Open Journal of Radiology
Vol.05 No.03(2015), Article ID:58293,10 pages
10.4236/ojrad.2015.53020
Atypical CT and MRI Features of Focal Nodular Hyperplasia of Liver: A Study with Radiologic-Pathologic Correlation
Narendra Darai1, Rongbao Shu2, Rajkumar Gurung2, Xiaojuan Zhang2, Gaojun Teng2*
1Department of Radiology, Zhong Da Hospital, Southeast University, Nanjing, China
2Medical School, Southeast University, Nanjing, China
Email: darainaren@hotmail.com, *gjteng@vip.sina.com
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 17 June 2015; accepted 19 July 2015; published 24 July 2015
ABSTRACT
Focal Nodular Hyperplasia (FNH) is the second most hepatic tumor next to hemangioma predominantly affecting women. It is a benign regenerative nodule having an unencapsulated well-de- fined mass with fibrovascular septae and proliferating bile ductules. Gadoxetic acid is a hepatocyte specific MR contrast agent which is known to be specific for the identifying FNH. Congenital vascular malformation and enlargement due to hormone stimulation is being considered as the main cause of FNH. The central stellate fibrovascular scar is a typical diagnostic imaging feature of FNH and the atypical pathological findings of FNH include large lesions multiple in number, internal necrosis, haemorrhagic foci and fatty infiltration. The atypical imaging features include non- enhancement of the central scar, calcification of the lesion, nonvisualized central scar and pseudocapsular enhancement on delayed imaging. For the accurate diagnosis of FNH, study of atypical radiologic features of FNH in correlation with pathological findings is the most essential. The macroscopic and the microscopic pathognomic changes should be taken as helpful points in the diagnosis of FNH. The main objective of this study is to recognize and understand the typical and atypical imaging patterns observed in CT and MR imaging of FNH with pathological correlation which avoids the necessity of biopsy and further investigations.
Keywords:
Focal Nodular Hyperplasia (FNH), Atypical Imaging and Pathological Features, CT, MRI, Differential Diagnosis

1. Introduction
Focal Nodular Hyperplasia (FNH) is the second most benign hepatic tumor which affects both male and female, but predominantly women (80% - 95%) during third-fifth decade of life [1] [2] . FNH accounts only 2% of hepatic tumors that occurs in childhood (0 - 10 years) [3] . Gadoxetic acid, which is taken up by hepatocytes and excreted via bile duct and kidney, is a hepatocyte specific MR contrast agent which is known to be specific for the identifying FNH [4] - [6] . FNH is a benign regenerative nodule comprising disorganized growing normal hepatocytes having an unencapsulated well-defined mass with fibrovascular septae and proliferating bile ductules [7] [8] .
Congenital vascular malformation and enlargement due to hormone stimulation is being considered as the cause of FNH and the use of oral contraceptives is also to be taken in consideration as its causative association. [1] . However FNH is expected to arise as a consequence of pre-existing spider-like arterial structures with heterogenous blood flow resulting a hyperplastic hepatocyte response [7] .
The central stellate fibrovascular scar is a typical diagnostic imaging feature of FNH which accounts only about 50% of FNH lesion.
2. Pathological Findings
The atypical pathological findings of FNH; which are very rare; includes large lesions multiple in number, internal necrosis, haemorrhagic foci, fatty infiltration and the atypical imaging features includes non-enhancement of the central scar, calcification of the lesion, nonvisualized central scar, pseudocapsular enhancement on delayed imaging. Despite the advancement in imaging techniques like triple phase spiral CT and fast MR imaging, it becomes sometimes not easy to differentiate FNH because of its atypical features. So for the accurate diagnosis of FNH, study of atypical radiologic features of FNH in correlation with pathological findings is the most essential. Core needle biopsy helps in confirmatory diagnosis of FNH which shows lack of portal tracts, normal central vein and bile duct drainage with damaged normal architecture [9] .
The Macroscopic and Microscopic Findings
The macroscopic pathognomic changes like homogenous central stellate scar, radiating septa with rare presence of necrosis and hemorrhagic foci with excellent arterial blood supply; and also the microscopic pathognomic changes like fibrous septa, area of hepatocellular proliferation, fibromuscular hyperplasia, myxomatous changes with inflammatory cells should be taken as helpful points in the diagnosis of FNH [1] [2] . As FNH has no life threating complications or malignant potentials, surgical intervention or further evaluation is not needed at the time of diagnosis [2] .
3. Objective
The main objective of this study is to prevent the common and uncommon imaging patterns observed in CT and MR imaging of FNH with pathological correlation.
Generally, FNH has a solitary nodule smaller than 5 cm in diameter which is lobulated and well circumscribed without capsule [1] [2] . The presence of a central stellate scar with radiating fibrous septa, dividing the lesion into nodules of normal hepatocytes arranged abnormally is the pathognomonic macroscopic feature (Figure 1). The fibrous septae and the cellular areas of hepatocellular proliferation are the microscopic features of FNH (Figure 2).
4. Typical CT and MRI Findings
4.1. CT Findings
On unenhanced CT, FNH is seen as solitary lesion with central focal low attenuation scar surrounded by well defined homogenous area showing mass effect; the attenuation of which is similar to that of surrounding liver parenchyma. This typical feature of FNH is found in approximately 20% of patients [10] .
During the arterial phase of hepatic enhancement, FNH is homogenously enhanced (96%) with the exception of the central scar. In portal phase of hepatic enhancement, the lesion becomes iso-attenuating to the surrounding liver parenchyma but the central scar remains as low attenuated spot. Unexpectedly the central scar show enhancement in delayed phase which is due to the presence of abubdant myxomatous stroma [11] .

Figure 1. Pathology of focal nodular hyperplasia in 27-year-old women. Gross section of right lobectomy specimen shows well-circumscribed lobulated mass with central scar (arrow) and radiating septations [21] .

Figure 2. Pathology of focal nodular hyperplasia in 27-year-old woman. Photomicrograph of histopathologic specimen shows regions of nodular hepatocellular proliferation separated by radiating bands and surrounding myxomatous scar (arrows) (H and E, ×80) [21] .
4.2. MRI Findings
On T1WI, the FNH shows iso- or hypointensity (94% - 100%) and on T2WI the lesion shows hyper or isointensity (94% - 100%) and homogeneity (96%). At the same time the central scar is of decreased signal on T1WI and of increased signal (84%) on T2WI because of the bile ductules, edematous myxomatous tissue and its vascular supply [1] [12] .
Following intravenous gadolinium chelates, the whole lesion enhances expect the central scar in arterial phase but the central scar shows enhancement on delayed phase [11] .
Hepatic adenoma, which is a differential diagnosis of FNH, is distinguished from FNH by the presence of heterogenous MR SI due to intralesional hemorrhage or fat component [13] .
Also for central scar of fibrolamellar HCC is distinguished from FNH by presence of hypointense on T1WI and T2WI without definite enhancement [14] .
5. Atypical CT and MR Findings
5.1. The Size of the Tumor
Atypical presentation may be showed by the size of the tumor if the size exceeds 5 cm in diameter although majority possess the size less than 5 cm. In study by Ishak and Rabin of the 130 patients with FNH, 85% of patients was found to have a single nodule less than 5 cm in diameter, 12% had a FNH which measured between 5 and 10 cm and only 3% had the lesion greater than 10 cm. Larger tumors if measure greater than 5 cm may cause symptoms because the lesions may expand the Glisson’s capsule or cause focal mass effect on surrounding structures [15] . Large tumors may cause abdominal pain or awareness of the presence of an abdominal mass. Abdominal pain is usually caused by the expansion of the Glisson’s capsule or focal mass effect on surrounding organs or vascular structures (Figure 3).
5.2. Multiplicity of Lesions
Another parameter of FNH showing atypical presentation is multiplicity of lesions. Although mostly FNH is solitary, 22% (8 patients out of 37 patients) of FNH were found to have multiple lesions in study of Vilgrain et al. [12] . Two lesions in each of six patients, three in one patient and four in another patient were found (Figure 4 and Figure 5).
5.3. Hemorrhage and Necrosis
Some of FNH is found having hemorrhage and necrosis which are unusual findings [1] . Ischemic necrosis of FNH occurs more rarely which has been reported in 3 women who have history of oral contraceptive use [16] . Estrogens may cause vascular changes in FNH (Figure 6 and Figure 7).
5.4. Abnormal Enhancement Pattern
On Gd-EOB-DTPA-enhanced MRI, T1WI of FNH may show homogenously intense enhancement in early phase, subtle washout during the delayed phase and a low signal perfusion defect in the hepatobiliary phase

Figure 3. Large focal nodular hyperplasia in 42-year-old woman. Delayed phase contrast-enhanced CT scan shows large well-circumscribed nearly isodense mass in medial segment of left lobe of liver (black arrows). Left portal vein and hepatic artery (arrowhead) are adjacent to and displaced by the lesion. Additionally, bile ducts of segments II and VII of liver are slightly dilated (white arrows) [21] .
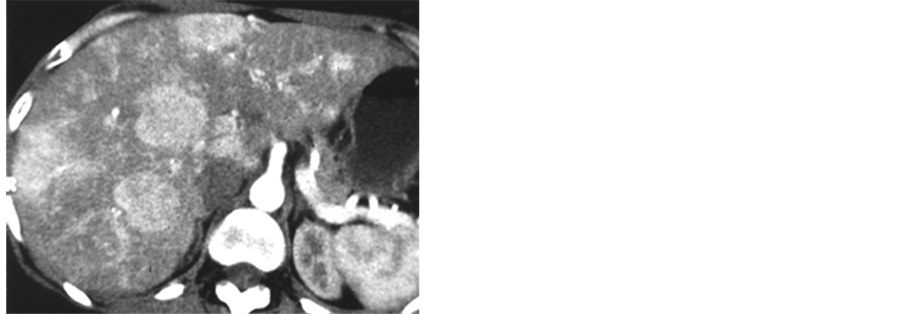
Figure 4. Multiple focal nodular hyperplasia in 28-year-old woman. Contrast-enhanced CT scan during arterial phase shows multiple hypervascular lesions disseminated throughout liver [21] .
![]()
Figure 5. Multiple focal nodular hyperplasia in 49-year-old woman. Portal venous phase gadolinium- enhanced T1-weighted MR image shows three lesions (arrows) in plane of image. Presence of enhancing central scar in smallest lesion (arrowhead) made these lesions consistent with focal nodular hyperplasia. Finding was confirmed at biopsy [21] .
![]()
Figure 6. Internal necrosis and hemorrhage in focal nodular hyperplasia in 52-year-old woman who presented with persistent abdominal pain. Arterial phase gadolinium-enhanced T1-weighted fast low- angle shot MR image shows inhomogeneous enhancement of mass with areas of necrosis present (black arrow). Note second smaller lesion (arrowhead) in right liver lobe with central scar (white arrow) [21] .
![]()
Figure 7. Internal necrosis and hemorrhage in focal nodular hyperplasia in 52-year-old woman who presented with persistent abdominal pain. Photomicrograph of histopathologic specimen of lesion shows cellular arrangement consistent with focal nodular enhancement and area of hemorrhagic necrosis (arrows) in lesion. (H and E, ×40) [21] .
which is similar to the findings of an expanding nodular HCC. Some atypical findings of FNH of patients of he patitis B may include hepatic nodule taking complete enhancement during the early arterial phase of MDCT, the delayed phase without definite washout of the contrast enhancement although the portal venous phase shows iso-attenuation with T2WI showing a high SI and mild diffusion restriction on DWI (b-factor 800) apparent different coefficient imaging with Gadoxetic acid enhanced MRI showing early intense homogenous enhancement and subtle peripheral washout during portal phase and ring like peripheral enhancement with central washout during equilibrium phase and hepatobiliary phase; which gives vague differential diagnosis like well-dif- ferentiated HCC, a high grade dysplastic nodule and hepatic adenoma. In this situation, we need to go for USG guided biopsy for confirm diagnosis [6] [17] [18] .
5.5. Intralesional Steatosis
Intralesional steatosis in FNH is thought to have association with several hepatic injury like alcoholic toxicity, obesity and protein malabsorbtion. But fatty infiltration in FNH without underlying cause has been found very rarely and has been documented only twice in the literature [19] . In earlier reports, hepatic steatosis was thought to be result of the patient’s underlying disease while describing the presence of fat in FNH (Figure 8 and Figure 9).
5.6. The Undetectable Central Scar
It is found that the central scar of FNH is undetectable on CT (16% - 40%) and on MRI (22%) due to its extremely tiny size [1] [2] [10] [12] . This non-visualized scar only can be noticed when there is deformity of liver configuration or presence of mass effects like displacement of adjacent hepatic vessels (Figure 10 and Figure 11).
5.7. Fibrous Thick Hyaline Pseudocapsule
Fibrous thick hyaline pseudocapsule surrounding FNH can be seen enhanced which is very rare [20] . The presence of pseudocapsule in FNH may suggest that underlying lesion is growing slowly, the capsule in this cases is fibrous, thick and hyaline (Figure 12 and Figure 13); however in some cases it may be confused with the eccentric compression of the lesion on hypertrophied feeding vessels.
5.8. The Nonenhanced Central Scar
In delayed phase on contrast-enhanced CT and on T1W MR, the central scar of FNH may still appear hypodense and hypointense respectively while may mimick the collagenous scar in hepatic adenoma, HCC, fibrolamellar carcinoma or intrahepatic cholagiocarcinoma [20] . After administration of constrast material, appearance of the nonenhanced central scar may be due to obliterative vascular hyperplasia of the central arteries [1] (Figure 14 and Figure 15).
![]()
Figure 8. Fatty infiltration in focal nodular hyperplasia in 47-year-old woman. Unenhanced axial CT scan shows total fatty replacement of liver and well-delineated, inhomogeneous, and hypodense mass (arrows) in right liver lobe [21] .
![]()
Figure 9. Fatty infiltration in focal nodular hyperplasia in 47-year-old woman. Photomicrograph of histopathologic specimen shows central stellate scar (large arrow) with ductular proliferation surrounded by normal and steatotic (small arrows) hepatic parenchyma. (H and E, ×40) [21] .
![]()
Figure 10. Nonvisualization of central scar in focal nodular hyperplasia of 53-year-old woman. Arterial phase contrast-enhanced CT scan shows small hypervascular lesion in right lobe of liver (arrow). No central scar is visible [21] .
![]()
Figure 11. Nonvisualization of central scar in focal nodular hyperplasia in 45-year-old man. T2- weighted half-Fourier acquisition single-shot turbo spin-echo MR image shows small isointense mass in right lobe of liver (arrows). No scar is present [21] .
![]()
Figure 12. Pseudocapsular enhancement of focal nodular hyperplasia. Delayed phase gadolinium-en- hanced T1-weighted fast low-angle shot MR image of 34-year-old woman shows isointense lesion in lateral segment of left liver lobe with marked enhancement of central scar and pseudocapsule (arrows) [21] .
![]()
Figure 13. Pseudocapsular enhancement of focal nodular hyperplasia. Low-power photomicrograph of histopathologic specimen of pseudocapsule shows prevalent stromal component (arrow) between lesion and normal parenchyma (reticulum stroma stain) [21] .
![]()
Figure 14. Nonenhancement of central scar in 48-year old woman. Contrast-enhanced CT scan shows 8cm lesion in segment IV of left lobe of liver. Centrally, 4 cm hypodense scar is shown. Nonenhancement of scar is seen either on arterial or delayed phase CT scans [21] .

Figure 15. Nonenhancement of central scar in 53-year-old man .After administration of gadopentetate dimeglumine, delayed phase (24 min) T1-weighted MR image shows gradual but incomplete enhancement of central scar (arrow) [21] .
6. Conclusion
Identification of FNH is essential for management of the lesion. The diagnosis of FNH includes both pathological and imaging features. The pathological features include macroscopic and microscopic features. The Imaging features include CT and MRI features with or without contrast enhancement. Despite the advancement in imaging modalities in recent few years, diagnosing FNH may be a challenging task if there is unexpectedly the presence of atypical imaging features of FNH, although FNH usually presents with typical imaging features. So understanding and recognizing the atypical imaging features is an important aspect for radiologist in diagnosing FNH correctly which helps to avoid the necessity of biopsy and further studies. Differentiating FNH from malignant lesions avoiding unnecessary intervention is also a valuable aspect of this review. Each of these diagnostic procedures has own limitations and clinicians should be aware of them.
Cite this paper
NarendraDarai,RongbaoShu,RajkumarGurung,XiaojuanZhang,GaojunTeng, (2015) Atypical CT and MRI Features of Focal Nodular Hyperplasia of Liver: A Study with Radiologic-Pathologic Correlation. Open Journal of Radiology,05,131-141. doi: 10.4236/ojrad.2015.53020
References
- 1. Mathieu, D., Vilgrain, V., Mahfouz, A.E., Anglade, M.C., Vullierme, M.P. and Denys, A. (1997) Benign Liver Tumors. Magnetic Resonance Imaging Clinics of North America, 5, 255-288.
- 2. Shirkhoda, A., Farah, M.C., Bernacki, E., Madrazo, B. and Roberts, J. (1994) Hepatic Focal Nodular Hyperplasia: CT and Sonographic Spectrum. Abdominal Imaging, 19, 34-38.
http://dx.doi.org/10.1007/BF02165858 - 3. Reymond, D., Plaschkes, J., Luthy, A.R., Leibundgut, K., Hirt, A. and Wagner, H.P. (1995) Focal Nodular Hyperplasia of the Liver in Children: Review of Follow-Up and Outcome. Journal of Pediatric Surgery, 30, 1590-1593. http://dx.doi.org/10.1016/0022-3468(95)90162-0
- 4. Grazioli, L., Morana, G., Federle, M.P., Brancatelli, G., Testoni, M., Kirchin, M.A., et al. (2001) Focal Nodular Hyperplasia: Morphologic and Functional Information from MR Imaging with Gadobenate Dimeglumine. Radiology, 221, 731-739. http://dx.doi.org/10.1148/radiol.2213010139
- 5. Huppertz, A., Haraida, S., Kraus, A., Zech, C.J., Scheidler, J., Breuer, J., et al. (2005) Enhancement of Focal Liver Lesions at Gadoxetic Acid-Enhanced MR Imaging: Correlation with Histopathologic Findings and Spiral CT—Initial Observations. Radiology, 234, 468-478.
http://dx.doi.org/10.1148/radiol.2342040278 - 6. Ko, K.R., Lee, D.H., Park, J.S., Yi, B.H., Lim, J.W., Ko, Y.T., et al. (2003) Focal Nodular Hyperplasia with Retraction of Liver Capsule: A Case Report. Korean Journal of Radiology, 4, 66-69.
http://dx.doi.org/10.3348/kjr.2003.4.1.66 - 7. Wanless, I.R., Mawdsley, C. and Adams, R. (1985) On the Pathogenesis of Focal Nodular Hyperplasia of the Liver. Hepatology, 5, 1194-1200. http://dx.doi.org/10.1002/hep.1840050622
- 8. Choi, J.Y., Lee, H.C., Yim, J.H., Shim, J.H., Lim, Y.S., Shin, Y.M., et al. (2011) Focal Nodular Hyperplasia or Focal Nodular Hyperplasia-Like Lesions of the Liver: A Special Emphasis on Diagnosis. Journal of Gastroenterology and Hepatology, 26, 1004-1009. http://dx.doi.org/10.1111/j.1440-1746.2011.06659.x
- 9. Rummeny, E., Weissleder, R., Sironi, S., et al. (1989) Central Scars in Primary Liver Tumors: MR Features, Specificity and Pathologic Correlation. Radiology, 171, 323-326.
http://dx.doi.org/10.1148/radiology.171.2.2539605 - 10. Shamsi, K., de Schepper, A., Degryse, H. and Deckers, F. (1993) Focal Nodular Hyperplasia of the Liver: Radiologic Findings. Abdominal Imaging, 18, 32-38. http://dx.doi.org/10.1007/BF00201698
- 11. Grandin, C.B., Van Beers, B.E., Pauwels, S., Demeure, R., Jamart, J. and Pringot, J. (1997) Ferumoxides and Tc-99m Sulfur Colloid: Comparison of the Tumor-to-Liver Uptake in Focal Nodular Hyperplasia. Journal of Magnetic Resonance Imaging, 7, 125-129. http://dx.doi.org/10.1002/jmri.1880070117
- 12. Vilgrain, V., Flejou, J.F., Arrive, L., Belghiti, J., Najmark, D., Menu, Y., et al. (1992) Focal Nodular Hyperplasia of the Liver: MR Imaging and Pathologic Correlation in 37 Patients. Radiology, 184, 699-703. http://dx.doi.org/10.1148/radiology.184.3.1509052
- 13. Shortell, C.K. and Schwartz, S.I. (1991) Hepatic Adenoma and Focal Nodular Hyperplasia. Surgery, Gynecology, and Obstetrics, 173, 426-431.
- 14. Mergo, P.J. and Ros, P.R. (1998) Benign Lesions of the Liver. Radiologic Clinics of North America, 36, 319-331. http://dx.doi.org/10.1016/S0033-8389(05)70025-7
- 15. Ishak, K.G. and Rabin, L. (1975) Benign Tumors of the Liver. Medical Clinics of North America, 59, 995-1013.
- 16. Brunt, E.M. and Flye, M.W. (1991) Infraction in Focal Nodular Hyperplasia of the Liver: A Case Report. American Journal of Clinical Pathology, 95, 503-506.
- 17. Federle, M.P. and Brancatelli, G. (2001) Imaging of Benign Hepatic Masses. Seminars in Liver Disease, 21, 237-249. http://dx.doi.org/10.1055/s-2001-15344
- 18. Trotter, J.F. and Everson, G.T. (2001) Benign Focal Lesions of the Liver. Clinics in Liver Disease, 5, 17-42. http://dx.doi.org/10.1016/S1089-3261(05)70152-5
- 19. Chaoui, A., Mergo, P.J. and Lauwers, G.Y. (1998) Unusual Appearance of Focal Nodular Hyperplasia with Fatty Change. American Journal of Roentgenology, 171, 1433-1434.
http://dx.doi.org/10.2214/ajr.171.5.9798902 - 20. Choi, C.S. and Frenny, P.C. (1998) Triphasic Helical CT of Hepatic Focal Nodular Hyperplasia: Incidence of Atypical Findings. American Journal of Roentgenology, 170, 391-395.
http://dx.doi.org/10.2214/ajr.170.2.9456952 - 21. Mortelé, K.J., Praet, M., Van Vlierberghe, H., Kunnen, M. and Ros, P.R. (2000) CT and MR Imaging Findings in Focal Nodular Hyperplasia of the Liver: Radiologic-Pathologic Correlation. American Journal of Roentgenology, 175, 687-692.
Abbreviations
FNH: Focal Nodular Hyperplasia
CT: Computed Tomography
MR: Magnetic Resonance
MRI: Magnetic Resonance Imaging
Gd-EOB-DTPA: Gadoxetic Acid
T1WI: T1 Weighted Image
T2WI: T2 Weighted Image
DWI: Diffusion Weighted Imaging
MDCT: Multi-detector Computed Tomography
HCC: Hepatocellular Carcinoma
USG: Ultrasound
NOTES

*Corresponding author.