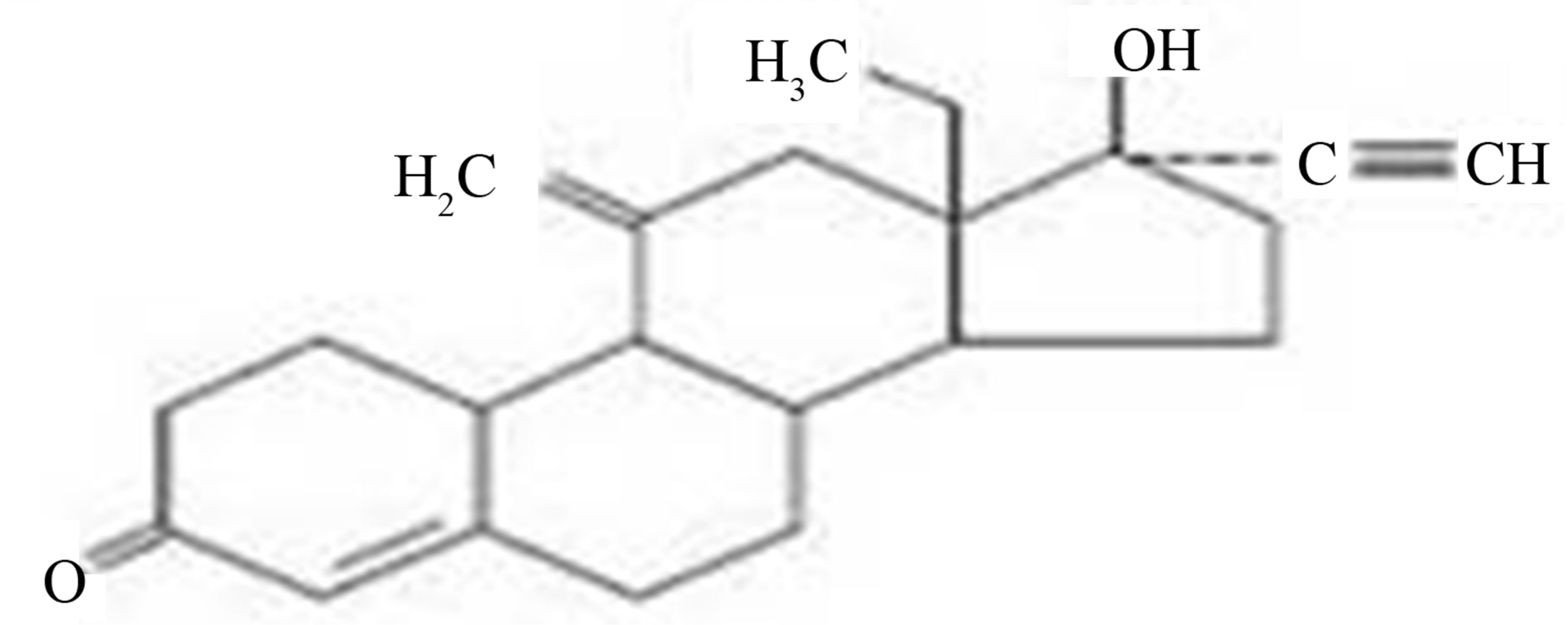 (b)
(b)
Figure 8. Chemical structure of (a) desogestrel and (b) etonogestrel.
and 300 mg) have been tested for contraceptive efficacy in combination with TE and T-implants [39-41]. Findings have suggested that 300 mg dose regimen of DSG in combination with 100 mg TE (i.m. weekly to 24 weeks), 400 mg testosterone pellets (subcutaneous) and 100 mg TE (for 6 months) were able to induce azoospermia in all tested subjects, respectively. However, higher dose of DSG (300 mg) resulted into reduction of HDL-Cholesterol levels. Etonogestrel (3-keto desogestrel, ENG) is an active metabolite of desogestrel (Figure 8(b)). Administration of etonogestrel implants at an appropriate dose together with a long-acting testosterone preparation induces profound and constant suppression of spermatogenesis that can be maintained for a period of 1 year [25,42]. The combination of 300 µg ENG with 400 mg testosterone decanoate (TD) every 4 weeks proved superior in terms of efficacy, hormone profiles, and safety compared to 300 µg oral ENG daily and 400 mg TD every 6 weeks. This represents a promising approach to male hormonal contraception [43].
5.4. Levonorgestrel
Levonorgestrel (LNG) is a second generation synthetic progestogen used as an active ingredient in female hormonal contraceptives, viz., contraceptive pills (Figure 9) [44]. Various regimens of LNG have been tested for male contraceptive efficacy along with testosterone preparation. The LNG 500 mg daily with TE (100 mg/ week) provides greater azoospermia compared to administration of TE alone [45]. Different dose regimens of LNG have been compared for minimal dose administration and better contraceptive efficacy. Two lower doses of LNG (125 mg and 250 mg) in combination with TE (100 mg) i.m. weekly for 6 weeks were compared. The higher dose (250 mg) leads to 78% azoospermia as compared to 67% in lower dose (125 mg) [46]. While two other LNG regimens (31.25 mg versus 62.50 mg), both in combination with TE (100 mg; i.m. for 6 months), showed no significant difference in azoospermia percentile [47]. Likewise, no significant difference in azoospermia (57% versus 50%) state was observed when compared to 250 mg LNG with or without 100 mg TE ( i.m. weekly injections for six weeks) [48]. Moreover, a 125 mg LNG doses in combination either with TE, dutastride or acyline have been tested and resulted in non-significant azoospermia percentile (60% - 80%) [49]. Another combination of LNG 125 mg dose regimen/ LNG implant with T-patches had achieved < 60 % azoospermia [50]. These findings suggest that testosterone preparation plays an important role in the suppression of gonadotropins.
5.5. Norethisterone Enanthate
The 19-norethisterone (NETE) is the oldest synthetic gestagen used for female contraception (Figure 10). Three different dose regimens of NETE with different intervals along with TU have been studied and higher doses of 400 mg NETE with 1000 mg TU injection at 6 week interval had resulted into azoospermia in 92% men [51]. It has been reported that even 8-week interval between two consecutive dose of TU (1000 mg), does not affect the contraceptive efficacy when administered with 200 mg NETE [52]. The NETE (200 mg) with two different dose regimens of TU i.e., 750 mg v/s 1000 mg/8

Figure 9. Chemical structure of levonorgestrel.
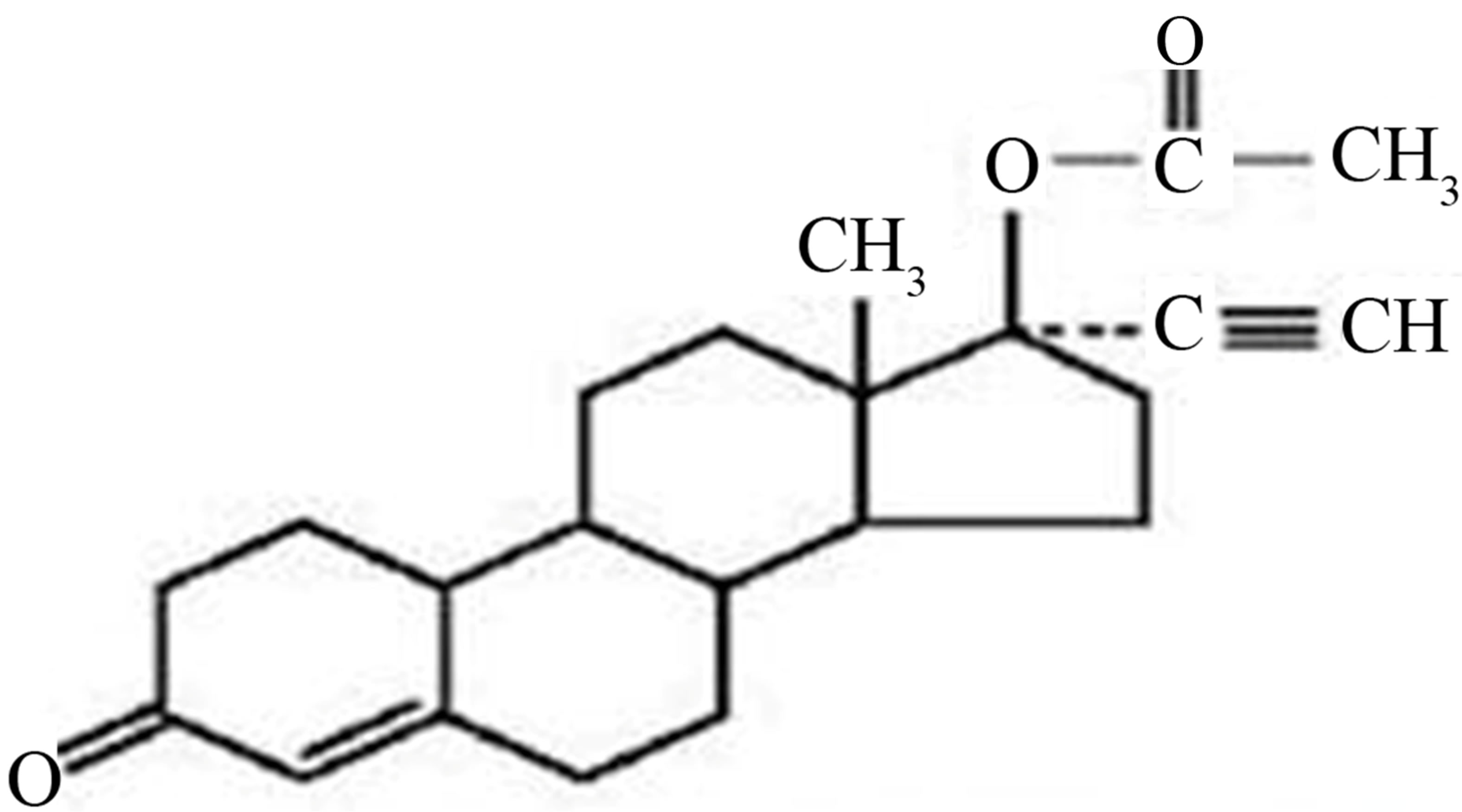
Figure 10. Chemical structure of norethisterone enanthate.
weekly injection up to 24 weeks resulted in variable azoospermia (30% to 70%), respectively [53].
6. Conclusion
In conclusion, researches during past several decades have shown advancement in the development of testosterone based contraceptive regimen. Initially, only testosterone and testosterone analogs were tested which failed to provide uniform azoospermia. To overcome these limitations, new testosterone based combinations (androgen-progestin) were examined for contraceptive efficacy. Short term clinical studies have shown promising results in suppression of spermatogenesis with no significant changes in clinical parameters, viz., hematology and clinical biochemistry such as lipid profile etc. However, long-term clinical trials > 10 years or more are required to confirm the safety of androgen-progestin regimens currently under clinical trials. In view of struggle in advancement of developing effective male hormonal contraceptive, alternative methods of male contraception have been approached. Amongst them, the vas based approaches have led to achieving uniform azoospermia and are under advanced clinical trials.
REFERENCES
- L. B. Finer and M. R. Zolna, “Unintended Pregnancy in the United States: Incidence and Disparities, 2006,” Contraception, Vol. 84, No. 5, 2011, pp. 478-485. doi:10.1016/j.contraception.2011.07.013
- S. K. Henshaw, “Unintended Pregnancy in the United States,” Family Planning Perspectives, Vol. 30, No. 1, 1998, pp. 24-29. doi:10.2307/2991522
- N. J. Hackel, “Production of Oligospermia in Man by the Use of Testosterone Propionate,” Experimental Biology and Medicine, Vol. 40, No. 4, 1939, pp. 658-659. doi:10.3181/00379727-40-10527P
- E. P. McCllagh and F. J. McGurl, “Further Observation on Clinical Use of Testosterone Propionate,” Journal of Urology, Vol. 42, 1939, pp. 1265-1267.
- A. D. Coviello, A. M. Matsumoto, W. J. Bremner, K. L. Herbst, J. K. Amory and B. D. Anawalt, “Low-Dose Human Chorionic Gonadotropin Maintains Intratesticular Testosterone in Normal Men with Testosterone-Induced Gonadotropin Suppression,” The Journal of Clinical Endocrinology & Metabolism, Vol. 90, No. 5, 2005, pp. 2595-2602. doi:10.1210/jc.2004-0802
- C. Wang, N. G. Berman, J. D. Veldhuis, T. Der, V. McDonald, B. Steiner and R. S. Swerdloff, “Graded Testosterone Infusions Distinguish Gonadotropin NegativeFeedback Responsiveness in Asian and White Men—A Clinical Research Center Study,” The Journal of Clinical Endocrinology & Metabolism, Vol. 83, No. 3, 1998, pp. 870-876. doi:10.1210/jc.83.3.870
- S. A. P. Hikim, C. Wang, Y. Lue, L. Johnson, X. H. Wang and R. S. Swerdloff, “Spontaneous Germ Cell Apoptosis in Humans: Evidence for Ethnic Differences in the Susceptibility of Germ Cells to Programmed Cell Death,” The Journal of Clinical Endocrinology & Metabolism, Vol. 83, No. 1, 1998, pp. 152-156. doi:10.1210/jc.83.1.152
- P. Aaltonen, J. K. Amory, R. A. Anderson, H. M. Behre, G. Bialy and D. Blithe, “10th Summit Meeting Consensus: Recommendations for Regulatory Approval for Hormonal Male Contraception,” Journal of Andrology, Vol. 28, No. 3, 2007, pp. 362-363. doi:10.2164/jandrol.106.002311
- G. R. Cunningham, V. E. Silverman, J. Thornby and P. O. Kohler, “The Potential for an Androgen Male Contraceptive,” The Journal of Clinical Endocrinology & Metabolism, Vol. 49, No. 4, 1979, pp. 520-526. doi:10.1210/jcem-49-4-520
- C. J. Bagatell, A. M. Matsumoto, R. B. Christensen, J. E. Rivier and W. J. Bremner, “Comparison of a Gonadotropin Releasing-Hormone Antagonist Plus Testosterone (T) Versus T Alone as Potential Male Contraceptive Regimens,” The Journal of Clinical Endocrinology & Metabolism, Vol. 77, No. 2, 1993, pp. 427-432. doi:10.1210/jc.77.2.427
- M. Y. Roth, S. T. Page, K. Lin, B. D. Anawalt, A. M. Matsumoto, B. Marck, W. J. Bremner and J. K. Amory, “The Effect of Gonadotropin Withdrawal and Stimulation With Human Chorionic Gonadotropin on Intratesticular Androstenedione and DHEA in Normal Men,” The Journal of Clinical Endocrinology & Metabolism, Vol. 96, No. 4, 2011, pp. 1175-1181. doi:10.1210/jc.2010-2518
- P. J. Snyder and D. A. Lawrence, “Treatment of Male Hypogonadism with Testosterone—Enanthate,” The Journal of Clinical Endocrinology & Metabolism, Vol. 51, No. 6, 1980, pp. 1335-1339. doi:10.1210/jcem-51-6-1335
- Y. Q. Gu, X. H. Wang, D. Xu, L. Peng, L. F. Cheng, M. K. Huang, Z. J. Huang and G. Y. Zhang, “A Multicenter Contraceptive Efficacy Study of Injectable Testosterone Undecanoate in Healthy Chinese Men,” The Journal of Clinical Endocrinology & Metabolism, Vol. 88, No. 2, 2003, pp. 562-568. doi:10.1210/jc.2002-020447
- F. Neumann, R. Von Bersworelt-Wallrabe, W. Elger, H. Stienbeck, J. D. Hahn and M. Kramer, “Aspects of Androgen-Dependent Events as Studied by Antiandrogens,” Recent Progress in Hormone Research, Vol. 26, 1970, pp. 337- 410.
- Z. Laron, G. Rumney, L. Rat and N. Naji, “Effects of 17α-hydroxy 6α-methyl-Progesterone Acetate (Depoprovera) on Urinary Gonadotrophins and Oestrogens in Man,” Acta Endocrinologica, Vol. 44, 1963, pp. 75-80.
- M. R. N. Prasad and M. Rajalakshmi, “Recent Advances in the Control of Male Reproductive Functions,” In: R. O. Greep, Ed., International Review of Physiology, Reproductive Physiology II, 2nd Edition, University Park Press, Baltimore, 1977, pp. 153-159.
- L. L. Ewing, L. G. Stratton and C. Desjardins, “Effect of Testosterone Polydimethyl-Siloxane Implants upon Sperm Production, Libido and Accessory Sex Organ Function in Rabbits,” Journal of the Society for Reproduction and Fertility, Vol. 25, No. 2, 1973, pp. 245-253. doi:10.1530/jrf.0.0350245
- R. S. Swerdloff, A. Palacios, R. D. McClure, L. A. Campfield and S. A. Brosmen, “Clinical Evaluation of Testosterone Enanthate in the Reversible Suppression of SpermAtogenesis in the Human Male: Efficacy, Mechanism of Action and Adverse Effects,” In: D. J. Patanelli, Ed., Hormonal Control of Male Fertility, US DHEW (NIH), Bethesda, 1978, pp. 41-70.
- D. Jayaprakash, K. Sharma, A. S. Ansari and N. K. Lohiya, “Testosterone Enanthate, Single Entity Male Contraceptive Agent in Langur Monkey,” European Archives of Biology, Vol. 105, No. 3, 1994, pp. 103-110.
- World Health Organization Task Force on Methods for the Regulation of Male Fertility, “Contraceptive Efficacy of Testosterone Induced Azoospermia and Oligozoospermia in Normal Men,” Fertility and Sterility, Vol. 65, No. 4, 1996, pp. 821-829.
- World Health Organization Task Force on Methods for the Regulation of Male Fertility, “Contraceptive Efficacy of Testosterone-Induced Azoospermia in Normal Men,” Lancet, Vol. 336, No. 8721, 1990, pp. 955-959. doi:10.1016/0140-6736(90)92416-F
- Y. Gu, X. Liang, W. Wu, M. Liu, S. Song, L. Cheng, L. Bo, C. Xiong, X. Wang, X. Liu, L. Peng and K. Yao, “Multicenter Contraceptive Efficacy Trial of Injectable Testosterone Undecanoate in Chinese Men,” The Journal of Clinical Endocrinology & Metabolism, Vol. 94, No. 6, 2009, pp. 1910-1915. doi:10.1210/jc.2008-1846
- K. Heinemann, F. Saad, M. Wiesemes, S. White and L. Heinemann, “Attitudes toward Male Fertility Control: Results of a Multinational Survey on Four Continents,” Human Reproduction, Vol. 20, No. 2, 2005, pp. 549-556. doi:10.1093/humrep/deh574
- D. J. Handelsman, A. J. Conway, C. J. Howe, L. Turner and M. A. Mackey, “Establishing the Minimum Effective Dose and Additive Effects of Depot Progestin in Suppression of Human Spermatogenesis by a Testosterone Depot,” The Journal of Clinical Endocrinology & Metabolism, Vol. 81, No. 11, 1996, pp. 4113-4121. doi:10.1210/jc.81.11.4113
- R. A. Anderson, D. Kinniburgh and D. T. Baird, “Suppression of Spermatogenesis by Etonogestrel Implants With Depot Testosterone: Potential for Long-Acting Male Contraception,” The Journal of Clinical Endocrinology & Metabolism, Vol. 87, No. 8, 2002, pp. 3640-3649. doi:10.1210/jc.87.8.3640
- L. Turner, A. J. Conway, M. Jimenez, P. Y. Liu, E. Forbes, R. I. McLachlan and D. J. Handelsman, “Contraceptive Efficacy of a Depot Progestin and Androgen Combination in Men,” The Journal of Clinical Endocrinology & Metabolism, Vol. 88, No. 10, 2003, pp. 4659- 4667. doi:10.1210/jc.2003-030107
- J. K. Amory, S. T. Page, B. D. Anawalt, A. M. Matsumoto and W. J. Bremner, “Acceptability of a Combination Testosterone Gel and Depot-Medroxyprogesterone Acetate Male Contraceptive Regimen,” Contraception, Vol. 75, No. 3, 2007, pp. 218-223. doi:10.1016/j.contraception.2006.11.003
- R. S. Swerdloff and C. Wang, “Three-Year Follow-Up of Androgen Treatment in Hypogonadal Men: Preliminary Report with Testosterone Gel,” Aging Male, Vol. 6, No. 3, 2003, pp. 207-211.
- S. T. Page, J. K. Amory, B. D. Anawalt, M. S. Irwig, A. T. Brockenbrough, A. M. Matsumoto and W. J. Bremner, “Testosterone Gel Combined with Depomedroxy-Progesterone Acetate is an Effective Male Hormonal Contraceptive Regimen and is Not Enhanced by the Addition of a GnRH Antagonist,” The Journal of Clinical Endocrinology & Metabolism, Vol. 91, No. 11, 2006, pp. 4374- 4380. doi:10.1210/jc.2006-1411
- C. S. Yadav, M. Bajpai, V. Kumar, S. K. Datta, P. Gupta, R. S. Ahmed and B. D. Banerjee, “Polymorphisms in the P450 c17 (17-Hydroxylase/17, 20-Lyase) Gene: Association with Estradiol and Testosterone Concentration in Hypospadias,” Urology, Vol. 78, No. 4, 2011, pp. 902- 907. doi:10.1016/j.urology.2011.04.021
- C. Wang and R. S. Swerdloff, “Hormonal Approaches to Male Contraception,” Current Opinion in Urology, Vol. 20, No. 6, 2010, pp. 520-524, doi:10.1097/MOU.0b013e32833f1b4a
- N. K. Lohiya and O. P. Sharma, “Effects of Cyproterone Acetate with Combination of Testosterone Enanthate on Seminal Characteristics, Androgenicity and Clinical Chemistry in Langur Monkey,” Contraception, Vol. 28, No. 6, 1983, pp. 575-586. doi:10.1016/0010-7824(83)90108-7
- N. K. Lohiya, O. P. Sharma, R. C. Sharma and R. S. Sharma, “Reversible Sterility by Cyproterone Acetate Plus Testosterone Enanthate in Langur Monkey with Maintenance of Libido,” Biomedica Biochemica Acta, Vol. 46, No. 4, 1987, pp. 259-266.
- M. C. Meriggiola, W. J. Bremner, C. A. Paulsen, A. Valdiserri, L. Incorvaia, R. Motta, A. Pavani, M. Capelli and Flamigni, “A Combined Regimen of Cyproterone Acetate and Testosterone Enanthate as a Potentially Highly Effective Male Contraceptive,” The Journal of Clinical Endocrinology & Metabolism, Vol. 81, No. 8, 1996, pp. 3018-3023. doi:10.1210/jc.81.8.3018
- M. C. Meriggiola, A. Costantino, S. Cerpolini, W. J. Bremner, D. Huebler, A. M. Morselli Labate, B. Kirsch, A. Bertaccini, C. Pelusi and G. Pelusi, “Testosterone Undecanoate Maintains Spermatogenic Suppression Induced by Cyproteroneacetate Plus Testosterone Undecanoate in Normal Men,” The Journal of Clinical Endocrinology & Metabolism, Vol. 88, No. 12, 2003, pp. 5818-5826. doi:10.1210/jc.2003-030574
- M. C. Meriggiola, W. J. Bremner, A. Costantino, G. Di Cintio and C. Flamigni, “Low Dose of Cyproterone Acetate and Testosterone Enanthate for Contraception in Men,” Human Reproduction, Vol. 13, No. 5, 1998, pp. 1225-1229. doi:10.1093/humrep/13.5.1225
- N. Moeloek, D. A. Pujianto and R. Agustin, “Achieving Azoospermia by Injections of Testosterone Undecanoate Alone or Combined with Depot Medroxyprogesterone Acetate in Indonesian Men (Jakarta Center Study),” Proceeding of the 7th International Congress of Andrology, Montreal, 15-19 June 2001, Poster 1/2-133.
- Y. Gu, J. S. Tong, D. Z. Ma, X. H. Wang, D. Yuan, W. H. Tang and W. J. Bremner, “Male Hormonal Contraception: Effects of Injections of Testosterone Undecanoate and Depot Medroxyprogesterone Acetate at Eight-Week Intervals in Chinese Men,” The Journal of Clinical Endocrinology & Metabolism, Vol. 89, No. 2, 2004, pp. 2254- 2262. doi:10.1210/jc.2003-031307
- F. C. Wu, R. Balasubramanian, T. M. Mulders and H. J. Coelingh-Bennink, “Oral Progestogen Combined with Testosterone as a Potential Male Contraceptive: Additive Effects Between Desogestrel and Testosterone Enanthate in Suppression of Spermatogenesis, Pituitary-Testicular Axis, and Lipid Metabolism,” The Journal of Clinical Endocrinology & Metabolism, Vol. 84, No. 1, 1999, pp. 112-122. doi:10.1210/jc.84.1.112
- B. D. Anawalt, K. L. Herbst, A. M. Matsumoto, T. M. Mulders, H. J. Coelingh-Bennink and W. J. Bremner, “Desogestrel Plus Testosterone Effectively Suppresses Spermato-Genesis but Also Causes Modest Weight Gain and High-Density Lipoprotein Suppression,” Fertility and Sterility, Vol. 74, No. 4, 2000, pp. 707-714. doi:10.1016/S0015-0282(00)01490-4
- D. Kinniburgh, H. Zhu, L. Cheng, A. T. Kicman, D. T. Baird and R. A. Anderson, “Oral Desogestrel with Testosterone Pellets Induces Consistent Suppression of Spermatogenesis to Azoospermia in both Caucasian and Chinese Men,” Human Reproduction, Vol. 17, No. 6, 2002, pp. 1490-1501. doi:10.1093/humrep/17.6.1490
- M. Brady, M. Walton, N. Hollow, A. T. Kicman, D. T. Baird and R. A. Anderson, “Depot Testosterone with Etonogestrel Implants Result in Induction of Azoospermia in all Men for Long-Term Contraception,” Human Reproduction, Vol. 19, No. 6, 2004, pp. 2658-2667. doi:10.1093/humrep/deh491
- J. Hay, B. M. Brady, M. Zitzmann, K. Osmanagaoglu, P. Pollanen and D. Apter, “A Multicenter Phase IIb Study of a Novel Combination of Intramuscular Androgen (Testosterone Decanoate) and Oral Progestogen (Etonogestrel) for Male Hormonal Contraception,” The Journal of Clinical Endocrinology & Metabolism, Vol. 90, No. 4, 2005, pp. 2042-2049. doi:10.1210/jc.2004-0895
- A. Nelson, “New Low-Dose, Extended-Cycle Pills with Levonorgestrel and Ethinyl Estradiol: An Evolutionary Step in Birth Control,” International Journal of Women’s Health, Vol. 2, 2010, pp. 99-106. doi:10.2147/IJWH.S4886
- R. A. Bebb, B. D. Anawalt, R. B. Christensen, C. A. Paulsen, W. J. Bremner and A. M. Matsumoto, “Combined Administration of Levonorgestrel and Testosterone Induces More Rapid and Effective Suppression of Spermatogenesis than Testosterone Alone: A Promising Male Contraceptive Approach,” The Journal of Clinical Endocrinology & Metabolism, Vol. 81, No. 2, 1996, pp. 757- 762. doi:10.1210/jc.81.2.757
- B. D. Anawalt, R. A. Bebb, W. J. Bremner and A. M. Matsumoto, “A Lower Dosage Levonorgestrel and Testosterone Combination Effectively Suppresses Spermatogenesis and Circulating Gonadotropin Levels with Fewer Metabolic Effects than Higher Dosage Combinations,” Journal of Andrology, Vol. 20, No. 3, 1999, pp. 407-414.
- B. D. Anawalt, J. K. Amory, K. L. Herbst, A. D. Coviello, S. T. Page, W. J. Bremner and A. M. Matsumoto, “Intramuscular Testosterone Enanthate Plus Very Low Dosage Oral Levonorgestrel Suppresses Spermatogenesis without Causing Weight Gain in Normal Young Men: A Randomized Clinical Trial,” Journal of Andrology, Vol. 26, No. 3, 2005, pp. 405-413. doi:10.2164/jandrol.04135
- A. Kamischke, D. Plöger, S. Venherm, S. von Eckardstein, A. von Eckardstein and E. Nieschlag, “Intramuscular Testosterone Undecanoate with or without Oral Levonorgestrel: A Randomized Placebo-Controlled Feasibility Study for Male Contraception,” Clinical Endocrinology, Vol. 53, No. 1, 2000, pp. 43-52. doi:10.1046/j.1365-2265.2000.01024.x
- K. L. Matthiesson, J. K. Amory, R. Berger, A. Ugoni, R. I. McLachlan and W. J. Bremner, “Novel Male Hormonal Contraceptive Combinations: The Hormonal and Spermatogenic Effects of Testosterone and Levonorgestrel Combined with a 5α-Reductase Inhibitor or Gonadotropin-Releasing Hormone Antagonist,” The Journal of Clinical Endocrinology & Metabolism, Vol. 90, No. 1, 2005, pp. 91-97. doi:10.1210/jc.2004-1228
- I. T. Gonzalo, R. S. Swerdloff, A. L. Nelson, B. Clevenger, R. Garcia, N. Berman and C. Wang, “Levonorgestrel Implants (Norplant II) for Male Contraception Clinical Trials: Combination with Transdermal and Injectable Testosterone,” The Journal of Clinical Endocrinology & Metabolism, Vol. 87, No. 8, 2002, pp. 3562- 3572. doi:10.1210/jc.87.8.3562
- A. Kamischke, T. Heuermann, K. Krüger, S. von Eckardstein, I. Schellschmidt, A. Rübig and E. Nieschlag, “An Effective Hormonal Male Contraceptive Using Testosterone Undecanoate With Oral or Injectable Norethisterone Preparations,” The Journal of Clinical Endocrinology & Metabolism, Vol. 87, No. 2, 2002, pp. 530-539. doi:10.1210/jc.87.2.530
- M. C. Meriggiola, A. Costantino, F. Saad, L. D'Emidio, A. M. Morselli Labate, A. Bertaccini, W. J. Bremner, I. Rudolph, M. Ernst, B. Kirsch, G. Martorana and G. Pelusi, “Norethisterone Enanthate plus Testosterone Undecanoate for Male Contraception: Effects of Various Injection Intervals on Spermatogenesis, Reproductive Hormones, Testis, and Prostate,” The Journal of Clinical Endocrinology & Metabolism, Vol. 90, No. 4, 2005, pp. 2005- 2014. doi:10.1210/jc.2004-1852
- A. Qoubaitary, C. Meriggiola, C. M. Ng, L. Lumbreras, S. Cerpolini and G. Pelusi, “Pharmacokinetics of Testosterone Undecanoate Injected Alone or in Combination with Norethisterone Enanthate in Healthy Men,” Journal of Andrology, Vol. 27, No. 6, 2006, pp. 853-867. doi:10.2164/jandrol.106.000281
NOTES
*Corresponding author.