Open Journal of Gastroenterology
Vol.05 No.05(2015), Article ID:56534,4 pages
10.4236/ojgas.2015.55008
CT-Guided Celiac Plexus Neurolysis in the Management of Pain Related to Unresectable Pancreatic Cancer: About 2 Cases
A. Souguir1*, A. Hammami1, Kh. Kadri2, I. Ben Mansour1, H. Jaziri1, A. Zayene1, A. Ben Slama1, M. Ksiaa1, A. Brahem1, S. Ajmi1, A. Jmaa1
1Department of Gastroenterology Sahloul, Sousse, Tunisia
2Department of Radiology Sahloul, Sousse, Tunisia
Email: *souguirahlem@yahoo.fr
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 1 March 2015; accepted 19 May 2015; published 22 May 2015
ABSTRACT
Celiac plexus neurolysis (CPN) has become a minimally invasive approach for the management of patients with unresectable pancreatic cancer and abdominal pain unresponsive to medical treat- ment. CPN has been shown to have long-lasting improvement in abdominal pain and decreased narcotic usage in 70% to 90% of patients. Therefore, the aim of this paper was to report our ex- perience with CPN in the treatment of two cases of advanced pancreatic cancer, with satisfying results in controlling pain. The use of CT scan-guided CPN should be considered and performed relatively early in the course of disease to offer optimal pain relief and increase the patient’s qua- lity of life.
Keywords:
Pancreas, Celiac Plexus Neurolysis, Unresectable Pancreatic Cancer, Palliative Treatment

1. Introduction
Pain is one of the major complications of advanced pancreatic cancer which is difficult to control, even with high doses of analgesics [1] [2] . Abdominal pain caused by pancreatic carcinoma is usually secondary to the progression of the tumor with neural invasion or nerve compression [3] . This neuropathic pain is a target for effective palliation. Conventional drugs do not provide adequate analgesia and many adverse effects are usually seen with opioids.
Therefore, methods leading to the interruption of pain transmission are promising options for pain relief and reduction of the risk of drug-induced adverse effects. Imaging-guided Celiac plexus neurolysis for refractory pain management has been used for almost 100 years in patients with advanced abdominal malignancy. It in- volves the injection of a neurolytic agent (absolute alcohol, most commonly) into or around the celiac plexus to disrupt these impulses and effectively control pain without the noted side effects typical of opioids [4] . To date, there are conflicting conclusions concerning its effectiveness in terms of pain alleviation and improvement of quality of life. The aim of this paper was to report the results of our experience with CPN in the treatment of two cases of unresectable pancreatic cancer and to highlight its safety and initial efficacy in pain relief.
2. Case 1
A 64-year-old woman was admitted in our department with a complaint of progressive worsening of abdominal pain in the mid-epigastrium radiating to the back, for four months, associated with alteration of her general con- dition. She had no past medical history. Her physical examination showed a mild tenderness in the right hypo- chondrium with hepatomegaly. No cutaneous stigmata of liver disease, or palpable adenopathy were present. There was no fever or icterus. Laboratory tests showed anicteric cholestasis (GGT: 4 N) and elevation of tumor markers (CA19-9 > 10000 UI/ml). The other biological tests were within normal limits. An abdominal CT scan showed a 4 × 5 cm soft-tissue mass in the head of the pancreas with adjacent celiomesenteric lymphadenopathy, encasement of the celiac artery and hepatic metastasis (Figure 1). The patient was then referred for palliative pain control with celiac plexux neurolysis (CPN) (Figure 2). Anterior approach has been chosen. The injection needle (22-gauge, Chiba biopsy needle) was placed into the targeted central position, and inserted through the anterior abdominal wall directly into the region of the celiac plexus. A single injection of 5 ml of absolute alco- hol was then administered. During the procedure, a biopsy of the tumor was performed and cytopathology con- firmed the diagnosis of adenocarcinoma. When the needle was withdrawn, there was no evidence of immediate complications. Within 48 hours of the procedure, the patient experienced significant pain relief with decrease in morphine requirements. A chemotherpy based on Gemcitabine was initiated but she died 9 months after.
3. Case 2
A sixty nine-year-old woman presented with the chief complaint of abdominal pain in the epigastrum, since eight months, with alteration of her general condition. Pain was dull in nature, radiating to the back, with no specific aggravating and relieving factors. There was no history of vomiting, jaundice, or fever. On physical examination, there was mild tenderness in the epigastrium. Laboratory investigations including complete blood count, liver function tests and urine analysis were within normal ranges. Erythrocyte sedimentation test, the C- reactive protein and the CA 19-9 were elevated. The upper endoscopy showed no abnormalities. A CT scan re- vealed a 5 cm mass in the body of the pancreas that encased the celiac and superior mesenteric artery origins (Figure 3). The patient was, at first, treated with high doses of opiate-based analgesics without any improve-

Figure 1. Cancer of the head of the pancreas with liver metastases.

Figure 2. CT-guided Celiac Plexus neurolysis performed with an anterior approach.
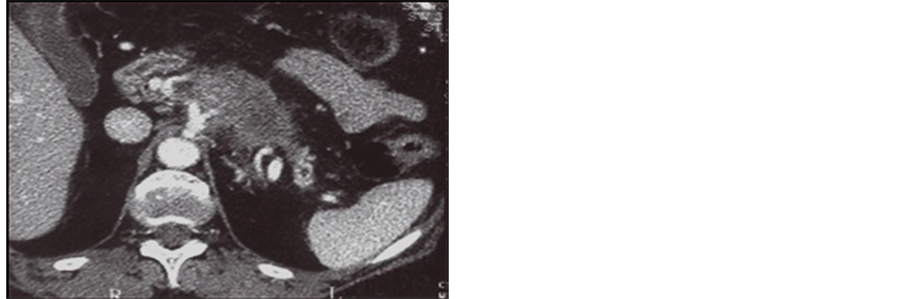
Figure 3. Pancreatic tumor with vascular invasion.
ment. Therefore, we decided to perform celiac plexus neurolysis. The procedure was done under deep sedation. Fine-needle aspiration biopsy under CT scan guidance, confirmed the diagnosis of adenocarcinoma. After the procedure, the patient was observed for 24 hours to identify any immediate complications such as hypotension, tachycardia, and pain enhancement. A short and spontaneously reversible episode of hypotension occurred. No immediate post-procedure complications were detected. After alcohol ablation therapy, abdominal pain disappeared and the patient was discharged on the next day. She was proposed for palliative chemotherapy but she died within two weeks following the CPN.
4. Discussion
Treatment of pain in patients with advanced pancreatic cancer is one of the most important challenges of palliative care. Although opioids effectively relieve pain, they are associated with many different adverse effects such as delirium, dry mouth, anorexia, constipation, nausea and vomiting [5] , which can determine a great decrease in quality of life and may also compromise the immune function. Since its initial description in 1914 by Kapisa [6] , Celiac plexus neurolysis (CPN) was performed as a technique that can potentially improve pain control in pancreatic cancer while preventing further escalation of opioid consumption [4] . It consists of a permanent destruction of celiac plexus in abdominal malignancies, by injection of neurolytic agent, and must be distinguished from endoscopic celiac plexus block that is performed in patients with benign disease and inhibit temporally the celiac plexus function by steroids or less commonly alcohol.
CPN modalities include surgical splanchnectomy, percutaneous CPN, and Endoscopic ultrasound-guided CPN. Patients who underwent percutaneous neurolysis experienced significant pain relief enabling reduction of analgesic doses, and improved quality of life [7] [8] . CPN involves the destruction of the sympathetic plexus by injecting alcohol near the celiac axis. In a previously published meta-analysis, radiological CPN was effective in controlling pain in 70% - 90% of patients [9] . Recently, Polati et al. [10] , demonstrated in a double-blinded study including 24 patients with pancreatic cancer who received percutaneous CPN that there was significant reduction in analgesic use and drug-related collateral effects in the study group compared to those who received medical therapy alone. The major disadvantage of percutaneous CPN is the possibility of occurrence of serious complications, in 1% - 2% of cases, including paraesthesia of lower extremities, paraplegia, injury of adjacent organs, gastroparesis and diarrhea [11] . More severe neurologic complications may also occur caused by spinal cord ischemia secondary to an injury of the arterial blood supply [12] . Celiac plexus neurolysis is performed under deep sedation and cardiorespiratory monitoring.
CT-scan guidance allowed for direct visualization of important vascular structures, particularly the aorta, celiac trunk, and superior mesenteric artery. One of the major aspects of CT is its ability to follow the spread of the neurolytic agent and to detect its leakage into the peritoneal cavity [13] . Appropriate patient positioning is crucial for a successful procedure. The position should allow the shortest and least complicated route to the celiac plexus. The most commonly described are prone, lateral decubitus, supine, and oblique. Once the needle is in position, an injection of 5 to 10 mL of dilute contrast (1 mL contrast: 9 mL saline) is performed, and CT images are obtained. Once correct position is confirmed by contrast dispersion, absolute alcohol is injected slowly (over 2 minutes) via the needle. The volume injected is variable, but typically is in the range of 10 to 40 mL. At the end of the procedure, the patient is observed for signs of peritonitis and hypotension [14] .
5. Conclusion
Although surgical resection has long been considered as the treatment of choice of pancreatic cancer, few patients are not eligible for surgery because of old age, comorbidities or advanced stage cancer. For these patients, successful application of CT scan guided ablation therapy using ethanol has been reported as a relatively safe and attractive method for relieving malignancies-related pain. Its greatest benefit lies in reducing opioid requirements and its related side effects. Prospective large trials should be performed to better evaluate this technique, its indications and complications before it is recommended for widespread use in clinical practice.
References
- Moore, J.C. and Adler, D.G. (2009) Celiac Plexus Neurolysis for Pain Relief in Pancreatic Cancer. Journal of Supportive Oncology, 7, 83-87, 90.
- Yan, B.M. and Myers, R.P. (2007) Neurolytic Celiac Plexus Block for Pain Control in Unresectable Pancreatic Cancer. American Journal of Gastroenterology, 102, 430-438. http://dx.doi.org/10.1111/j.1572-0241.2006.00967.x
- Bockman, D.E. (1998) An Introduction to Surgical Anatomy and Neuroanatomy. In: Berger, H.G., Warshaw, A.L., Buchler, M.W., Eds., The Pancreas, Blackwell Science, Oxford, 11-18.
- Eisenberg, E., Carr, D.B. and Chalmers, T.C. (1995) Neurolytic Celiac Plexus Block for Treatment of Cancer Pain: A Meta-Analysis. Anesthesia and Analgesia, 80, 290-295.
- Caraceni, A. and Portenoy, R.K. (1996) Pain Management in Patients with Pancreatic Carcinoma. Cancer, 78, 639-653. http://dx.doi.org/10.1002/(SICI)1097-0142(19960801)78:3<639::AID-CNCR45>3.0.CO;2-X
- Kappis, M. (1914) Erfahrungen Mit Localanasthesie bie bauchoperationen. Vehr Dtsch Gesellsch Chir, 43, 87-89.
- Yan, B.M. and Myers, R.P. (2007) Neurolytic Celiac Plexus Block for Pain Control in Unresectable Pancreatic Cancer. American Journal of Gastroenterology, 102, 430-438. http://dx.doi.org/10.1111/j.1572-0241.2006.00967.x
- Michaels, A.J. and Draganov, P.V. (2007) Endoscopic Ultrasonography Guided Celiac Plexus Neurolysis and Celiac Plexus Block in the Management of Pain Due to Pancreatic Cancer and Chronic Pancreatitis. World Journal of Gastroenterology, 13, 3575-3580. http://dx.doi.org/10.3748/wjg.v13.i26.3575
- Soweid, A.M. and Azar, C. (2010) Endoscopic Ultrasound-Guided Celiac Plexus Neurolysis. World Journal of Gastrointestinal Endoscopy, 16, 228-231. http://dx.doi.org/10.4253/wjge.v2.i6.228
- Polati, E., Finco, G., Gottin, L., Bassi, C., Pederzoli, P. and Ischia, S. (1998) Prospective Randomized Double-Blind Trial of Neurolytic Coeliac Plexus Block in Patients with Pancreatic Cancer. British Journal of Surgery, 85, 199-201. http://dx.doi.org/10.1046/j.1365-2168.1998.00563.x
- Davies, D.D. (1993) Incidence of Major Complications of Neurolytic Coeliac Plexus Block. Journal of the Royal Society of Medicine, 86, 264-266. http://dx.doi.org/10.1097/00132586-199312000-00033
- Van Dongen, R.T. and Crul, B.J. (1991) Paraplegia Following Coeliac Plexus Block. Anaesthesia, 46, 862-863. http://dx.doi.org/10.1111/j.1365-2044.1991.tb09603.x
- Wang, P.J., Shang, M.Y., Qian, Z., Shao, C.W., Wang, J.H. and Zhao, X.H. (2006) CT-Guided Percutaneous Neurolytic Celiac Plexus Block Technique. Abdom Imaging, 31, 710-718. http://dx.doi.org/10.1007/s00261-006-9153-5
- Nitschke, A.M. and Ray Jr., C.E. (2013) Percutaneous Neurolytic Celiac Plexus Block. Seminars in Interventional Radiology, 30, 318-321. http://dx.doi.org/10.1055/s-0033-1353485
NOTES

*Corresponding author.